Pipefitter Struck by Pressurized Pipe and Killed ______DATE: March 6, 2018 SUMMARY
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Paper: Role of Hydrostatic Testing in Pipeline Integrity Assessment
ROLE OF HYDROSTATIC TESTING IN PIPELINE INTEGRITY ASSESSMENT by John F. Kiefner presented at Northeast Pipeline Integrity Workshop Albany, New York June 12, 2001 KIEFNER AND ASSOCIATES, INC. 893 High Street, Suite L P.O. Box 268 Worthington, Ohio 43085 www.kiefner.com 1 ROLE OF HYDROSTATIC TESTING IN PIPELINE INTEGRITY ASSESSMENT by John F. Kiefner INTRODUCTION Hydrostatic testing is universally known and accepted as a means of demonstrating the fitness of a pressurized component for service(1, 2). After a test, a pipeline or pressure vessel can be expected to safely contain its intended operating pressure. The confidence level that a pipeline or pressure vessel is fit for safe service increases as the ratio of test pressure to operating pressure increases. This highly beneficial aspect of hydrostatic testing applies not only to a new component to be placed in service for the first time. A similar benefit accrues to an in-service component if that component is taken out of service after a period of time and subjected to a hydrostatic test. A “revalidation” test of the latter type assures either that no significant time- dependent deterioration of the component has taken place or that any segment that has been significantly degraded will be revealed and eliminated. There are limitations to the use of hydrostatic testing to revalidate integrity. Some are economic, some are technical, and some are both economic and technical in nature. First, taking a segment of a pipeline out of service means loss of service for the period of the test. Some operators may have this option; others may not. -

Quality Rental Tools and Equipment– Well Serviced, Priced Right
RENTAL CATALOG QUALITY RENTAL TOOLS AND EQUIPMENT– WELL SERVICED, PRICED RIGHT. RENTAL INDEX CORE DRILLS SAFETY AIR COMPRESSORS Core Drills . 1 Confined Space Tripod . 13 Air Compressors - Tow Behind . 24 Accessories . 1 Davit System . 13 Air Compressors - Electric . 24 Bits . 2 Fall Protection Carts . 13 Retractable Lifelines . 13 BREAKERS ELECTRICAL Horizontal Lifelines . 13 Air (30lb, 60lb and 90lb) . 25 Cable Cutters . 3 Gas Monitors . 13 Electric . 25 Cable Crimpers . 3 Monitor Pumps . 13 Air Hose . 25 Cable Pullers . 3 Cable Sheaves . 3 BLOWERS BAKER SCAFFOLD Pull Monitor . 3 Blowers . 14 Baker Scaffold . 25 Cable Feeder . 5 Reel Stands . 5 MATERIAL LIFTS AIR TOOLS Reel Stand Spindles . 5 Material Lifts . 14 Rivet Buster . 26 Rod and Strut Cutters . 5 Roustabouts . 14 Rivet Buster Bits . .26 Conduit Benders . 5-6 A/C Lift and Mover . 14 Scalers . 26 Conduit Cart . 6 Gantry . .15 Chippers . 26 Knock Out Sets . 6 Bits for Air Chippers . 26 Cable Stripper . 6 HYDRAULIC CYLINDERS Impacts . 26 Hydraulic Cylinders/Bags . 15-16 Air Hose . 26 RADIOS Hydraulic Pumps and Hoses . 16 Saws . 28 Radios . 6 TORQUE TOOLS COMPACTION PIPING TOOLS Hand Torque Wrenches . 16 Plate Compactor . .28 Threaders . 7 Cordless Torque Wrenches . 18 Jumping Jack Tampers . 28 Threader Accessories . 7 Hydraulic Torque Wrenches . 18 Roll Groovers . 7 Punches . 18 GENERATORS AND PUMPS Groover Accessories . 9 Generators . 28 See Snake Camera . 9 CHAIN HOISTS Gas Pumps . 29 Locators . 9 Hand Chainfall Hoist . 18-19 Electric Pumps . 29 Pipe Freeze Kits . 9 Hand Lever Hoist (Come-A-Long) . 19 Pipe Thawers . 9 Electric Chainfalls . 20-21 WELDING T-Drills . 9 Air Hoist . -
Formulating Guidance on Hydrotesting Deepwater Oil and Gas Pipelines Final Report
