Plantar Fascitis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

November Committee Meetings in Nashville All-CGA Committee Meetings in Nashville the All-CGA Committee Meetings, Nov
10 19 A Monthly Newsletter of the Common Ground Alliance November Committee Meetings in Nashville All-CGA Committee Meetings in Nashville The All-CGA Committee Meetings, Nov. 18-21 at the Renaissance Nashville Hotel, are just around the corner! CGA is excited to announce a new pro- plants and nonprofit associations. In gramming element at the CGA Commit- addition to co-authoring three books, tee Meetings: Dr. Victoria M. Grady will be she has recently published pieces in the general session breakfast speaker on Bloomberg News, GovExec.com, the Wednesday, Nov. 20. Journal of Change Management and The Public Manager. Dr. Grady is the Academic Director of the MSM Graduate Program and Assistant Dr. Grady’s keynote will Professor of Management/Organizational inspire damage prevention Behavior in the School of Business at professionals as we work George Mason University. Her research toward the organizational portfolio focuses on the behavioral impli- and behavioral changes cations of organizations introducing and necessary to achieve our implementing organizational change. goal of zero damages. We are looking forward We are looking for- ward to a productive to a productive week of week of meetings in meetings in Nashville. Nashville. Click here to learn more about Dr. Grady’s research includes work with CGA’s upcoming U.S. federal government agencies, private committee meet- and public healthcare organizations ings in Nashville, in the U.S. and United Kingdom, utility taking place Nov. organizations in Australia, K-12 and higher 18-21. education institutions, nuclear power October 2019 | 2 ICUEE 2019 included over 1,000 exhibitors Louisville heats up showcasing the latest products and solu- tions for the utility construction industry. -

Sport-Scan Daily Brief
SPORT-SCAN DAILY BRIEF NHL 06/07/19 Arizona Coyotes Boston Bruins cont'd 1146137 Arizona Coyotes sign defenseman Robbie Russo to 1146177 Watch Bruins fans give injured Zdeno Chara huge ovation 1-year deal before Game 5 vs. Blues 1146138 It’s safe to say that some of us are a little nuts’: Chara’s 1146178 Watch Bobby Orr, Derek Sanderson serve as Bruins' decision may add to NHL’s playoff lore Stanley Cup Game 5 banner captains 1146179 Bruins' Zdeno Chara (jaw) medically cleared to play in Boston Bruins Game 5 1146139 Painful night all around for Zdeno Chara and Bruins 1146180 Bruins' awesome Stanley Cup Game 5 hype video 1146140 Late non-call stole the show in Bruins’ Game 5 loss features Tom Brady cameo 1146141 Tyler Bozak’s apparent slew foot of Noel Acciari in Game 1146181 Bruins vs. Blues live stream: Watch 2019 Stanley Cup 5 ‘was a missed call on the biggest stage of hockey’ Final Game 5 online 1146142 Series deficit about more than officials, but Game 5 was a 1146182 Who could Bruins banner captains be for Games 5 and 7 crime of the Stanley Cup Final? 1146143 Blues beat Bruins to take 3-2 lead in Stanley Cup Final 1146183 Bruins' scoreless second line has to 'have more of an 1146144 Non-call on third-period trip hard to ignore after 2-1 loss attack mentality' 1146145 Zdeno Chara joins a stellar list of those who played in pain 1146184 ‘It’s safe to say that some of us are a little nuts’: Chara’s 1146146 Bruins’ Matt Grzelcyk out for Game 5 of Stanley Cup Final decision may add to NHL’s playoff lore 1146147 NBC’s Patrick Sharp knows -

2017-18 COLORADO BASKETBALL Colorado Buffaloes
colorado buffaloes All-America Selections Jack Harvey Robert Doll 1939 & 1940 1942 In his back-to-back All- Bob Doll was the big-play man for America campaigns, Jack coach Frosty Cox’s 1941-42 Big Seven Harvey led the Buffs to two Championship squad. Doll, along with conference championships fellow All-American Leason McCloud and a trip to the NCAA helped lead CU to a 16-2 record and Tournament in his senior the NCAA Western Tournament finals season. During those as a senior. He scored 168 points (9.4 two years, CU posted an ppg.) and was known as an outstanding amazing 31-8 mark and rebounder and controlled the paint in received recognition as many CU wins. He was also renowned the No. 1 team in the for his shooting prowess, finishing second land. Known for his tough to McCloud in scoring. An unanimous All- defense, Harvey proved to Big Seven selection, Doll was selected to be key in numerous Buff All-America teams by Look, Pic and Time victories. He was also an magazines. He was also tabbed as MVP of outstanding ball-handler for New York’s Metropolitan Tournament as a a big man and was a key sophomore and was a huge factor in CU’s component in the CU fast three conference titles in a four-year span. break. A solid All-Conference After graduation, Doll went on to play for performer, Harvey is the the Boston Celtics. only CU cager to be selected twice as an All-American Leason McCloud 1942 Jim Willcoxon The leading scorer for the 1939 1942 Big Seven Champion Buffs, Known for his defense, Leason McCloud was Coach Frosty Jim Willcoxon continued Cox’s “go-to guy.” Known for his Coach Frosty Cox’s tradition silky-smooth shot, McCloud was of talented cagers. -

