Appendix 4: a Guide to Public Health
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Exploration of How a Mobile Health (Mhealth) Intervention May Support
WHITE, A. 2018. Exploration of how a mobile health (mHealth) intervention may support midwives in the management and referral of women with pre-eclampsia in rural and remote areas of highland Scotland. Robert Gordon University [online], MRes thesis. Available from: https://openair.rgu.ac.uk Exploration of how a mobile health (mHealth) intervention may support midwives in the management and referral of women with pre- eclampsia in rural and remote areas of highland Scotland. WHITE, A. 2018 The author of this thesis retains the right to be identified as such on any occasion in which content from this thesis is referenced or re-used. The licence under which this thesis is distributed applies to the text and any original images only – re-use of any third-party content must still be cleared with the original copyright holder. This document was downloaded from https://openair.rgu.ac.uk Exploration of how a mobile health (mHealth) intervention may support midwives in the management and referral of women with pre-eclampsia in rural and remote areas of Highland Scotland A thesis presented for the degree of Master of Research (part-time) in Nursing and Midwifery by Research at the Robert Gordon University by Alan White 1601992 Supervisors: Prof Dr Susan Crowther and Dr Siew Hwa Lee This study was supported by a grant from The Scottish Digital Health and Care Institute (DHI) February 2018 1 Contents Page List of Tables 8 List of Figures 8 Abstract 9 Declaration of authorship 12 Acknowledgements 15 Glossary and definition of terms 17 CHAPTER 1– Introduction -

Qualitative Baseline Evaluation of the GP
Qualitative baseline evaluation of the GP Community Hub Fellowship pilot in NHS Fife and NHS Forth Valley Briefing paper This resource may also be made available on request in the following formats: 0131 314 5300 [email protected] This briefing paper was prepared by NHS Health Scotland based on the findings from the evaluation undertaken by Fiona Harris, Hazel Booth and Sarah Wane at the Nursing, Midwifery and Allied Health Professions Research Unit – University of Stirling. Published by NHS Health Scotland 1 South Gyle Crescent Edinburgh EH12 9EB © NHS Health Scotland 2018 All rights reserved. Material contained in this publication may not be reproduced in whole or part without prior permission of NHS Health Scotland (or other copyright owners). While every effort is made to ensure that the information given here is accurate, no legal responsibility is accepted for any errors, omissions or misleading statements. NHS Health Scotland is a WHO Collaborating Centre for Health Promotion and Public Health Development. Summary In 2016 NHS Fife and NHS Forth Valley began to pilot a new GP Community Hub (GPCH) Fellowship model aimed at bridging the gap between primary and secondary care for frail elderly patients and those with complex needs. NHS Health Scotland commissioned a baseline evaluation to capture the early learning from implementation of the model. The following summarises the key findings from the evaluation. The evaluation was conducted between February and June 2017 when the model of delivery in the two pilot sites was still evolving. The findings may therefore not reflect the ways in which the model was subsequently developed and is currently being delivered in the two areas. -

