Pharmacogenetic Information in Swiss Drug Labels €“ a Systematic Analysis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Genomic Association of Single Nucleotide Polymorphisms with Blood Pressure Response to Hydrochlorothiazide Among South African Adults with Hypertension
Journal of Personalized Medicine Article Genomic Association of Single Nucleotide Polymorphisms with Blood Pressure Response to Hydrochlorothiazide among South African Adults with Hypertension Charity Masilela 1,* , Brendon Pearce 1 , Joven Jebio Ongole 2 , Oladele Vincent Adeniyi 3 and Mongi Benjeddou 1 1 Department of Biotechnology, University of the Western Cape, Bellville 7530, South Africa; brendon.biff@gmail.com (B.P.); [email protected] (M.B.) 2 Center for Teaching and Learning, Department of Family Medicine, Piet Retief Hospital, Mkhondo 2380, South Africa; [email protected] 3 Department of Family Medicine, Walter Sisulu University, East London 5200, South Africa; [email protected] * Correspondence: [email protected] Received: 23 October 2020; Accepted: 23 November 2020; Published: 9 December 2020 Abstract: This study described single nucleotide polymorphisms (SNPs) in hydrochlorothiazide- associated genes and further assessed their correlation with blood pressure control among South African adults living with hypertension. A total of 291 participants belonging to the Nguni tribes of South Africa on treatment for hypertension were recruited. Nineteen SNPs in hydrochlorothiazide pharmacogenes were selected and genotyped using MassArray. Uncontrolled hypertension was defined as blood pressure 140/90 mmHg. The association between genotypes, alleles and blood ≥ pressure response to treatment was determined by conducting multivariate logistic regression model analysis. The majority of the study participants were female (73.19%), -

An Update on HLA Alleles Associated with Adverse Drug Reactions
Drug Metabol Pers Ther 2017; 32(2): 73–87 Review Ingrid Fricke-Galindo, Adrián LLerena and Marisol López-López* An update on HLA alleles associated with adverse drug reactions DOI 10.1515/dmpt-2016-0025 Due to the improvement of drug therapy and the economic Received July 27, 2016; accepted February 7, 2017; previously published benefit that HLA screening represents, investigations on online March 18, 2017 HLA alleles associated with ADR should continue. Abstract: Adverse drug reactions (ADRs) are considered as Keywords: abacavir; allopurinol; adverse drug reac- an important cause of morbidity and mortality. The hyper- tions; carbamazepine; human leukocyte antigen (HLA); sensitivity reactions are immune-mediated ADRs, which hypersensitivity syndrome; pharmacogenetics; Stevens- are dose-independent, unpredictable and have been asso- Johnson syndrome. ciated with several HLA alleles. The present review aimed to describe HLA alleles that have been associated with different ADRs in populations worldwide, the recommen- dations of regulatory agencies and pharmacoeconomic Introduction information and databases for the study of HLA alleles in Immunologic-mediated adverse drug reactions (ADRs) are pharmacogenetics. A systematic search was performed in included in type B ADRs which are not related to the dose June 2016 of articles relevant to this issue in indexed jour- and that are uncommon and unpredictable in that they are nals and in scientific databases (PubMed and PharmGKB). not related with the pharmacodynamics of the drug and The information of 95 association studies found was sum- present high mortality [1]. There is evidence that suscep- marized. Several HLA alleles and haplotypes have been tibility to at least some Type B ADR is found under strong associated with ADRs induced mainly by carbamazepine, genetic influence [2], and identifying genetic risk factors allopurinol, abacavir and nevirapine, among other drugs. -