The Olympics Are As Much an Exercise in Patriotism As They Are An
OLYMPICS | LONDON 2012 America's Best Moments he Olympics are as much an exercise in patriotism as they Tare an individual achievement. It just feels good to root for athletes from your own country. The United States is fortunate to have some of the most thrilling victories in the THE DREAM TEAM history of summer Olympics. Here's a look Widely considered the at a few of them. most talented Olympic team to compete in any sport, the 1992 United States men's JESSE OWENS Olympic basketball team Adolf Hitler had plans to make the 1936 consisted of the biggest Olympic games a demonstration of the stars in the National superiority of the Aryan race. Basketball Association. Jesse Owens had other ideas. Consisting entirely of bas- Owens, a black man from America, won ketball icons — including four different gold medals in Berlin in one Michael Jordan, David of history's greatest athletic accomplish- Robinson, Patrick Ewing, ments. It would take nearly 50 years — Larry Bird, Scottie until the 1984 games — before any runner Pippen, Clyde Drexler, equaled his Olympic four-gold-medal per- Karl Malone, Charles formance. Barkley and Magic Hitler is said to have been embarrassed Johnson — the Dream that a non-German could dominate the Team soundly defeated Berlin games so completely. Owens showed every opponent in the that it's talent and training, not a particular games. set of genetics, that leads to victory. They beat their com- petition by an average of 43 points per game, MARY LOU RETTON making it look easy to In 1984, when the Cold War was still sim- win a gold medal. -

Renormalizing Individual Performance Metrics for Cultural Heritage Management of Sports Records
Renormalizing individual performance metrics for cultural heritage management of sports records Alexander M. Petersen1 and Orion Penner2 1Management of Complex Systems Department, Ernest and Julio Gallo Management Program, School of Engineering, University of California, Merced, CA 95343 2Chair of Innovation and Intellectual Property Policy, College of Management of Technology, Ecole Polytechnique Federale de Lausanne, Lausanne, Switzerland. (Dated: April 21, 2020) Individual performance metrics are commonly used to compare players from different eras. However, such cross-era comparison is often biased due to significant changes in success factors underlying player achievement rates (e.g. performance enhancing drugs and modern training regimens). Such historical comparison is more than fodder for casual discussion among sports fans, as it is also an issue of critical importance to the multi- billion dollar professional sport industry and the institutions (e.g. Hall of Fame) charged with preserving sports history and the legacy of outstanding players and achievements. To address this cultural heritage management issue, we report an objective statistical method for renormalizing career achievement metrics, one that is par- ticularly tailored for common seasonal performance metrics, which are often aggregated into summary career metrics – despite the fact that many player careers span different eras. Remarkably, we find that the method applied to comprehensive Major League Baseball and National Basketball Association player data preserves the overall functional form of the distribution of career achievement, both at the season and career level. As such, subsequent re-ranking of the top-50 all-time records in MLB and the NBA using renormalized metrics indicates reordering at the local rank level, as opposed to bulk reordering by era. -

