Serum Diamine Oxidase in Pseudoallergy in the Pediatric Population
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Headache Is One of the Most Common Complaints Voiced in a Doctor's
Headache is one of the most common complaints voiced in a doctor’s examination room. Many of these headaches are "benign" in the sense that they are brought on by stress or anxiety, the amount of discomfort is mild to moderate, and relief is achieved withi n a few hours. A second type of headache occurs secondary to a medical illnesses, usually a minor condition such as the flu. Only in rare cases are these headaches a sign of serious conditions such as cerebral aneurysms or strokes. A third type of headache , affecting 10 - 20% of the population, is a migraine (1). Migraines consist of periodic attacks of hemicranial pain, vomiting, photophobia, phonophobia, tiredness, irritability, and impaired concentration. In the case of a classical migraine, the headache itself is preceded by an "aura" consisting of visual problems, generally blind spots or hallucinations. A common migraine contains no premonitory aura (2). Several hypothesis have been proposed to account for the various features of a migraine, yet no cle ar mechanism exists to explain why or how a migraine headache occurs. Certain foods, such as chocolate, wine, and cheese, have been suspected of initiating migraines. It is the purpose of this paper to evaluate the evidence for dietary triggers of migraine s, suggest a mechanism by which specific molecules in food could induce a migraine, and make recommendations regarding dietary treatment for migraine sufferers. Research on the Role of Food in Migraine Headaches Studies implicating food in the pathogene sis of migraines date back to the 1920’s when researchers began to examine and manipulate the diets of individuals suffering from migraines. -
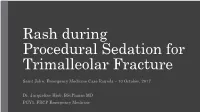
Rash During Procedural Sedation for Trimalleolar Fracture
Rash during Procedural Sedation for Trimalleolar Fracture Saint John, Emergency Medicine Case Rounds – 10 October, 2017 Dr. Jacqueline Hiob, BScPharm MD PGY1, FRCP Emergency Medicine Learning points for discussion around… • Response to possible drug reaction during procedural sedation • Options for avoiding or mitigating histamine release reactions to opioids Case 14 y/o M, healthy Fall from bicycle ~ 1 hour prior to presentation to ED No head injury, no LOC c/o pain and swelling R. ankle Unable to ambulate Transport by EMS – pt splinted on route, extremity NVI, Entonox for analgesia Case In the ED…. - Entonox Acetaminophen, Fentanyl - closed R. ankle injury, remains NVI - BP 145/72, P 90, S 96% RA, T 36.8 - off to xray he goes…. Imaging - Comminuted fractures, distal tibia + fibula - Apex medial and posterior angulation - Ankle and growth plate intact Case - Ortho consulted - Ortho R3 arrives in ED to assist with reduction - Full team: ED attending, ED resident, Emerg CC3, Ortho resident, RN, RN (training), RT, RT (student), LPN, X-Ray Tech Case Balanced Procedural Sedation with…. - Fentanyl - Ketamine - Propofol Case - ~ 20 minutes into procedure, macular rash noted over patients chest, progressing over abdomen - - no airway involvement, no hypotension or tachycardia - - decision made to treat with IV diphenhydramine and have epinephrine on hand ** smaller area of involvement than pictured - meds for anaphylaxis not immediately available and nurse sent to retrieve Case - Reduction completed within few minutes of rash presentation - Rash -
Blood Cell Changes in Complement Activation- Related Pseudoallergy
Eur. J. Nanomed. 2015; 7(3): 233–244 Mini Review Zsófia Patkó* and János Szebeni Blood cell changes in complement activation- related pseudoallergy DOI 10.1515/ejnm-2015-0021 Introduction Received April 13, 2015; accepted May 19, 2015 Complement activation-related pseudoallergy (CARPA), as the name implies, is a non-Ig-E-mediated (pseudo- Abstract: The characteristic physiological changes allergic) hypersensitivity reaction (HSR) that is triggered in complement (C) activation-related pseudoallergy by C activation, or C activation plays a major contributing (CARPA) include thrombocytopenia, leukocytosis and role. CARPA is best known in the context of nanotoxicity, leukopenia with or without compensatory leukocytosis. since nanomedicines, i.e. particulate drugs and agents in In the background of these phenomena it is known that the nano (10−9–10 −6 m) size range often cause such reac- anaphylatoxins, the triggers of CARPA, can activate white tions. As reviewed earlier (1–8), and also discussed in blood cells (WBCs) and platelets, and that this activation other papers of this issue, the phenomenon represents can lead to the binding of these cells to each other and an immune barrier to the clinical use of many promising also to capillary endothelial cells, entailing microthrom- nanomedicines. In essence, CARPA may be perceived as bus formation and circulatory blockage mainly in the pul- a biological stress on blood that arises as a consequence monary and coronary microcirculation. These changes of the similarity of nanomedicines to viruses, between are key contributors to the hemodynamic alterations in which the immune system cannot make difference (8). CARPA, and can lead to anaphylactic shock. -