Precision Medicine and Adverse Drug Reactions Related to Cardiovascular Drugs †
diseases Review Precision Medicine and Adverse Drug Reactions Related to Cardiovascular Drugs † James D. Noyes 1 , Ify R. Mordi 1 , Alexander S. Doney 2, Rahman Jamal 3 and Chim C. Lang 1,* 1 Division of Molecular and Clinical Medicine, School of Medicine, University of Dundee, Dundee DD1 9SY, UK; [email protected] (J.D.N.); [email protected] (I.R.M.) 2 Division of Population Health and Genomics, School of Medicine, University of Dundee, Dundee DD1 9SY, UK; [email protected] 3 UKM Medical Molecular Biology Institute, Universiti Kebangsaan Malaysia Medical Centre, Kuala Lumpur 56000, Malaysia; [email protected] * Correspondence: [email protected]; Tel.: +44-1382-383283 † Precision medicine in cardiology. Abstract: Cardiovascular disease remains the leading global cause of death. Early intervention, with lifestyle advice alongside appropriate medical therapies, is fundamental to reduce patient mortality among high-risk individuals. For those who live with the daily challenges of cardiovascular disease, pharmacological management aims to relieve symptoms and prevent disease progression. Despite best efforts, prescription drugs are not without their adverse effects, which can cause significant patient morbidity and consequential economic burden for healthcare systems. Patients with cardiovascular diseases are often among the most vulnerable to adverse drug reactions due to multiple co-morbidities and advanced age. Examining a patient’s genome to assess for variants that may alter drug efficacy and susceptibility to adverse reactions underpins pharmacogenomics. This strategy is increasingly being implemented in clinical cardiology to tailor patient therapies. The Citation: Noyes, J.D.; Mordi, I.R.; Doney, A.S.; Jamal, R.; Lang, C.C. -

Pharmacogenomics, How to Deal with Different Types of Variants in Next Generation Sequencing Data in the Personalized Medicine Area
Journal of Clinical Medicine Review Pharmacogenomics, How to Deal with Different Types of Variants in Next Generation Sequencing Data in the Personalized Medicine Area Alireza Tafazoli 1,2 , Natalia Wawrusiewicz-Kurylonek 3, Renata Posmyk 3 and Wojciech Miltyk 1,* 1 Department of Analysis and Bioanalysis of Medicines, Faculty of Pharmacy with the Division of Laboratory Medicine, Medical University of Białystok, 15-089 Białystok, Poland; [email protected] 2 Clinical Research Centre, Medical University of Białystok, 15-276 Bialystok, Poland 3 Department of Clinical Genetics, Medical University of Białystok, 15-089 Białystok, Poland; [email protected] (N.W.-K.); [email protected] (R.P.) * Correspondence: [email protected]; Tel.: +48-857485845 Abstract: Pharmacogenomics (PGx) is the knowledge of diverse drug responses and effects in people, based on their genomic profiles. Such information is considered as one of the main directions to reach personalized medicine in future clinical practices. Since the start of applying next generation sequencing (NGS) methods in drug related clinical investigations, many common medicines found their genetic data for the related metabolizing/shipping proteins in the human body. Yet, the employing of technology is accompanied by big obtained data, which most of them have no clear guidelines for consideration in routine treatment decisions for patients. This review article talks about different types of NGS derived PGx variants in clinical studies and try to display the current and newly developed approaches to deal with pharmacogenetic data with/without clear guidelines for considering in clinical settings. Citation: Tafazoli, A.; Keywords: pharmacogenomics; NGS variants; personalized medicine Wawrusiewicz-Kurylonek, N.; Posmyk, R.; Miltyk, W. -