Formulating Guidance on Hydrotesting Deepwater Oil and Gas Pipelines Final Report Prepared for: Bureau of Safety and Environmental Enforcement (BSEE) US Department of the Interior This report has been reviewed by the Bureau of Safety and Environ-mental Enforcement (BSEE) and approved for publication. Approval does not signify that the contents necessarily reflect the views and policies of the Bureau nor does mention of the trade names or commercial products constitute endorsement or recommendation for use. Prepared by: Stress Engineering Services, Inc. Houston, Texas SES Project Number: 1451110 Date Issued: 31 January 2013 Formulating Guidance on Hydrotesting Deepwater Oil and Gas Pipelines Final Report PN 1451110 Coauthored by: Oil & Gas Industry Core Team: Frans Kopp (Shell) Gary Harrison (BP) Ross Frazer (ATP) Wanda Parker (for Anadarko) Mike Williams (FMC) Industry Workshop Participant Responses from: Hess, Marathon, Petrobras, Shell, Williams, Anadarko, Apache, BP, Eni, ExxonMobil, FMC, Chevron, and BSEE Project Manager and Workshop Facilitator: Ray R. Ayers, PhD, PE Key Contributing Staff from Stress Engineering Services: David Garrett, PhD Kenneth Young, PE Lane Alexander, PE Rhett Dotson, PE Stress Engineering Services, Inc. 13800 Westfair East Drive Houston, TX 77041 Texas Registered Engineering Firm F-195 31 January 2013 Study concept, oversight, and funding were provided by the U.S. Department of the Interior, Bureau of Safety and Environmental Enforcement, Washington, DC under Purchase Order Number E12PX00069. Formulating -

308 Safety Equipment Inspections
Document Number: HSE - 308 Current Rev: 11/15/2019 Revised By: S. Lansing Review Cycle: 3 years Manager Approval: MOC No.19-8 Revision No. 0 Revisions noted in italics Page 1 of 23 Health, Safety and Environmental Procedure 308 – Safety Equipment Inspections 1.0 PURPOSE To identify safety equipment and define the process and frequency for these inspections. To also identify and provide specific inspections and preventative maintenance instructions for said safety equipment. 2.0 SCOPE This safety equipment management & inspection system applies to all Westlake’s; safety showers, overhead cranes, SCBA;s, five minute escape packs, SKA-PAK, level “A” suits, bunker gear, emergency rescue gear, ladders, AED’s, first aid kits and fall protection. This safety equipment inspection procedure applies to all Westlake’s employees, visitors, vendors and contract employees. 3.0 DEFINITIONS 3.1 Competent Person – Designated person who is authorized to perform inspections. Competent Persons are trained in equipment inspection and operation. This person is knowledgeable in the requirements of safety equipment inspection and frequency for their area of responsibility. 3.2 Inspection List – List that establishes the minimum requirements for what is inspected and with what frequency and general responsibility for who performs the inspections (see Appendixes). Each unit/area may add to this list to incorporate inspections specific to their particular areas and equipment. 3.3 Department, Area or Unit Supervision – Supervision of the department, area, or unit -

Fire Products Services &
part of www.wisesafetyenv.com Fire Products Services & Boston • Denver • Houston • Jacksonville • Kansas City • Little Rock • Louisville • St. Louis • Salt Lake City Updated 1/2018 Testing & Repair Instrument Service • General Repair • Sensor Replacement • Calibration • Noise Instrument Calibration Testing Services • Respirator Inspection & Cleaning • Respirator Fit Testing • Level A Suit Pressure Testing (required annually or after each use) • SCBA Function Test and Repair Respiratory Mobile Service On-Site Respirator Fit Testing Companies with large inventory of SCBA’s and instruments are often reluctant to send equipment away for service. They fear having an emergency without enough equipment to respond. By bringing our truck or trailer to your location, your equipment is available should a need arise. Call for availability. (No charge for mileage within 30 miles.) Respiratory Cleaning Suit Pressure Testing Half Face (any Manufacturer) . $ 10.00 EA Full Face (any Manufacturer) . 15.00 EA Other Services PAPR-Full Face, Helmet or Visor. 25.00 EA Respirators are cleaned, disinfected, and deodorized with an OSHA, Hydrostatic Test–SCBA Cylinder . $ 30.00 EA ANSI and CSA approved formula and then packaged in individual Hydrostatic Test–Cascade Cylinder. 75.00 EA sterile bags. Price includes inspection for broken or damaged parts SCBA Functional Test . 40.00 EA prior to cleaning. Re place ment parts and labor are extra. Level A Suit Testing. 60.00 EA Cylinder Filling Air Quality Testing . 120.00 EA Any necessary parts or repairs extra 2216 PSI SCBA Cylinder . $ 10.00 EA 3000 PSI SCBA Cylinder . 10.00 EA Quantitative Fit Testing 4500 PSI SCBA Cylinder . 10.00 EA On-Site Quantitative Fit Test . -