Nhs Lanarkshire Patient Access Policy
NHS LANARKSHIRE PATIENT ACCESS POLICY 1. BACKGROUND NHS Lanarkshire is required by Scottish Government to deliver a consistent, safe, equitable and patient centred service to Lanarkshire patients within national waiting time standards. The current waiting time standards are: • 12 weeks for new outpatient appointment • 6 weeks for the eight diagnostic tests and investigations • 18 weeks Referral to Treatment for 90% of patients • The legal 12 week Treatment Time Guarantee NHS Lanarkshire is required from 1 October 2012 to comply with the Patient Rights (Scotland) Act 2011 that places a legal responsibility on the NHS Board to ensure that all patients due to receive planned treatment on a day case or inpatient basis receive treatment within 12 weeks of the patient agreeing to the treatment. The Patient Access Policy sets out the approach that NHS Lanarkshire will follow to book outpatient, day case, inpatient and diagnostic appointments, what patients can expect in terms of advance notification and the number and type of offers of appointment they can expect to receive. It describes the locations from which services are routinely delivered by NHS Lanarkshire. The Patient Access Policy also sets out the implications to the patient of cancelled appointments and also non-attendance at clinic and /or treatment. In addition, it describes actions available to patients when they are dissatisfied with the service that they receive. NHS Lanarkshire is committed to improving the patient journey and patient experience through improved process, effective use of new technology and through maximising available capacity. Effective communication with patients is essential to achieving that and NHS Lanarkshire will use all available options including letter, email and text to keep in contact with patients. -
Inverclyde CHCP
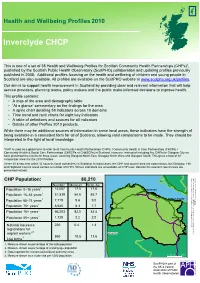
Inverclyde CHCP Inverclyde Health 2010 Health and Wellbeing Profiles published by the Scottish Public Observatory Health presented instead. of CHPs number areas andcontain aCouncil Highland areasnestThese autho38 councils within 32 (local comparator areasfor Profiles.2010 the for presentedhave threeareas,results coverin the Community Health &(CHSCPs Social Care Partnerships used toCommu*CHP is all global term toas refer a interpretedin the lightoflocal knowledge. being availablea in consistent form for allofSco While there be may additional sources of informatio This profile contains: serviceproviders, planning teams, policy makers an aim Our is to support health improvement in Scotlan published in Additional2008. profiles focusingon This is setof a one Healthof38 andWellbeing Pro Scotland available.are also All areavailprofiles CHP CHP Population: 80,210 4. Measure shown as a crude rate per 1,000 populati 1,000 perrate crude a as shown Measure 4. author (local council reported for relevant Data 3. popul age working of percentage as shown Measure 2. populat total the of percentage as shown Measure 1. Population Population 75+ years Population 65–74 years Population 16–64 years Population 0–15 years Population Population 85+ years Population 16+ years Live births workers migrant registrations for National insurance • • • • • • ‘At glance’a commentary theon findings for the a Aof thearea map demographyand table A spinechart detailing indicatorsacross59 10 do A table of definitions sourcesand for allindicat Time andtrend rank eightcharts for key indicator Details Profilesof other products.2010 4 2,3 1 1 1 1 1 1 Number Measure Scot. Av. 860220 10.6 1,72966,203 0.4 6,645 2.2 82.5 7,71951,839 8.3 14,007 9.6 64.6 17.5 ity)area g Glasgow North Glasgow North Westg andEast,Glasgow Glasgo on ion rities) in Scotland. -

The Governance of the NHS in Scotland - Ensuring Delivery of the Best Healthcare for Scotland Published in Scotland by the Scottish Parliamentary Corporate Body
Published 2 July 2018 SP Paper 367 7th report (Session 5) Health and Sport Committee Comataidh Slàinte is Spòrs The Governance of the NHS in Scotland - ensuring delivery of the best healthcare for Scotland Published in Scotland by the Scottish Parliamentary Corporate Body. All documents are available on the Scottish For information on the Scottish Parliament contact Parliament website at: Public Information on: http://www.parliament.scot/abouttheparliament/ Telephone: 0131 348 5000 91279.aspx Textphone: 0800 092 7100 Email: [email protected] © Parliamentary copyright. Scottish Parliament Corporate Body The Scottish Parliament's copyright policy can be found on the website — www.parliament.scot Health and Sport Committee The Governance of the NHS in Scotland - ensuring delivery of the best healthcare for Scotland, 7th report (Session 5) Contents Introduction ____________________________________________________________1 Staff Governance________________________________________________________3 Staff Governance Standard _______________________________________________3 Monitoring views of NHS Scotland staff______________________________________4 Staff Governance - themes raised in evidence ________________________________4 Pressure on staff - what witnesses told us __________________________________5 Consultation and staff relations __________________________________________6 Discrimination, bullying and harassment _________________________________7 Whistleblowing_________________________________________________________8 Confidence to -

