The Biometric Parameters of Aniso
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Annual Report
合 縱 連 橫 China New Town Development Company Limited 中國新城鎮發展有限公司 Hong Kong Stock Code: 1278 推 進 新 型 城 鎮 化 建 設 Singapore Stock Code: D4N.si 穩 中 致 勝 2015 Annual Report CORPORATE PROFILE Overview China New Town Development Company Limited (Stock code: D4N.si or 1278.hk) (the “Company” or “CNTD”) is dual-listed on the main board of The Singapore Exchange Securities Trading Limited (“SGX”) and The Stock Exchange of Hong Kong Limited (“HKEx”) since 14 November 2007 and 22 October 2010 respectively. In March 2014, China Development Bank International Holdings Limited (“CDBIH”), a wholly-owned subsidiary of China Development Bank Capital Corporation Limited (“CDBC” or “CDB Capital”) completed its subscription of CNTD’s 54.3% shares. China Development Bank Corporation (“CDB”) is one of the biggest policy Banks in China and has been continuously supporting the urbanization construction in China since its establishment. CDB Capital, as a wholly owned subsidiary of CDB, has a national network layout in the business segment of new town development business. To this point, the Company has officially become the one and only listed platform of CDB and CDB Capital in the business segment of new urbanization. In the future, we will leverage the advantage of controlling shareholder’s resources and experience, and integrate the opportunities arising from the new urbanization policy actively promoted by China, to build a national leading brand as a comprehensive new-town-developing operator. We are a pioneer in China’s new-type of urbanization. We have established industry leadership through over ten years of solid track record since 2002, and are among the very first players to engage to primary land development. -
SGS-Safeguards 04910- Minimum Wages Increased in Jiangsu -EN-10
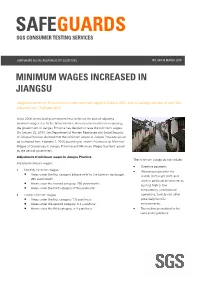
SAFEGUARDS SGS CONSUMER TESTING SERVICES CORPORATE SOCIAL RESPONSIILITY SOLUTIONS NO. 049/10 MARCH 2010 MINIMUM WAGES INCREASED IN JIANGSU Jiangsu becomes the first province to raise minimum wages in China in 2010, with an average increase of over 12% effective from 1 February 2010. Since 2008, many local governments have deferred the plan of adjusting minimum wages due to the financial crisis. As economic results are improving, the government of Jiangsu Province has decided to raise the minimum wages. On January 23, 2010, the Department of Human Resources and Social Security of Jiangsu Province declared that the minimum wages in Jiangsu Province would be increased from February 1, 2010 according to Interim Provisions on Minimum Wages of Enterprises in Jiangsu Province and Minimum Wages Standard issued by the central government. Adjustment of minimum wages in Jiangsu Province The minimum wages do not include: Adjusted minimum wages: • Overtime payment; • Monthly minimum wages: • Allowances given for the Areas under the first category (please refer to the table on next page): middle shift, night shift, and 960 yuan/month; work in particular environments Areas under the second category: 790 yuan/month; such as high or low Areas under the third category: 670 yuan/month temperature, underground • Hourly minimum wages: operations, toxicity and other Areas under the first category: 7.8 yuan/hour; potentially harmful Areas under the second category: 6.4 yuan/hour; environments; Areas under the third category: 5.4 yuan/hour. • The welfare prescribed in the laws and regulations. CORPORATE SOCIAL RESPONSIILITY SOLUTIONS NO. 049/10 MARCH 2010 P.2 Hourly minimum wages are calculated on the basis of the announced monthly minimum wages, taking into account: • The basic pension insurance premiums and the basic medical insurance premiums that shall be paid by the employers. -