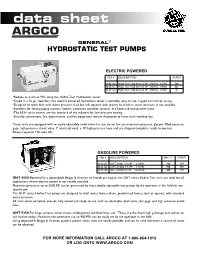
Hydrostatic Test Pumps
data sheet GENERAL® HYDROSTATIC TEST PUMPS ELECTRIC POWERED ITEM # DESCRIPTION WEIGHT 30-99-160 Hydro Test Pump 6334 1/2 HP - 250 PSI - 3 GPM 60# 30-99-161 Hydro Test Pump 6334 3/4 HP - 350 PSI - 3 GPM 64# 30-99-162 Hydro Test Pump 6334 3/4 HP - 500 PSI - 2 GPM 65 •Reduce as much as 90% using the Hydro-Test Hydrostatic tester. •Cased in a 16 ga. steel box, this electric powered hydrostatic tester is portable, easy to use, rugged and money saving. •Designed to work best with water pressure feed but will operate with gravity feed where water pressure is not available. •Excellent for testing piping systems, boilers, automatic sprinkler systems, fire hose and extinguisher tanks. •The 6334 series testers are the standard of the industry for low pressure testing. •Used by contractors, fire departments, and fire equipment dealers thousands of times each working day. These units are equipped with an easily adjustable relief valve that can be set for any maximum pressure, glycerin filled pressure gage, high pressure check valve, 7' electrical cord, a 10' high pressure hose and are shipped complete, ready to operate. Power required 120 volts AC. GASOLINE POWERED ITEM # DESCRIPTION MAX PSI WEIGHT 30-99-163 GHT-3500 3.5 HP - 3 GPM 500 85# 30-99-164 GHT-31000 3.5 HP - 2 GPM 500 85# 30-99-165 GHT-3550 5.5 HP - 10 GPM 400 87# GHT-5550 Powered by a dependable Briggs & Stratton or Honda gas engine, the GHT series Hydro-Test units are ideal for all applications where electric power is not readily available. -
Essentials of Fire Fighting, 6Th Edition
ESSENTIALS OF FIRE FIGHTING INTERNATIONAL FIRE SERVICE TRAINING ASSOCIATION Firefighter Personal Protective Equipment Chapter Contents Case History ......................................259 Donning from a Side or Rear Personal Protective Equipment ...............259 External Mount .......................................... 300 Donning from a Backup Mount...................... 300 Structural Fire Fighting Protective Clothing .. 261 Donning the Facepiece .................................. 301 Wildland Personal Protective Clothing .......... 270 Doffing Protective Breathing Apparatus ....... 302 Roadway Operations Clothing ....................... 273 Emergency Medical Protective Clothing ........274 Inspection and Maintenance of Protective Special Protective Clothing ............................274 Breathing Apparatus ......................303 Station/Work Uniforms ................................. 276 Protective Breathing Apparatus Inspections and Care ..................................................... 303 Care of Personal Protective Clothing ............ 277 Annual Inspection and Maintenance ............. 306 Safety Considerations for Personal Protective Equipment ............................... 280 SCBA Air Cylinder Hydrostatic Testing .......... 306 Respiratory Protection ..........................281 Refilling SCBA Cylinders ............................... 307 Respiratory Hazards ...................................... 281 Replacing SCBA Cylinders ..............................311 Types of Respiratory Using Respiratory Protection Equipment -

Chief Or Training Officer
Chief or Training Officer: In this packet you will find eight (8) forms. The first four (4) forms need to be completed and returned to NIPSTA. The last four (4) forms contain information for you and your candidate. 1. Fire Department Attestation Form 2. Participant Acknowledgment and Release Of Claims Form 3. Candidate information Form 4. Emergency Information Form 5. OSFM Roster Notice 6. Candidate Equipment and Apparel Checklist 7. Required Textbook Notice 8. Physical Fitness Preparation and Expectation All departments must complete the first four (4) forms and return them to NIPSTA no later than one (1) week prior to the start of the program. These forms should be submitted to District Chief and Program Coordinator Orlando Diaz at [email protected]. Please be advised that we maintain an “open campus” philosophy, which means that you and any member