The Genome-Wide Landscape of Copy Number Variations in the MUSGEN Study Provides Evidence for a Founder Effect in the Isolated Finnish Population
European Journal of Human Genetics (2013) 21, 1411–1416 & 2013 Macmillan Publishers Limited All rights reserved 1018-4813/13 www.nature.com/ejhg ARTICLE The genome-wide landscape of copy number variations in the MUSGEN study provides evidence for a founder effect in the isolated Finnish population Chakravarthi Kanduri1, Liisa Ukkola-Vuoti1, Jaana Oikkonen1, Gemma Buck2, Christine Blancher2, Pirre Raijas3, Kai Karma4, Harri La¨hdesma¨ki5 and Irma Ja¨rvela¨*,1 Here we characterized the genome-wide architecture of copy number variations (CNVs) in 286 healthy, unrelated Finnish individuals belonging to the MUSGEN study, where molecular background underlying musical aptitude and related traits are studied. By using Illumina HumanOmniExpress-12v.1.0 beadchip, we identified 5493 CNVs that were spread across 467 different cytogenetic regions, spanning a total size of 287.83 Mb (B9.6% of the human genome). Merging the overlapping CNVs across samples resulted in 999 discrete copy number variable regions (CNVRs), of which B6.9% were putatively novel. The average number of CNVs per person was 20, whereas the average size of CNV per locus was 52.39 kb. Large CNVs (41 Mb) were present in 4% of the samples. The proportion of homozygous deletions in this data set (B12.4%) seemed to be higher when compared with three other populations. Interestingly, several CNVRs were significantly enriched in this sample set, whereas several others were totally depleted. For example, a CNVR at chr2p22.1 intersecting GALM was more common in this population (P ¼ 3.3706 Â 10 À44) than in African and other European populations. The enriched CNVRs, however, showed no significant association with music-related phenotypes. -
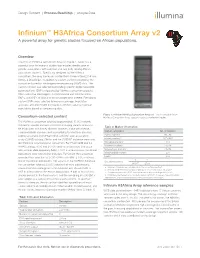
Infinium™ H3africa Consortium Array V2 a Powerful Array for Genetic Studies Focused on African Populations
Design Content | Process BeadChip | Analyze Data Infinium™ H3Africa Consortium Array v2 A powerful array for genetic studies focused on African populations. Overview The Infinium H3Africa Consortium Array v2 (Figure 1, Table 1) is a powerful array for research studies that enables identification of genetic associations with common and rare traits among African populations (Table 2). Specifically designed by the H3Africa consortium, the array harnesses content from Illumina Omni2.5-8 and Omni5-4 BeadChips, in addition to custom content selected by the consortium based on whole-genome sequencing (WGS) data. The custom content was selected by including specific single nucleotide polymorphisms (SNPs) requested by H3Africa consortium projects, SNPs within the MHC region, X-chromosome and mitochondrion SNPs, and SNPs of clinical or pharmacogenomic interest. Remaining custom SNPs were selected to improve coverage, imputation accuracy, and enrichment in novel but common variants in African populations based on sequencing data. Figure 1: Infinium H3Africa Consortium Array v2—The 8-sample Infinium Consortium-selected content H3Africa Consortium Array supports rapid cost-effective studies. The H3Africa consortium selected approximately 10,000 variants relevant to specific diseases of interest including variants known to Table 2: Marker information be associated with kidney disease, diabetes, sickle cell disease, a cardiometabolic diseases and susceptibility to infectious diseases. Marker categories No. of markers b Additional variants from PharmGKB, genome-wide association Exonic markers 88,785 b study (GWAS) catalog, ClinVar and the COSMIC database were also Intronic markers 1,074,881 c identified and selected by the consortium. For PharmGKB and the Nonsense markers 313 c GWAS catalog, 4000 and 24,000 variants, respectively, that occur Missense markers 23,548 c with a minor allele frequency (MAF) ≥ 0.01 in at least one of the African Synonymous markers 21,654 c populations were selected for inclusion. -

Genome-Wide Association Studies of Drug Response and Toxicity: an Opportunity for Genome Medicine
HHS Public Access Author manuscript Author ManuscriptAuthor Manuscript Author Nat Rev Manuscript Author Drug Discov. Author Manuscript Author manuscript; available in PMC 2017 May 24. Published in final edited form as: Nat Rev Drug Discov. 2017 January ; 16(1): 1. doi:10.1038/nrd.2016.234. Genome-wide Association Studies of Drug Response and Toxicity: An Opportunity for Genome Medicine Kathleen M. Giacomini1,2,*, Sook Wah Yee1, Taisei Mushiroda3, Richard M. Weinshilboum4, Mark J. Ratain5, and Michiaki Kubo3,* 1Department of Bioengineering and Therapeutic Sciences, University of California San Francisco 2Institute of Human Genetics, University of California San Francisco 3RIKEN Center for Integrative Medical Science, Yokohama 230-0045, Japan 4Division of Clinical Pharmacology, Mayo Clinic, Rochester, Minnesota 55905 5Center for Personalized Therapeutics, University of Chicago, Chicago, Illinois, USA 6Department of Medicine, University of Chicago, Chicago, Illinois, USA Genome-wide association studies (GWAS), provide an unbiased approach for the discovery of potential mechanisms and pathways that underlie human characteristics, diseases and drug response. As common diseases are frequently associated with genetic variants that exert small effect sizes, GWAS have increasingly focused on large cohorts of patients. For example, a recent mega-GWAS of schizophrenia included more than 37,000 individuals with schizophrenia and 113,000 controls, which enabled the identification of 108 genetic regions linked to schizophrenia, of which 83 were novel, as discussed in a recent news article (Massive schizophrenia genomic study offers new drug directions. Nat. Rev. Drug Discov., 13, 641–642 (2014))1. This study was made possible through the Psychiatric Genomics Consortium, a large group of more than 500 scientists coming from 80 different institutions. -