Histamine and Gut Mucosal Immune Regulation S
Allergy REVIEW ARTICLE Histamine and gut mucosal immune regulation S. Smolinska1,2, M. Jutel1,2, R. Crameri3 & L. O’Mahony3 1Department of Clinical Immunology, Wroclaw Medical University, Wroclaw; 2‘ALL-MED’ Medical Research Institute, Wroclaw, Poland; 3Swiss Institute of Allergy and Asthma Research, University of Zurich, Davos, Switzerland To cite this article: Smolinska S, Jutel M, Crameri R, O’Mahony L. Histamine and gut mucosal immune regulation. Allergy 2013; DOI: 10.1111/all.12330. Keywords Abstract allergy; histamine; inflammation; microbial Histamine is a biogenic amine with extensive effects on many cell types, mediated metabolites; mucosal immunology. by the activation of its four receptors (H1R–H4R). Distinct effects are dependent Correspondence on receptor subtypes and their differential expression. Within the gastrointestinal Dr. Liam O’Mahony, SIAF, Obere Strasse tract, histamine is present at relatively high concentrations, particularly during 22, 7270 Davos Platz, Switzerland. inflammatory responses. In this review, we discuss the immunoregulatory influ- Tel.: +41-81-4100853 ence of histamine on a number of gastrointestinal disorders, including food Fax: +41-81-4100840 allergy, scombroid food poisoning, histamine intolerance, irritable bowel syn- E-mail: [email protected] drome, and inflammatory bowel disease. It is clear that the effects of histamine on mucosal immune homeostasis are dependent on expression and activity of the Accepted for publication 21 October 2013 four currently known histamine receptors; however, the relative protective or pathogenic effects of histamine on inflammatory processes within the gut are still DOI:10.1111/all.12330 poorly defined and require further investigation. Edited by: Hans-Uwe Simon Histamine [2-(4-imidazolyl)-ethylamine] is a short-acting studies demonstrate the influence of histamine on wound endogenous amine, which is widely distributed throughout healing, circulatory disease, immunology, oncology, and the body (1, 2). -

Food Allergy and Intolerance: a Narrative Review on Nutritional Concerns
nutrients Review Food Allergy and Intolerance: A Narrative Review on Nutritional Concerns Domenico Gargano 1,†, Ramapraba Appanna 2,†, Antonella Santonicola 2 , Fabio De Bartolomeis 1, Cristiana Stellato 2, Antonella Cianferoni 3, Vincenzo Casolaro 2 and Paola Iovino 2,* 1 Allergy and Clinical Immunology Unit, San Giuseppe Moscati Hospital, 83100 Avellino, Italy; [email protected] (D.G.); [email protected] (F.D.B.) 2 Department of Medicine, Surgery and Dentistry “Scuola Medica Salernitana”, University of Salerno, 84081 Baronissi, Italy; [email protected] (R.A.); [email protected] (A.S.); [email protected] (C.S.); [email protected] (V.C.) 3 Division of Allergy and Immunology, The Children’s Hospital of Philadelphia, Perelman School of Medicine at University of Pennsylvania, Philadelphia, PA 19104, USA; [email protected] * Correspondence: [email protected]; Tel.: +39-335-7822672 † These authors contributed equally to this work. Abstract: Adverse food reactions include immune-mediated food allergies and non-immune-mediated intolerances. However, this distinction and the involvement of different pathogenetic mechanisms are often confused. Furthermore, there is a discrepancy between the perceived vs. actual prevalence of immune-mediated food allergies and non-immune reactions to food that are extremely common. The risk of an inappropriate approach to their correct identification can lead to inappropriate diets with severe nutritional deficiencies. This narrative review provides an outline of the pathophysiologic and clinical features of immune and non-immune adverse reactions to food—along with general Citation: Gargano, D.; Appanna, R.; diagnostic and therapeutic strategies. Special emphasis is placed on specific nutritional concerns for Santonicola, A.; De Bartolomeis, F.; each of these conditions from the combined point of view of gastroenterology and immunology, in Stellato, C.; Cianferoni, A.; Casolaro, an attempt to offer a useful tool to practicing physicians in discriminating these diverging disease V.; Iovino, P. -