GP Registration Form 2020
APPLICATION TO REGISTER PERMANENTLY WITH A GENERAL MEDICAL PRACTICE ALL FIELDS MARKED * ARE MANDATORY AND MUST BE COMPLETED AS FULLY AS POSSIBLE 1. PERSONAL DETAILS ,VWKLV\RXU¿UVWUHJLVWUDWLRQZLWKD Yes No Will you be in the area for more Yes No GP Practice in the UK? than 3 months? ,Iµ1R¶SOHDVHFRPSOHWHDWHPSRUDU\UHVLGHQWIRUP Male * Female * Date of birth * Address * Title * Surname * Forenames * Previous surname * Postcode * Telephone # Email address # Mobile # WKHGDWDVXSSOLHGLQWKHVH¿HOGVZLOOQRWEHLQSXWWRRUXSGDWHGLQWKH&RPPXQLW\+HDOWK,QGH[ &+, EXWZLOOEHKHOGRQWKH*33UDFWLFH¶VV\VWHP The following information can be found on your current medical card : Community Health Index (CHI) number * NHS number * The following information can be found on your ELUWKFHUWL¿FDWH : Town of birth * Country of birth * Registered district of birth Mother’s maiden name 6FRWODQGRQO\ 2. HELP US TO TRACE YOUR PREVIOUS GP HEALTH RECORDS BY PROVIDING THE FOLLOWING INFORMATION Address in UK when you were last registered with a GP * Name and address of previous GP Practice in UK * Postcode * Postcode * If you are from abroad: 'DWH\RX¿UVWFDPHWROLYHLQWKH8. If previously resident in the UK, date of leaving * Your most recent country of residence If you have served in the British Armed Forces: Service Number Enlistment date * Are you a Reservist? Yes No If yes provide your address before enlisting * Leaving date * Postcode * ,VWKLV\RXU¿UVWUHJLVWUDWLRQZLWKD*3VLQFHOHDYLQJWKHDUPHGIRUFHV" Yes No 1 *06*359 3. VOLUNTARY AUTHORISATION FOR ORGAN OR TISSUE DONATION <RXKDYHDFKRLFHDERXWRUJDQRUWLVVXHGRQDWLRQDIWHU\RXUGHDWK7RILQGRXWPRUHDERXWZK\LWLVLPSRUWDQWWKDW\RXWDNHWKHWLPHWRPDNH\RXUGRQDWLRQ GHFLVLRQDQGUHFRUGLWJRWRwww.organdonationscotland.org 4. HOW WE USE INFORMATION The information you have provided will be used by NHS Scotland to carry out its various functions and services including scheduling appointments, ordering tests, hospital referrals and sending correspondence. -
NHS Western Isles Written Submission
HS/S5/18/16/7 Submission for the Scottish Parliament Health and Sport Committee 15 May 2018 Gordon Jamieson Chief Executive, NHS Western Isles Page 1 of 329 HS/S5/18/16/7 NHS WESTERN ISLES LOCAL DELIVERY PLAN 2017/18 Filename LDP Version 2 Owner Dr Maggie Watts Director of Public Health Author Michelle McPhail Business Manager 1 Page 2 of 329 HS/S5/18/16/7 CONTENT Strategic Priority 1 – Health Inequalities and Prevention 1.1 ~ NHS Procurement Policies 1.2 ~ Employment policies supporting people to gain employment 1.3 ~ Supporting staff to support most vulnerable populations 1.4 ~ Using Horticulture as a complementary form of therapy 1.5 ~ Smoke Hebrides 1.6 ~ Health Promoting Health Service 1.7 ~ Healthy Working Lives 1.8 ~ Alcohol 1.9 ~ Obesity / Weight management 1.10 ~ Detect Cancer Early 1.11 ~ Police custody healthcare referral pathways Strategic Priority 2 – Antenatal and Early Years 2.1 ~ Duties consequent to Children and Young People (Scotland) Act 2014 – Staff development 2.2 ~ Health Visiting Strategic Priority 3 – Person Centred Care 3.1 ~ Person centred care (“Must do with Me”) 3.2 ~ Staff and public feedback 3.3 ~ Feedback and complaints – closing the loop Strategic Priority 4 – Safe Care 4.1 ~ Excellence in Care 4.2 ~ Scottish Patient Safety Programme rollout of acute programme into primary care, maternity, neonates and paediatrics and mental health services Strategic Priority 5 – Primary Care 5.1 ~ Strategic Intentions – 5.1.1 ~ Leadership and workforce 5.1.2 ~ Prioritised local actions to increase capacity 5.1.3 ~ Technology -