Filed By: [email protected], Filed Date: 1/7/20 11:04 PM, Submission Status: Approved Page 47 of 123 Barcode:3927422-02 A-351-853 INV - Investigation
Barcode:3927422-02 A-351-853 INV - Investigation - Company Name Address E-mail Phone Website Estrada Municipal - CDR 455, S / N | km 1 Castilian 55 49 3561-3248 and 55- Adami S/A Madeiras Caçador (SC) | Postal Code 89514-899 B [email protected] 49-9184-1887 http://www.adami.com.br/ Rua Distrito Industrial - Quadra 06 - lote 03 - Setor D, Advantage Florestal Ananindeua - PA, 67035-330, Brazil [email protected] 55(91) 3017-5565 https://advantageflorestal.com.br/contact-us/ São Josafat, 1850 Street - Clover - Prudentópolis AFFONSO DITZEL & CIA LTDA Paraná - Brazil - ZIP Code 84400-000 [email protected] 55 42 3446-1440 https://www.affonsoditzel.com/index.php AG Intertrade [email protected] 55 41 3015-5002 http://www.agintertrade.com.br/en/home-2/ General Câmara Street, 243/601 55-51-2217-7344 and Araupel SA 90010-230 - Porto Alegre, RS - Brazil [email protected] 55-51-3254-8900 http://www.araupel.com.br/ Rua Félix da Cunha, 1009 – 8º andar CEP: 90570-001 [email protected] and 55 43 3535-8300 and 55- Braspine Madeiras Ltda. Porto Alegre – RS [email protected] 42-3271-3000 http://www.braspine.com.br/en/home/ R. Mal. Floriano Peixoto, 1811 - 12° andar, Sala 124 - Brazil South Lumber Centro, Guarapuava - PR, 85010-250, Brazil [email protected] 55 42 3622-9185 http://brazilsouthlumber.com.br/?lang=en Curupaitis Street, 701 - Curitiba - Paraná - Brazil - ZIP COMERCIAL EXPORTADORA WK LTDA Code 80.310-180 [email protected] http://wktrading.com.br/ 24 de Outubro Street, -

New Oriental Education & Technology Group Inc
Table of Contents UNITED STATES SECURITIES AND EXCHANGE COMMISSION Washington, D.C. 20549 FORM 20-F (Mark One) ☐ REGISTRATION STATEMENT PURSUANT TO SECTION 12(B) OR 12(G) OF THE SECURITIES EXCHANGE ACT OF 1934 OR ☒ ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(D) OF THE SECURITIES EXCHANGE ACT OF 1934 For the fiscal year ended May 31, 2011. OR ☐ TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(D) OF THE SECURITIES EXCHANGE ACT OF 1934 OR ☐ SHELL COMPANY REPORT PURSUANT TO SECTION 13 OR 15(D) OF THE SECURITIES EXCHANGE ACT OF 1934 Date of event requiring this shell company report For the transition period from to Commission file number: 001-32993 NEW ORIENTAL EDUCATION & TECHNOLOGY GROUP INC. (Exact name of Registrant as specified in its charter) N/A (Translation of Registrant’s name into English) Cayman Islands (Jurisdiction of incorporation or organization) No. 6 Hai Dian Zhong Street Haidian District, Beijing 100080 The People’s Republic of China (Address of principal executive offices) Louis T. Hsieh, President and Chief Financial Officer Tel: +(86 10) 6260-5566 E-mail: [email protected] Fax: +(86 10) 6260-5511 No. 6 Hai Dian Zhong Street Haidian District, Beijing 100080 The People’s Republic of China (Name, Telephone, E-mail and/or Facsimile number and Address of Company Contact Person) Securities registered or to be registered pursuant to Section 12(b) of the Act: Title of Each Class Name of Exchange on Which Registered American depositary shares, each representing one New York Stock Exchange common share* Common shares, par value US$0.01 per share New York Stock Exchange** * Effective August 18, 2011, the ratio of ADSs to our common shares was changed from one ADS representing four common shares to one ADS representing one common share. -