5 Allergic Diseases (And Differential Diagnoses)
Chapter 5 5 Allergic Diseases (and Differential Diagnoses) 5.1 Diseases with Possible IgE Involve- tions (combination of type I and type IVb reac- ment (“Immediate-Type Allergies”) tions). Atopic eczema will be discussed in a separate section (see Sect. 5.5.3). There are many allergic diseases manifesting in The maximal manifestation of IgE-mediated different organs and on the basis of different immediate-type allergic reaction is anaphylax- pathomechanisms (see Sect. 1.3). The most is. In the development of clinical symptoms, common allergies develop via IgE antibodies different organs may be involved and symp- and manifest within minutes to hours after al- toms of well-known allergic diseases of skin lergen contact (“immediate-type reactions”). and mucous membranes [also called “shock Not infrequently, there are biphasic (dual) re- fragments” (Karl Hansen)] may occur accord- action patterns when after a strong immediate ing to the severity (see Sect. 5.1.4). reactioninthecourseof6–12harenewedhy- persensitivity reaction (late-phase reaction, LPR) occurs which is triggered by IgE, but am- 5.1.1 Allergic Rhinitis plified by recruitment of additional cells and 5.1.1.1 Introduction mediators.TheseLPRshavetobedistin- guished from classic delayed-type hypersensi- Apart from being an aesthetic organ, the nose tivity (DTH) reactions (type IV reactions) (see has several very interesting functions (Ta- Sect. 5.5). ble 5.1). It is true that people can live without What may be confusing for the inexperi- breathing through the nose, but disturbance of enced physician is familiar to the allergist: The this function can lead to disease. Here we are same symptoms of immediate-type reactions interested mostly in defense functions against are observed without immune phenomena particles and irritants (physical or chemical) (skin tests or IgE antibodies) being detectable. -

Drug Allergies & Cross-Sensitivities
DRUG ALLERGIES & CROSS-SENSITIVITIES A Presentation for HealthTrust Members June 2, 2020 Vasyl Zbyrak, PharmD, PGY-1Pharmacy Resident Saint Barnabas Medical Center Kristine A. Sobolewski, PharmD, BCPS, Preceptor 2 Speaker & Preceptor Disclosures The presenter and his preceptor have no real or perceived conflicts of interest related to this presentation. Note: This program may contain the mention of suppliers, brands, products, services or drugs presented in a case study or comparative format using evidence-based research. Such examples are intended for educational and informational purposes and should not be perceived as an endorsement of any particular supplier, brand, product, service or drug. 3 Learning Objectives Pharmacists & Nurses: Distinguish the different drug class allergies and their mechanism of action Describe the most common drug allergies and characteristics of an allergic reaction Recommend alternative treatment options based on the drug allergy profile while evaluating the potential risk for the patient 4 Learning Objectives Pharmacy Technicians Identify the characteristics of an allergic reaction and common drug allergies Recognize the names of potentially inappropriate medications based on allergies and cross-sensitivities 5 Patient Case JG is 62 YO female presenting to the ED with pain 9/10. Patient was ordered morphine 4 mg IV push. Pain was relieved, but a rash appeared on her face with some flushing. Patient is not complaining of any other symptoms or shortness of breath. 6 Is the patient experiencing a drug allergy? 7 Adverse Drug Reactions A general term utilized to encompass any unwanted reaction to a medication and are broadly divided into Type A and B reactions Type A Type B • Reactions occurring in most • Drug hypersensitivity that is patients that are common relatively uncommon, rare and predictable and mostly unpredictable • Involves potential overdose, • Involves intolerances, side effects and drug idiosyncrasy, pseudoallergy interactions and drug allergies Source: Celik G, et al. -