Michael Jordan: a Biography
Michael Jordan: A Biography David L. Porter Greenwood Press MICHAEL JORDAN Recent Titles in Greenwood Biographies Tiger Woods: A Biography Lawrence J. Londino Mohandas K. Gandhi: A Biography Patricia Cronin Marcello Muhammad Ali: A Biography Anthony O. Edmonds Martin Luther King, Jr.: A Biography Roger Bruns Wilma Rudolph: A Biography Maureen M. Smith Condoleezza Rice: A Biography Jacqueline Edmondson Arnold Schwarzenegger: A Biography Louise Krasniewicz and Michael Blitz Billie Holiday: A Biography Meg Greene Elvis Presley: A Biography Kathleen Tracy Shaquille O’Neal: A Biography Murry R. Nelson Dr. Dre: A Biography John Borgmeyer Bonnie and Clyde: A Biography Nate Hendley Martha Stewart: A Biography Joann F. Price MICHAEL JORDAN A Biography David L. Porter GREENWOOD BIOGRAPHIES GREENWOOD PRESS WESTPORT, CONNECTICUT • LONDON Library of Congress Cataloging-in-Publication Data Porter, David L., 1941- Michael Jordan : a biography / David L. Porter. p. cm. — (Greenwood biographies, ISSN 1540–4900) Includes bibliographical references and index. ISBN-13: 978-0-313-33767-3 (alk. paper) ISBN-10: 0-313-33767-5 (alk. paper) 1. Jordan, Michael, 1963- 2. Basketball players—United States— Biography. I. Title. GV884.J67P67 2007 796.323092—dc22 [B] 2007009605 British Library Cataloguing in Publication Data is available. Copyright © 2007 by David L. Porter All rights reserved. No portion of this book may be reproduced, by any process or technique, without the express written consent of the publisher. Library of Congress Catalog Card Number: 2007009605 ISBN-13: 978–0–313–33767–3 ISBN-10: 0–313–33767–5 ISSN: 1540–4900 First published in 2007 Greenwood Press, 88 Post Road West, Westport, CT 06881 An imprint of Greenwood Publishing Group, Inc. -
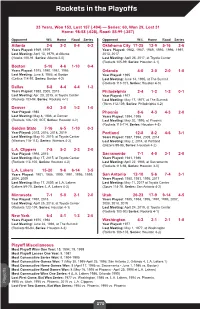
Rockets in the Playoffs
Rockets in the Playoffs 33 Years, Won 153, Lost 157 (.494) — Series: 60, Won 29, Lost 31 Home: 98-58 (.628), Road: 55-99 (.357) Opponent W-L Home Road Series Opponent W-L Home Road Series Atlanta 2-6 2-2 0-4 0-2 Oklahoma City 17-25 12-9 5-16 2-6 Years Played: 1969, 1979 Years Played: 1982, 1987, 1989, 1993, 1996, 1997, Last Meeting: April 13, 1979, at Atlanta 2013, 2017 (Hawks 100-91, Series: Atlanta 2-0) Last Meeting: April 25, 2017, at Toyota Center (Rockets 105-99, Series: Houston 4-1) Boston 5-16 4-6 1-10 0-4 Years Played: 1975, 1980, 1981, 1986 Orlando 4-0 2-0 2-0 1-0 Last Meeting: June 8, 1986, at Boston Year Played: 1995 (Celtics 114-97, Series: Boston 4-2) Last Meeting: June 14, 1995, at The Summit (Rockets 113-101, Series: Houston 4-0) Dallas 8-8 4-4 4-4 1-2 Years Played: 1988, 2005, 2015 Philadelphia 2-4 1-2 1-2 0-1 Last Meeting: Apr. 28, 2015, at Toyota Center Year Played: 1977 (Rockets 103-94, Series: Rockets 4-1) Last Meeting: May 17, 1977, at The Summit (76ers 112-109, Series: Philadelphia 4-2) Denver 4-2 3-0 1-2 1-0 Year Played: 1986 Phoenix 8-6 4-3 4-3 2-0 Last Meeting: May 8, 1986, at Denver Years Played: 1994, 1995 (Rockets 126-122, 2OT, Series: Houston 4-2) Last Meeting: May 20, 1995, at Phoenix (Rockets 115-114, Series: Houston 4-3) Golden State 7-16 6-5 1-10 0-3 Year Played: 2015, 2016, 2018, 2019 Portland 12-8 8-2 4-6 3-1 Last Meeting: May 10, 2019, at Toyota Center Years Played: 1987, 1994, 2009, 2014 (Warriors 118-113), Series: Warriors 4-2) Last Meeting: May 2, 2014, at Portland (Blazers 99-98, Series: Houston 4-2) L.A. -