Table of Codes for Each Court of Each Level
Table of Codes for Each Court of Each Level Corresponding Type Chinese Court Region Court Name Administrative Name Code Code Area Supreme People’s Court 最高人民法院 最高法 Higher People's Court of 北京市高级人民 Beijing 京 110000 1 Beijing Municipality 法院 Municipality No. 1 Intermediate People's 北京市第一中级 京 01 2 Court of Beijing Municipality 人民法院 Shijingshan Shijingshan District People’s 北京市石景山区 京 0107 110107 District of Beijing 1 Court of Beijing Municipality 人民法院 Municipality Haidian District of Haidian District People’s 北京市海淀区人 京 0108 110108 Beijing 1 Court of Beijing Municipality 民法院 Municipality Mentougou Mentougou District People’s 北京市门头沟区 京 0109 110109 District of Beijing 1 Court of Beijing Municipality 人民法院 Municipality Changping Changping District People’s 北京市昌平区人 京 0114 110114 District of Beijing 1 Court of Beijing Municipality 民法院 Municipality Yanqing County People’s 延庆县人民法院 京 0229 110229 Yanqing County 1 Court No. 2 Intermediate People's 北京市第二中级 京 02 2 Court of Beijing Municipality 人民法院 Dongcheng Dongcheng District People’s 北京市东城区人 京 0101 110101 District of Beijing 1 Court of Beijing Municipality 民法院 Municipality Xicheng District Xicheng District People’s 北京市西城区人 京 0102 110102 of Beijing 1 Court of Beijing Municipality 民法院 Municipality Fengtai District of Fengtai District People’s 北京市丰台区人 京 0106 110106 Beijing 1 Court of Beijing Municipality 民法院 Municipality 1 Fangshan District Fangshan District People’s 北京市房山区人 京 0111 110111 of Beijing 1 Court of Beijing Municipality 民法院 Municipality Daxing District of Daxing District People’s 北京市大兴区人 京 0115 -

Results Announcement for the Year Ended December 31, 2020
(GDR under the symbol "HTSC") RESULTS ANNOUNCEMENT FOR THE YEAR ENDED DECEMBER 31, 2020 The Board of Huatai Securities Co., Ltd. (the "Company") hereby announces the audited results of the Company and its subsidiaries for the year ended December 31, 2020. This announcement contains the full text of the annual results announcement of the Company for 2020. PUBLICATION OF THE ANNUAL RESULTS ANNOUNCEMENT AND THE ANNUAL REPORT This results announcement of the Company will be available on the website of London Stock Exchange (www.londonstockexchange.com), the website of National Storage Mechanism (data.fca.org.uk/#/nsm/nationalstoragemechanism), and the website of the Company (www.htsc.com.cn), respectively. The annual report of the Company for 2020 will be available on the website of London Stock Exchange (www.londonstockexchange.com), the website of the National Storage Mechanism (data.fca.org.uk/#/nsm/nationalstoragemechanism) and the website of the Company in due course on or before April 30, 2021. DEFINITIONS Unless the context otherwise requires, capitalized terms used in this announcement shall have the same meanings as those defined in the section headed “Definitions” in the annual report of the Company for 2020 as set out in this announcement. By order of the Board Zhang Hui Joint Company Secretary Jiangsu, the PRC, March 23, 2021 CONTENTS Important Notice ........................................................... 3 Definitions ............................................................... 6 CEO’s Letter .............................................................. 11 Company Profile ........................................................... 15 Summary of the Company’s Business ........................................... 27 Management Discussion and Analysis and Report of the Board ....................... 40 Major Events.............................................................. 112 Changes in Ordinary Shares and Shareholders .................................... 149 Directors, Supervisors, Senior Management and Staff.............................. -

Effect of Birth Order on Stereoacuity in Chinese Preschool Children: a Cross- Sectional Study
Open access Original research BMJ Open: first published as 10.1136/bmjopen-2019-032833 on 12 October 2020. Downloaded from Effect of birth order on stereoacuity in Chinese preschool children: a cross- sectional study Shu Han,1 Xiaohan Zhang,2 Rui Li,3 Haohai Tong,3 Xiaoyan Zhao,3 Yue Wang,3 Qingfeng Hao,3 Dan Huang,3 Hui Zhu,3 Xiaojun Zhang,1 Hu Liu 3 To cite: Han S, Zhang X, Li R, ABSTRACT Strengths and limitations of this study et al. Effect of birth order Objective This study aimed to investigate the relationship on stereoacuity in Chinese between birth order and stereoacuity among Chinese ► To our limited knowledge, no report has demon- preschool children: a cross- children aged 60–72 months. sectional study. BMJ Open strated the correlation between birth order and Design Cross- sectional. 2020;10:e032833. doi:10.1136/ stereoacuity. Participants 1342 children with complete data on the bmjopen-2019-032833 ► With the two- child policy in China, evaluating the ef- questionnaire, stereoacuity and refraction were included. fects of this baby boom on stereoacuity might bene- ► Prepublication history for Results The mean stereoacuity was 53.2±1.7, 56.9±1.9 fit both families and the society. this paper is available online. and 60.9±1.5 s of arc in the first- born group, second- born ► This is a population- based study comprising 1342 To view these files, please visit group and third- born group, respectively. Lower birth the journal online (http:// dx. doi. children aged 60–72 months. order was significantly correlated with better stereoacuity org/ 10. -