of your staff are invited to visit our training grounds at any time to see our operations first-hand. You will also receive weekly progress reports designed to help you track the progress of your personnel, and monitor day-to-day activities. Additionally, you be invited to a Chiefs Luncheon with your Candidate, which will be scheduled mid-way through the nine-week academy program. We thank you for the opportunity and privilege to train your personnel. Please do not hesitate to contact us if you have any Questions, or need more information. Sincerely, Ken Koerber Fire & Technical Rescue Program Director Northeastern Illinois Public Safety Training Academy Cell: 847-567-6976 Email: [email protected] NIPSTA FIRE ACADEMY 2300 Patriot Boulevard Glenview Illinois ★ Phone: (847) 998-8090 ★ Fax: (847) 998-8091 Fire Department Attestation Form Candidate Name: Candidates Fire Department: Fire Academy Session Dates: The undersigned individual attests that the above named participant is enrolled in the NIPSTA Fire Academy on the dates listed above, and: . -

LAG670000.Pdf
Part I Page 2 of 14 LAG670000 AI No. 97422 PART I SECTION A: APPLICABILITY Coverage under this general permit is available for discharges of hydrostatic test and vessel testing wastewater from: 1) new pipelines, flowlines, piping, vessels, or tanks; and 2) pipelines, flowlines, piping, vessels, or tanks which have been used for the transport, transfer, or storage of natural gas, crude oil, liquid or gaseous petroleum hydrocarbons, or other substances which would adequately be regulated by the effluent limitations in this permit, and which discharge wastewater as a result of these hydrostatic tests. For the purpose of this permit, “petroleum” shall mean crude oil, gasoline, diesel fuel, aviation fuel, fuel oils, petroleum lubricants, petroleum solvents, petroleum derived asphalts, and gasoline additives stored and used in conjunction with gasoline storage; and 3) vessel testing wastewater from the above sources provided the vessel testing wastewater is generated from the conduits or vessels that will be hydrostatically tested. This general permit may provide either site-specific or statewide authorization to discharge. Site owners or operators who conduct hydrostatic tests at more than one location in the state may obtain statewide coverage under this permit for discharges related to those testing activities. Statewide authorization numbers shall be designated LAG679XXX while the site-specific authorization numbers are LAG67YXXX where X equals a numeral from 0 to 9 and Y equals a numeral from 0 to 8. All persons operating a source or conducting an activity that results in a discharge as described above and who meet all eligibility conditions may be covered under this general permit and will become permittees authorized to discharge upon the receipt of a hand-delivered, correctly completed Notice of Intent (NOI) by the Office of Environmental Services, Water Permits Division, 48 hours after the postmark date on the envelope that contains the correctly completed NOI, or 48 hours after receipt of an electronic NOI. -

Nondestructive Examination – Overview
Volume 9 Number 1 Nondestructive Examination – Overview December 2009 Introduction: Nondestructive examination (NDE) is a general term that includes all testing, inspection and examination activities used to find, size or determine something about an object or flaws therein, and allow the investigator to determine whether the object and/or flaws are acceptable. Various Flowserve pumps, forms of nondestructive examination are used in the pump industry. This is a subject that has mechanical seals, not previously been covered in a Materials Newsletter article. Given the widespread use of NDE in the manufacture of our products, it was thought that an overview of some of the more commonly quarter-turn valves, used techniques and their primary applications would be beneficial to many of our associates. actuators and controls Discussion: Visual Examination are the benchmarks Visual examination is a minimum requirement for most wrought and cast materials used in pumps. ASTM specifications for ferrous castings require compliance with