Prices Realized
SPRING 2014 PREMIER AUCTION PRICES REALIZED Lot# Title Final Price 1 C.1850'S LEMON PEEL STYLE BASEBALL (NSM COLLECTION) $2,421.60 2 1880'S FIGURE EIGHT STYLE BASEBALL (NSM COLLECTION) $576.00 3 C.1910 BASEBALL STITCHING MACHINE (NSM COLLECTION) $356.40 4 HONUS WAGNER SINGLE SIGNED BASEBALL W/ "FORMER PIRATE" NOTATION (NSM COLLECTION) $1,934.40 ORIGINAL INVITATION AND TICKET TO JUNE 30TH, 1909 FORBES FIELD (PITTSBURGH) OPENING GAME AND 5 DEDICATION CEREMONY (NSM COLLECTION) $7,198.80 ORIGINAL INVITATION AND TICKET TO JUNE 30TH, 1910 FORBES FIELD OPENING GAME AND 1909 WORLD 6 CHAMPIONSHIP FLAG RAISING CEREMONY (NSM COLLECTION) $1,065.60 1911 CHICAGO CHAMPIONSHIP SERIES (WHITE SOX VS. CUBS) PRESS TICKET AND SCORERS BADGE AND 1911 COMISKEY 7 PARK PASS (NSM COLLECTION) $290.40 ORIGINAL INVITATION AND TICKET TO MAY 16TH, 1912 FENWAY PARK (BOSTON) OPENING GAME AND DEDICATION 8 CEREMONY (NSM COLLECTION) $10,766.40 ORIGINAL INVITATION AND TICKET TO APRIL 18TH, 1912 NAVIN FIELD (DETROIT) OPENING GAME AND DEDICATION 9 CEREMONY (NSM COLLECTION) $1,837.20 ORIGINAL INVITATION TO AUGUST 18TH, 1915 BRAVES FIELD (BOSTON) OPENING GAME AND 1914 WORLD 10 CHAMPIONSHIP FLAG RAISING CEREMONY (NSM COLLECTION) $939.60 LOT OF (12) 1909-1926 BASEBALL WRITERS ASSOCIATION (BBWAA) PRESS PASSES INCL. 6 SIGNED BY WILLIAM VEECK, 11 SR. (NSM COLLECTION) $580.80 12 C.1918 TY COBB AND HUGH JENNINGS DUAL SIGNED OAL (JOHNSON) BASEBALL (NSM COLLECTION) $11,042.40 13 CY YOUNG SINGLE SIGNED BASEBALL (NSM COLLECTION) $42,955.20 1929 CHICAGO CUBS MULTI-SIGNED BASEBALL INCL. ROGERS HORNSBY, HACK WILSON, AND KI KI CUYLER (NSM 14 COLLECTION) $528.00 PHILADELPHIA A'S GREATS; CONNIE MACK, CHIEF BENDER, EARNSHAW, EHMKE AND DYKES SIGNED OAL (HARRIDGE) 15 BASEBALL (NSM COLLECTION) $853.20 16 BABE RUTH AUTOGRAPHED 1948 FIRST EDITION COPY OF "THE BABE RUTH STORY" (NSM COLLECTION) $7,918.80 17 BABE RUTH AUTOGRAPHED BASEBALL (NSM COLLECTION) $15,051.60 18 DIZZY DEAN SINGLE SIGNED BASEBALL (NSM COLLECTION) $1,272.00 1944 & 1946 WORLD CHAMPIONSHIP ST. -

Professional Sports Leagues and the First Amendment: a Closed Marketplace Christopher J
Marquette Sports Law Review Volume 13 Article 5 Issue 2 Spring Professional Sports Leagues and the First Amendment: A Closed Marketplace Christopher J. McKinny Follow this and additional works at: http://scholarship.law.marquette.edu/sportslaw Part of the Entertainment and Sports Law Commons Repository Citation Christopher J. McKinny, Professional Sports Leagues and the First Amendment: A Closed Marketplace, 13 Marq. Sports L. Rev. 223 (2003) Available at: http://scholarship.law.marquette.edu/sportslaw/vol13/iss2/5 This Comment is brought to you for free and open access by the Journals at Marquette Law Scholarly Commons. For more information, please contact [email protected]. COMMENTS PROFESSIONAL SPORTS LEAGUES AND THE FIRST AMENDMENT: A CLOSED MARKETPLACE 1. INTRODUCTION: THE CONTROVERSY Get murdered in a second in the first degree Come to me with faggot tendencies You'll be sleeping where the maggots be... Die reaching for heat, leave you leaking in the street Niggers screaming he was a good boy ever since he was born But fluck it he gone Life must go on Niggers don't live that long' Allen Iverson, 2 a.k.a. "Jewelz," 3 from the song "40 Bars." These abrasive lyrics, quoted from Allen Iverson's rap composition "40 Bars," sent a shock-wave of controversy throughout the National Basketball 1. Dave McKenna, Cheap Seats: Bum Rap, WASH. CITY PAPER, July 6-12, 2001, http://www.washingtoncitypaper.com/archives/cheap/2001/cheap0706.html (last visited Jan. 15, 2003). 2. Allen Iverson, a 6-foot, 165-pound shooting guard, currently of the Philadelphia 76ers, was born June 7, 1975 in Hampton, Virginia. -