Transmissibility of Hand, Foot, and Mouth Disease in 97 Counties of Jiangsu Province, China, 2015- 2020
Transmissibility of Hand, Foot, and Mouth Disease in 97 Counties of Jiangsu Province, China, 2015- 2020 Wei Zhang Xiamen University Jia Rui Xiamen University Xiaoqing Cheng Jiangsu Provincial Center for Disease Control and Prevention Bin Deng Xiamen University Hesong Zhang Xiamen University Lijing Huang Xiamen University Lexin Zhang Xiamen University Simiao Zuo Xiamen University Junru Li Xiamen University XingCheng Huang Xiamen University Yanhua Su Xiamen University Benhua Zhao Xiamen University Yan Niu Chinese Center for Disease Control and Prevention, Beijing City, People’s Republic of China Hongwei Li Xiamen University Jian-li Hu Jiangsu Provincial Center for Disease Control and Prevention Tianmu Chen ( [email protected] ) Page 1/30 Xiamen University Research Article Keywords: Hand foot mouth disease, Jiangsu Province, model, transmissibility, effective reproduction number Posted Date: July 30th, 2021 DOI: https://doi.org/10.21203/rs.3.rs-752604/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 2/30 Abstract Background: Hand, foot, and mouth disease (HFMD) has been a serious disease burden in the Asia Pacic region represented by China, and the transmission characteristics of HFMD in regions haven’t been clear. This study calculated the transmissibility of HFMD at county levels in Jiangsu Province, China, analyzed the differences of transmissibility and explored the reasons. Methods: We built susceptible-exposed-infectious-asymptomatic-removed (SEIAR) model for seasonal characteristics of HFMD, estimated effective reproduction number (Reff) by tting the incidence of HFMD in 97 counties of Jiangsu Province from 2015 to 2020, compared incidence rate and transmissibility in different counties by non -parametric test, rapid cluster analysis and rank-sum ratio. -

CHINA VANKE CO., LTD.* 萬科企業股份有限公司 (A Joint Stock Company Incorporated in the People’S Republic of China with Limited Liability) (Stock Code: 2202)
Hong Kong Exchanges and Clearing Limited and The Stock Exchange of Hong Kong Limited take no responsibility for the contents of this announcement, make no representation as to its accuracy or completeness and expressly disclaim any liability whatsoever for any loss howsoever arising from or in reliance upon the whole or any part of the contents of this announcement. CHINA VANKE CO., LTD.* 萬科企業股份有限公司 (A joint stock company incorporated in the People’s Republic of China with limited liability) (Stock Code: 2202) 2019 ANNUAL RESULTS ANNOUNCEMENT The board of directors (the “Board”) of China Vanke Co., Ltd.* (the “Company”) is pleased to announce the audited results of the Company and its subsidiaries for the year ended 31 December 2019. This announcement, containing the full text of the 2019 Annual Report of the Company, complies with the relevant requirements of the Rules Governing the Listing of Securities on The Stock Exchange of Hong Kong Limited in relation to information to accompany preliminary announcement of annual results. Printed version of the Company’s 2019 Annual Report will be delivered to the H-Share Holders of the Company and available for viewing on the websites of The Stock Exchange of Hong Kong Limited (www.hkexnews.hk) and of the Company (www.vanke.com) in April 2020. Both the Chinese and English versions of this results announcement are available on the websites of the Company (www.vanke.com) and The Stock Exchange of Hong Kong Limited (www.hkexnews.hk). In the event of any discrepancies in interpretations between the English version and Chinese version, the Chinese version shall prevail, except for the financial report prepared in accordance with International Financial Reporting Standards, of which the English version shall prevail. -