Public Health Reform Commission
Public Health Reform Commission Leadership for Public Health Research, Innovation and Applied Evidence Stakeholder Engagement August Engagement Event Capturing Emerging Stakeholder Views Appendix 1 1 | P a g e 21/08/2018 – Glasgow Attendees First Name Surname Job Title Organisation Mahmood Adil Medical Director NHS National Services Scotland Gillian Armour Librarian NHS Health Scotland Julie Arnot Researcher ScotPHN Hannah Atkins Knowledge Exchange Fellow University of Stirling Hannah Austin Specialty Registrar in Public Health ScotPHN Marion Bain Co-Director, Executive Delivery Group Scottish Government Rachel Baker Professor of Health Economics and Director Glasgow Caledonian University Tom Barlow Senior Research Manager Scottish Government Chief Scientist Office Corri Black Professor of Public Health University of Aberdeen Alison Bogle Library Services Manager NHS National Services Scotland Bernardette Bonello Research Associate University of Glasgow Craig Brown Environmental Services Manager South Lanarkshire Council NHS National Services Scotland - Information Duncan Buchanan Head of Service Services Division Simon Capewell Professor of Clinical Epidemiology University of Liverpool Andrew Carse Manager - Quality Improvement and Performance Angus Council Eric Chen Researcher NHS Lothian Ann Conacher ScotPHN Network Manager ScotPHN David Conway Professor of Dental Public Health University of Glasgow Phillip Couser Director Public Health and Intelligence NHS National Services Scotland Neil Craig Public Health Intelligence Principal -

New Patient Registration Pack (ADULT)
APPLICATION TO REGISTER PERMANENTLY WITH A GENERAL MEDICAL PRACTICE ALL FIELDS MARKED * ARE MANDATORY AND MUST BE COMPLETED AS FULLY AS POSSIBLE 1. PERSONAL DETAILS ,VWKLV\RXU¿UVWUHJLVWUDWLRQZLWKD Yes No Will you be in the area for more Yes No GP Practice in the UK? than 3 months? ,Iµ1R¶SOHDVHFRPSOHWHDWHPSRUDU\UHVLGHQWIRUP Male * Female * Date of birth * Address * Title * Surname * Forenames * Previous surname * Postcode * Telephone # Email address # Mobile # WKHGDWDVXSSOLHGLQWKHVH¿HOGVZLOOQRWEHLQSXWWRRUXSGDWHGLQWKH&RPPXQLW\+HDOWK,QGH[ &+, EXWZLOOEHKHOGRQWKH*33UDFWLFH¶VV\VWHP The following information can be found on your current medical card : Community Health Index (CHI) number * NHS number * The following information can be found on your ELUWKFHUWL¿FDWH : Town of birth * Country of birth * Registered district of birth Mother’s maiden name 6FRWODQGRQO\ 2. HELP US TO TRACE YOUR PREVIOUS GP HEALTH RECORDS BY PROVIDING THE FOLLOWING INFORMATION Address in UK when you were last registered with a GP * Name and address of previous GP Practice in UK * Postcode * Postcode * If you are from abroad: 'DWH\RX¿UVWFDPHWROLYHLQWKH8. If previously resident in the UK, date of leaving * Your most recent country of residence If you have served in the British Armed Forces: Service Number Enlistment date * Are you a Reservist? Yes No If yes provide your address before enlisting * Leaving date * Postcode * ,VWKLV\RXU¿UVWUHJLVWUDWLRQZLWKD*3VLQFHOHDYLQJWKHDUPHGIRUFHV" Yes No 1 *06*359 3. VOLUNTARY AUTHORISATION FOR ORGAN OR TISSUE DONATION <RXKDYHDFKRLFHDERXWRUJDQRUWLVVXHGRQDWLRQDIWHU\RXUGHDWK7RILQGRXWPRUHDERXWZK\LWLVLPSRUWDQWWKDW\RXWDNHWKHWLPHWRPDNH\RXUGRQDWLRQ GHFLVLRQDQGUHFRUGLWJRWRwww.organdonationscotland.org 4. HOW WE USE INFORMATION The information you have provided will be used by NHS Scotland to carry out its various functions and services including scheduling appointments, ordering tests, hospital referrals and sending correspondence. -