2014 Americana Men of the Year Are Both Cypress College Alumni, NBA Standouts
PUBLIC INFORMATION OFFICE Contact: Marc S. Posner FOR IMMEDIATE RELEASE (714) 484-7006 February 19, 2014 [email protected] 14-02 2014 Americana Men of the Year are Both Cypress College Alumni, NBA Standouts Two Cypress College alumni — Swen Nater and Mark Eaton — will be honored as the 2014 Americana Awards Men of the Year. Both men played for legendary Cypress College basketball coaches Don Johnson (for whom the college’s court is named) and Tom Lubin before continuing to successful careers in the National Basketball Association. Neither was playing basketball when Assistant Coach Lubin discovered, recruited, mentored, and trained them outside team practices. After completing their studies at Cypress College, both played at the University of California at Los Angeles. Not only did both Nater and Eaton play in the NBA, each still holds league records. The Cypress College Foundation’s 39th Annual Americana Awards. The Americana Awards, sponsored by Union Bank, N.A., will be held on Saturday, February 22, 2014 in the Disneyland Hotel’s Grand Ballroom. Nater started playing basketball in 1969 as a freshman at Cypress College—thanks directly to the effort Lubin. When he first went out for the team he did not own a pair of tennis shoes. He didn’t play much that first year but became an All-American in his second season and was recruited to play at UCLA for the legendary John Wooden. He went on to play in the American Basketball Association, where he was named Rookie of the Year, and then the NBA. He’s the only player to have led both the ABA and the NBA in rebounding. -
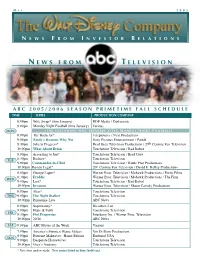
N E W S F R O M T E L E V I S I O N
M A Y 2 0 0 5 N E W S F R O M I N V E S T O R R E L A T I O N S N E W S F R O M T E L E V I S I O N A B C 2 0 0 5 / 2 0 0 6 S E A S O N P R I M E T I M E F A L L S C H E D U L E TIME SERIES PRODUCTION COMPANY 8:00pm Wife Swap* (thru January) RDF Media / Diplomatic 9:00pm Monday Night Football (thru January) Various MON ( T H E F O L L O W I N G W I L L P R E M I E R E A F T E R M O N D A Y N I G H T F O O T B A L L ) 8:00pm The Bachelor* Telepictures / Next Productions 9:00pm Emily’s Reasons Why Not Sony Pictures Entertainment / Pariah 9:30pm Jake in Progress* Brad Grey Television Productions / 20th Century Fox Television 10:00pm What About Brian Touchstone Television / Bad Robot 8:00pm According to Jim* Touchstone Television / Brad Grey 8:30pm Rodney* Touchstone Television TUE 9:00pm Commander-in-Chief Touchstone Television / Battle Plan Productions 10:00pm Boston Legal* 20th Century Fox Television / David E. Kelley Productions 8:00pm George Lopez* Warner Bros. Television / Mohawk Productions / Fortis Films 8:30pm Freddie Warner Bros. Television / Mohawk Productions / The Firm WED 9:00pm Lost* Touchstone Television / Bad Robot 10:00pm Invasion Warner Bros. -
Passion to Profession JMU Alumnus Captures the Stories of Sports Stars
FAREWELL FROM OUR FAVES Departing editors reflect on their time with The Breeze OPINION | 5 NEWS CHASING CARS ARTS THROWING SHADE Capstone project tests fuel Kendrick Lamar releases new 3 efficiency 8 hip-hop song Vol. 95, No. 26 Thursday, March 30, 2017 breezejmu.org JMU purchases most of neighborhood for over $4 million By MATT D’ANGELO purchased to provide JMU faculty and staff AND MIKE DOLZER with the opportunity to rent homes from The Breeze the university, and that there are currently no long-term plans for the area. Soft, fluttering wind chimes could be “Anytime a property becomes available heard as Carmenza Kline looked around that’s sort of contiguous to campus,” Wyatt in the backyard she’s called home for said, “we’ll consider, ‘Do we have a need almost 50 years. for it?’” “My children grew up here; I planted No student at JMU is foreign to the all the trees here. It’s my home; it’s my idea that the univer sity is growing. In the home and I don’t want to see my home, past four years, the university has turned you know, go and become a building … it UREC into an almost 300,000 square- means a lot,” Kline said. foot colossus; the Student Success Center Kline, 71, is one of two independent has cemented itself in the JMU skyline; homeowners in the Forest Hills D-Hall’s massive exoskeleton is under neighborhood, a development tucked construction behind Wilson Hall; the Grace away among the Edith J. Carrier Street corridor has been transformed into Arboretum, Forest Hills Manor and a route peppered with JMU buildings and Interstate 81.