Review of Intolerance Reactions to Food and Food Additives
International Food Risk Analysis Journal Review of Intolerance Reactions to Food and Food Additives Hikmat Hayder*, Utz Mueller and Andrew Bartholomaeus Risk Assessment Branch, Food Standards Australia New Zealand * Corresponding author E-mail: [email protected] Received 14 September 2011; final version received 7 November 2011 © 2011 Hayder et al.; licensee InTech. This is an open access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract There is ongoing interest in the community in perceived to be a major cause of intolerance reactions in the area of intolerance reactions to food and food the community. However, except for sulphites, clinical additives. To inform future discussions on this subject, evidence of a causal link between food additives and FSANZ initiated a scientific review to give further intolerance reactions is limited, and the frequency, consideration to key issues underpinning the public severity and spectrum of symptoms are yet to be debate. This paper provides an overview of the determined. contemporary understanding of food intolerance, and highlights the individual nature of intolerance reactions In Australia and New Zealand, the approval of food and the wide range of food chemicals, whether naturally additives follows a rigorous process based on two occurring or added to food, which may contribute to principles: the additive must fulfil a technological intolerance reactions. The clinical manifestations of function, and must not pose a safety concern to intolerance described in the literature vary widely, both consumers at the proposed level of use. -

4/6/2016 1 Drug Allergy: Focus on Antibiotics
4/6/2016 Drug Allergy: Focus on Antibiotics Jonathan Grey, Pharm.D. Clinical Coordinator/Antibiotic Stewardship Specialist Morton Plant Mease Healthcare April 9th, 2016 Disclosure Information I have no actual or potential conflict of interest in relation to this presentation Objectives By the end of this presentation, you should be able to: Classify the different types of drug hypersensitivity and explain the various strategies for drug avoidance based on these classifications Describe the risk of cross sensitivity between the antibiotic classes, including the role of R1 side chains in determining β-lactam cross sensitivity Delineate between the different roles of antibiotic desensitization, direct/graded challenges, and antibiotic skin testing in response to a patient with a reported allergy Discuss the significance of some non- β-lactam drug allergies and their impact on patient care 1 4/6/2016 Predictable Drug Reactions Predictable Dose dependent Related to pharmacologic action Occur in otherwise healthy individuals i.e. Dizziness with BP meds, hypoglycemia with insulin Unpredictable Drug Reactions Drug • Undesirable effect intolerance • Low doses • Normal metabolism, excretion, bioavailability • i.e. ASA tinnitis Drug • Abnormal, unexpected idiosyncrasy • Underlying abnormality of metabolism, excretion bioavailability • i.e. Dapsone hemolytic anemia Drug allergy • Immune mediated • Drug specific antibodies, T cells, or both • i.e. penicillin rash Pseudoallergy • Mimic anaphylaxis • No sensitization period, can occur with -

Histamine December 2013
Histamine December 2013 Introduction Histamine, an imidoamine synthesised metabolically from the decarboxylation of histidine, is a vasoactive amine of the gut and the immune system. It also acts as a neurotransmitter in the central nervous system and as a chemotactic agent for leucocytes. After synthesis, histamine may be broken down or stored in an inactive protein-bound form, primarily in the blood basophils or the pulmonary mast cells. Histamine exerts its actions by combining with one of four specific cell receptors, designated H1, H2, H3 and H4 [1]. Studies of allergic disease have shown that histamine release plays a central role in the pathogenesis of the early-phase allergic response. High histamine production and release is associated with allergic responses, particularly type 1 (immediate hypersensitivity) reactions [2], which are mediated by IgE antibodies. Excess histamine may also be responsible for immediate hypersenstivity reactions that are not associated with IgE antibodies, such as the symptoms of scombroid fish poisoning [3]. Gastric enterochromaffin-like cells and histaminergic nerves in the brain are also sources of histamine. Histamine receptors Histamine receptors are members of the 7-transmembrane-spanning family of receptors that couple ligand binding to intracellular reactions through interactions with guanosine triphosphate-binding heterotrimeric proteins [1]. The significance of histamine release is essentially defined by the cell types that express histamine receptors. There are four classes of histamine receptor. The H1 histamine receptor is widely distributed throughout smooth muscle, the vascular endothelium and the nervous system, as well as endothelial cells, neutrophils, eosinophils, monocytes and dendritic cells. Activation of the H1 receptor causes symptoms such as vasodilation, bronchoconstriction, smooth muscle activation and itching, as well as intracellular events characterized by changes in free cytosolic calcium concentration and by elevations in cyclic adenosine monophosphate (cAMP). -