one of two visual of performance examination standards. A802 “Standard Practice for Visual Examination of Steel Castings – Surface Acceptance Standards” is a newer standard, providing several different in the global acceptance criteria for a wide range of surface defects that can be encountered in castings. industrial equipment It is the responsibility of the purchaser to define the level of quality deemed necessary for the application. In the past, MSS-SP-55 was routinely used for both steels and cast irons to define marketplace. Key to minimum acceptable surface quality. This standard provided only a single level of minimum acceptable quality for various casting defects. Both standards rely on visual comparison with this reputation is the photos showing surface flaws or defects of various severity levels. -
Non Destructive Testing and Evaluation Methods
STP-PT-021 Designator: Meta Bold 24/26 Revision Note: Meta Black 14/16 NON DESTRUCTIVE TESTING AND EVALUATION METHODS FOR COMPOSITE HYDROGEN TANKS Date of Issuance: November 1, 2008 This report was prepared as an account of work sponsored by NCMS and the ASME Standards Technology, LLC (ASME ST-LLC). Neither ASME, ASME ST-LLC, nor others involved in the preparation or review of this report, nor any of their respective employees, members, or persons acting on their behalf, makes any warranty, express or implied, or assumes any legal liability or responsibility for the accuracy, completeness, or usefulness of any information, apparatus, product, or process disclosed, or represents that its use would not infringe upon privately owned rights. Reference in this report to any specific commercial product, process or service by trade name, trademark, manufacturer, or otherwise does not necessarily constitute or imply its endorsement, recommendation or favoring by ASME ST-LLC or others involved in the preparation or review of this report, or any agency thereof. The views and opinions of the authors, contributors and reviewers of the report expressed in this report do not necessarily reflect those of ASME ST-LLC or others involved in the preparation or review of this report, or any agency thereof. ASME ST-LLC does not take any position with respect to the validity of any patent rights asserted in connection with any items mentioned in this document, and does not undertake to insure anyone utilizing a publication against liability for infringement of any applicable Letters Patent, nor assumes any such liability. -

Requirements for Static Pressure Testing Field Piping Systems
Requirements for Static Pressure Testing Field Piping Systems I. SCOPE ............................................................................................................................ 1 II. SPECIFIC REQUIREMENTS ....................................................................................... 1 A. Preparation for test ................................................................................................................ 1 1. Calculations ...................................................................................................................... 1 2. Isolation ............................................................................................................................ 1 3. Selection of test medium ................................................................................................... 1 a) Hydrostatic test ............................................................................................................. 1 b) Pneumatic test ............................................................................................................... 2 c) Test .............................................................................................................................. 2 III. BACKGROUND AND DISCUSSION ............................................................................ 3 A. Philosophy ........................................................................................................................... 3 B. Background .........................................................................................................................