Language Provision in the Scottish Public Sector: Recommendations to Promote Inclusive Practice
Social Inclusion (ISSN: 2183–2803) 2021, Volume 9, Issue 1, Pages 45–55 DOI: 10.17645/si.v9i1.3549 Article Language Provision in the Scottish Public Sector: Recommendations to Promote Inclusive Practice Róisín McKelvey 1,2 1 Faculty of Social Sciences, University of Stirling, Stirling, FK9 4LA, Scotland; E-Mail: [email protected] 2 School of Literatures, Languages and Cultures, University of Edinburgh, Edinburgh, EH8 9YL, Scotland Submitted: 30 July 2020 | Accepted: 28 September 2020 | Published: 14 January 2021 Abstract Public service providers in Scotland have developed language support, largely in the form of interpreting and translation, to meet the linguistic needs of those who cannot access their services in English. Five core public sector services were selected for inclusion in a research project that focused on the aforementioned language provision and related equality issues: the Scottish Courts and Tribunal Service, NHS Lothian, NHS Greater Glasgow and Clyde, the City of Edinburgh Council and Glasgow City Council. The frameworks within which these public service providers operate—namely, the obligations derived from supranational and domestic legal and policy instruments—were analysed, as was the considerable body of standards and strategy documents that has been produced, by both national organisations and local service providers, in order to guide service delivery. Although UK equalities legislation has largely overlooked allochthonous languages and their speakers, this research found that the public service providers in question appear to regard the provision of language support as an obligation related to the Equality Act (UK Government, 2010). Many common practices related to language support were also observed across these services, in addition to shared challenges, both attitudinal and practical. -

Corporate Communications Strategy 2018 – 2021
NHS Forth Valley Communications Strategy 2018-2021 Table of Contents Page 1. Introduction 3 2. Aims and Objectives 4 3. Key Principles 4 4. Roles and Responsibilities 5 5. Policy Context 6 6. Key Audiences 6 7. Overview of Progress 7 8. Communication Priorities 8 9. Communication Tools 11 10. Monitoring and Evaluation 14 2 1. INTRODUCTION NHS services in Scotland have always been subject to change and this is set to continue over the next three years with work to implement NHS Forth Valley’s new Healthcare Strategy, progress health and social care integration, develop new regional delivery plans and implement key national strategies. A rising elderly population, growing numbers of people experiencing dementia and an increase in the number of people living with long-term health conditions such as diabetes, asthma and heart disease will also require new and innovative ways of working with a major shift to deliver care in people’s homes and local communities rather than in hospitals. There will also be an increasing requirement for 7 day working in both hospital and community-based health services. In addition, developments within the media and wider culture such as the increasing expansion of online media and the ever growing use of social media present require a shift in emphasis from traditional communication channels such as print media to online and digital communication channels. These changes will require a joined up approach to communications with greater partnership working at a local, regional and national level, more creative, innovative and cost-effective use of resources, innovative approaches and greater use of technology. -

Accessing Healthcare in Other Countries of the European Economic Area by the S2 (E112) Route
Accessing Healthcare in England If you are registered with a general practitioner in Scotland then you are entitled to free NHS care arranged by NHS Scotland. Generally that care will be provided as close to home as possible and within your own NHS Board area but care may be provided elsewhere in NHS Scotland if that is clinically necessary. NHS England runs a different financial system involving internal charging between “providers” (NHS Trusts) and “commissioners” (NHS Primary Care Trusts) for health care services. Residents of Scotland who are registered with a GP in Scotland will always be entitled to emergency care anywhere in the UK but are not automatically entitled to access elective (planned) NHS care in England as NHS providers will expect to invoice NHS Scotland for providing that service. Before providing elective services to patients registered within NHS Scotland, a provider Trust is therefore required to obtain advance financial consent from the relevant NHS Scotland Board. Where a patient wishes to access routine healthcare in England for social reasons such as studying or working in England or staying with relatives for a period longer than a normal holiday then we would strongly recommend that the patient registers with a local general practitioner in England which will entitle them to access their routine NHS care including community services from NHS England. Where it is necessary for clinical reasons to refer a patient to a specialist service in England because that service is not available in NHS Scotland then this is usually funded through national agreements managed by NHS National Services Division in Edinburgh.