The Role of Allergens and Pseudoallergens in Urticaria
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector The Role of Allergens and Pseudoallergens in Urticaria Torsten Zuberbier Department of Dermatology and Allergy, ChariteÂ, Humboldt University, Berlin, Germany Adverse reactions to food are a frequently discussed urticaria pseudoallergic reactions against NSAID are cause of urticaria. In acute urticaria 63% of patients responsible for approximately 9% of cases, and in a suspect food as the eliciting factor; however, this subset of patients with chronic urticaria a diet low in cannot be con®rmed in prospective studies. In adults pseudoallergens has been proven to be bene®cial in the rate of type I allergic reactions is below 1%, several studies, with response rates observed in more although in children the percentage appears to be than 55% of patients. Double-blind, placebo-con- higher. Also in chronic urticaria type I allergic reac- trolled challenge tests have shown that arti®cial food tions play only a minor role as an eliciting factor. additives are not only to blame, with the majority of The same holds for the physical urticarias. The role reactions being traced back to naturally occuring of pseudoallergic reactions has not been investigated pseudoallergens in food. Key words: angioderma/hyper- for all types of urticaria, but apparently they are not sensitivity/intolerance/wheal. Journal of Investigative important in physical urticarias; however, in acute Dermatology Symposium Proceedings 6:132±134, 2001 oth allergic and pseudoallergic reactions have fre- evidence for 0 of 50 and 1 of 109 patients, respectively. In quently been discussed as possible eliciting factors in childhood type I allergy appears to be of higher importance, with a various forms of urticaria; however, only a limited rate of 15% reported in the age group of 6 mo to 16 y (Kauppinen number of controlled studies are available. -

Angio-Oedema Associated with Colistin
This open access article is distributed under Creative Commons licence CC-BY-NC 4.0. IN PRACTICE CASE REPORT Angio-oedema associated with colistin A A Abulfathi,1 MBBS; T Greyling,2 MB ChB, FCP (SA), Cert ID (SA) Phys; M Makiwane,1 MB ChB, Dip HIV Man (SA), PG Dip (Pharm Med); M Esser,3 MB ChB, MMed (Paed), Cert Rheum; E Decloedt,1 MB ChB, BSc Hons (Pharm), FCCP (SA), MMed (Clin Pharm) 1 Division of Clinical Pharmacology, Faculty of Medicine and Health Sciences, Stellenbosch University, Tygerberg, Cape Town, South Africa 2 Division of Infectious Diseases, Faculty of Medicine and Health Sciences, Stellenbosch University, Tygerberg, Cape Town, South Africa 3 Immunology Unit, Medical Microbiology, National Health Laboratory Service Tygerberg; and Department of Pathology, Stellenbosch University, Tygerberg, Cape Town, South Africa Corresponding author: A A Abulfathi ([email protected]) A 50-year-old woman known to have type 1 diabetes mellitus presented with a rare case of angio-oedema associated with colistin use. The angio-oedema was temporally associated with the use and discontinuation of colistin with the reasonable exclusion of important differential diagnoses. Pseudoallergy may be a probable underlying mechanism. However, we cannot exclude the possibility of hereditary angio-oedema type 2 or 3, or that her concomitant medications (particularly enalapril) and her renal impairment contributed to the risk and severity of her angio-oedema. S Afr Med J 2016;106(10):990-991. DOI:10.7196/SAMJ.2016.v106i10.10835 We present what is to our knowledge a rare presentation of colistin-induced angio- oedema.[1] Case report 19 March 2015 19 March A 50-year-old woman presented to Tygerberg 2015 9 March 2015 22 March Hospital, Cape Town, South Africa (SA), Actraphane with dysuria, and suprapubic and lower abdominal pain.