Reference ID
HIGHLIGHTS OF PRESCRIBING INFORMATION Interstitial Lung Disease (ILD)/Pneumonitis: Occurred in 0.4% of patients. These highlights do not include all the information needed to use Immediately withhold ALECENSA in patients diagnosed with ALECENSA safely and effectively. See full prescribing information for ILD/pneumonitis and permanently discontinue if no other potential causes ALECENSA. of ILD/pneumonitis have been identified. (2.2, 5.2) Bradycardia: Monitor heart rate and blood pressure regularly. If ALECENSA® (alectinib) capsules, for oral use symptomatic, withhold ALECENSA then reduce dose, or permanently Initial U.S. Approval: 2015 discontinue. (2.2, 5.3) Severe Myalgia and Creatine Phosphokinase (CPK) Elevation: Occurred in --------------------------- INDICATIONS AND USAGE ---------------------------- 1.2% and 4.6% of patients, respectively. Assess CPK every 2 weeks during ALECENSA is a kinase inhibitor indicated for the treatment of patients with the first month of treatment and in patients reporting unexplained muscle anaplastic lymphoma kinase (ALK)-positive, metastatic non-small cell lung pain, tenderness, or weakness. In case of severe CPK elevations, withhold, cancer (NSCLC) who have progressed on or are intolerant to crizotinib. This then resume or reduce dose. (2.2, 5.4) indication is approved under accelerated approval based on tumor response Embryo-Fetal Toxicity: ALECENSA can cause fetal harm. Advise females rate and duration of response. Continued approval for this indication may be of reproductive potential of the potential risk to a fetus and to use effective contingent upon verification and description of clinical benefit in contraception. (5.5, 8.1 8.3) confirmatory trials. (1) ------------------------------ ADVERSE REACTIONS ------------------------------ ----------------------- DOSAGE AND ADMINISTRATION ----------------------- The most common adverse reactions (incidence fatigue, 600 mg orally twice daily. -

SLCO1B1 Pharmacogenetic Competency
SLCO1B1 Pharmacogenetic Competency Updated on 6/2015 Pre-test Question # 1 Which of the following is not currently a recognized SLCO1B1 phenotype? a) Low function b) Normal function c) Intermediate function d) Ultra-rapid function Pre-test Question # 2 What is the predicted SLCO1B1 phenotype for a patient with a genotype of *1/*15? a) Ultra-rapid metabolizer b) Extensive metabolizer c) Intermediate metabolizer d) Poor metabolizer Pre-test Question # 3 A patient with a low function SLCO1B1 phenotype is at ____________ risk for developing myopathy if prescribed normal doses of simvastatin. a) Low b) Intermediate c) High d) Normal Pre-test Question # 4 Which of the following simvastatin dosing adjustments is correct for a patient with the SLCO1B1 *5/*15 genotype? a) Consider an alternative statin agent b) Initiate simvastatin therapy at 20 mg/day c) Initiate simvastatin therapy at 40 mg/day d) Initiate simvastatin therapy at 80 mg/day Objectives • Upon completion of this competency, participants will be able to: – Recognize the different SLCO1B1 allele variants – Recognize the different SLCO1B1 phenotypes – Assign the correct phenotype based upon the allele variants – Make therapeutic recommendations for simvastatin dosing based on a patient's predicted SLCO1B1 phenotype SLCO1B1 Pharmacogenetics SLCO1B1 • SLCO1B1 stands for solute carrier organic anion transporter family member 1B1 • SLCO1B1 is a gene located on chromosome 12, that encodes for an organic anion transporter (SLCO1B1) that mediates the hepatic uptake of many endogenous compounds, such as bile acids, and several medicines including simvastatin. • For these medications, dose adjustments or alternative therapies may be needed if there is impaired transporter function Ramsey LB, et al. -

CPIC Guideline Update on Pharmgkb
CPIC Guideline Update on PharmGKB For: Clinical Pharmacogenetics Implementation Consortium Guidelines for Cytochrome P450 2D6 Genotype and Codeine Therapy: 2014 Update Date: August 2015 URL: (https://www.pharmgkb.org/guideline/PA166104996) Description: Supplemental table S3 (Association between allelic variants and CYP2D6 enzyme activity) was updated with Supplemental table S2 from the Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6 and CYP2C19 Genotypes and Dosing of Selective Serotonin Reuptake Inhibitors (2015 Supplement) PMID: 25974703. The table is an updated version including additions to functional status and additional alleles. Please see the updated guideline supplement at: (https://www.pharmgkb.org/guideline/PA166104996) Supplemental Material Clinical Pharmacogenetics Implementation Consortium (CPIC) guidelines for cytochrome P450 2D6 (CYP2D6) genotype and codeine therapy: 2014 Update Kristine R. Crews1, Andrea Gaedigk2,3, Henry M. Dunnenberger1, J. Steve Leeder2,3, Teri E. Klein4, Kelly E. Caudle1, Cyrine Haidar1, Danny D. Shen5, John T. Callaghan6,7, Senthilkumar Sadhasivam8,9, Cynthia A. Prows10,11, Evan D. Kharasch12, Todd C. Skaar5 1Department of Pharmaceutical Sciences, St. Jude Children’s Research Hospital, Memphis, TN 2 Division of Clinical Pharmacology & Therapeutic Innovation, Children’s Mercy Hospital & Clinics, Kansas City, MO 3Department of Pediatrics, University of Missouri-Kansas City, Kansas City, Missouri 4Department of Genetics, Stanford University, Stanford, CA 5Departments -

Abacavir Pathway Julia M
276 PharmGKB summary PharmGKB summary: abacavir pathway Julia M. Barbarinoa, Deanna L. Kroetzc, Russ B. Altmana,b and Teri E. Kleina Pharmacogenetics and Genomics 2014, 24:276–282 Correspondence to Teri E. Klein, PhD, Department of Genetics, 318 Campus Drive, Clark Center Room S221A, MC: 5448, Stanford, CA 94305, USA Keywords: abacavir, HIV, HLA-B, HLA-B*57:01, HSP70-HOM, hypersensitivity, Tel: + 1 650 736 0156; fax: + 1 650 725 3863; e-mail: [email protected] pharmacodynamics, pharmacogenetics, pharmacokinetics, PharmGKB Received 4 December 2013 Accepted 5 February 2014 Departments of aGenetics, bBioengineering, Stanford University, Stanford and cDepartment of Bioengineering and Therapeutic Sciences, University of California, San Francisco, California, USA Introduction P450 (CYP) enzymes are predicted [2]. In addition, in- Abacavir is a nucleoside reverse transcriptase inhibitor vitro studies have shown that abacavir is unlikely to (NRTI) used for treatment of HIV infection. HIV inhibit CYP enzymes at clinically relevant concentra- infection is usually treated with antiretroviral therapy tions [14]. As non-NRTIs and protease inhibitors are regimens, which consist of three or more different drugs primarily metabolized by CYP enzymes [15], this may used in combination. Typical antiretrovirals used in these eliminate the potential for drug interactions with regimens include NRTIs, non-NRTIs, protease inhibi- these types of antiretrovirals. No clinically significant tors, and integrase strand inhibitors [1]. Abacavir makes pharmacokinetic -

Linking Pharmacogenomic Information on Drug Safety and Efficacy with Ethnic Minority Populations
pharmaceutics Article Linking Pharmacogenomic Information on Drug Safety and Efficacy with Ethnic Minority Populations Dan Li 1, April Hui Xie 1,2, Zhichao Liu 1, Dongying Li 1, Baitang Ning 1, Shraddha Thakkar 1,3, Weida Tong 1 and Joshua Xu 1,* 1 Division of Bioinformatics and Biostatistics, National Center for Toxicological Research, U.S. Food and Drug Administration, Jefferson, AR 72079, USA; [email protected] (D.L.); [email protected] (A.H.X.); [email protected] (Z.L.); [email protected] (D.L.); [email protected] (B.N.); [email protected] (S.T.); [email protected] (W.T.) 2 School of Pharmacy, Virginia Commonwealth University, Richmond, VA 23298, USA 3 Office of Computational Sciences, Office of Translational Sciences, Center for Drug Evaluation and Research, U.S. Food and Drug Administration, Silver Spring, MD 20993, USA * Correspondence: [email protected] Received: 8 October 2020; Accepted: 23 October 2020; Published: 25 October 2020 Abstract: Numerous prescription drugs’ labeling contains pharmacogenomic (PGx) information to aid health providers and patients in the safe and effective use of drugs. However, clinical studies for such PGx biomarkers and related drug doses are generally not conducted in diverse ethnic populations. Thus, it is urgently important to incorporate PGx information with genetic characteristics of racial and ethnic minority populations and utilize it to promote minority health. In this project a bioinformatics approach was developed to enhance the collection of PGx information related to ethnic minorities to pave the way toward understanding the population-wide utility of PGx information.