Risk Assessment of Urban Rainstorm Disaster Based on Multi-Layer Weighted Principal Component Analysis: a Case Study of Nanjing, China
International Journal of Environmental Research and Public Health Article Risk Assessment of Urban Rainstorm Disaster Based on Multi-Layer Weighted Principal Component Analysis: A Case Study of Nanjing, China Junfei Chen 1,2,3,* , Juan Ji 1, Huimin Wang 1,4, Menghua Deng 1 and Cong Yu 1 1 Business School, Hohai University, Nanjing 211100, China; [email protected] (J.J.); [email protected] (H.W.); [email protected] (M.D.); [email protected] (C.Y.) 2 Yangtze Institute for Conservation and Development, Hohai University, Nanjing 210098, China 3 Research Institute of Jiangsu Yangtze River Conservation and High-Quality Development, Nanjing 210098, China 4 State Key Laboratory of Hydrology-Water Resources and Hydraulic Engineering, Hohai University, Nanjing 210098, China * Correspondence: [email protected]; Tel.: +86-25-6851-4613 Received: 26 June 2020; Accepted: 29 July 2020; Published: 30 July 2020 Abstract: Nanjing city is taken as a case in this urban rainstorm disaster risk research. Using the data of meteorology and social-economy statistics of Nanjing area, the paper selected ten indicators to establish the risk assessment system of urban rainstorm disaster from the aspects of the vulnerability of hazard-affected body, the fragility of disaster-pregnant environment, and the danger of hazard factors. Multi-layer weighted principal component analysis (MLWPCA) is an extension of the principal component analysis (PCA). The MLWPCA is based on factor analysis for the division subsystem. Then the PCA is used to analyze the indicators in each subsystem and weighted to synthesize. ArcGIS is used to describe regional differences in the urban rainstorm disaster risk. -

A Perspective on Housing Price-To-Income Ratios in Nanjing, China
sustainability Article Spatial Justice of a Chinese Metropolis: A Perspective on Housing Price-to-Income Ratios in Nanjing, China Shanggang Yin 1,2, Zhifei Ma 1,2, Weixuan Song 3,* and Chunhui Liu 4 1 School of Geographical Science, Nanjing Normal University, Nanjing 210023, China; [email protected] (S.Y.); [email protected] (Z.M.) 2 Jiangsu Center for Collaborative Innovation in Geographical Information Resource Development and Application, Nanjing 210023, China 3 Nanjing Institute of Geography and Limnology, Chinese Academy of Sciences, Nanjing 210008, China 4 College of Humanities and Social Development, Nanjing Agricultural University, Nanjing 210095, China; [email protected] * Correspondence: [email protected] Received: 20 February 2019; Accepted: 20 March 2019; Published: 26 March 2019 Abstract: The housing price-to-income ratio is an important index for measuring the health of real estate, as well as detecting residents’ housing affordability and regional spatial justice. This paper considers 1833 residential districts in one main urban area and three secondary urban areas in Nanjing during the period 2009–2017 as research units. It also simulates and estimates the spatial distribution of the housing price-to-income ratio with the kriging interpolation method of geographic information system (GIS) geostatistical analysis and constructs a housing spatial justice model by using housing price, income, and housing price-to-income ratio. The research results prove that in the one main urban area and the three secondary urban areas considered, the housing price-to-income ratio tended on the whole to rise, presenting a core edge model of a progressive decrease from the Main Urban Area to the secondary urban areas spatially, with high-value areas centered around famous school districts and new town centers. -

View’, Procedia-Social and Growth of That Area
Avestia Publishing International Journal of Civil Infrastructure (IJCI) Volume 3, Year 2020 ISSN: 2563-8084 DOI: 10.11159/ijci.2020.004 Spatial Differentiation and Influencing Factors of Attended Collection and Delivery Points in Nanjing City, China Muhammad Sajid Mehmood1,2, Gang Li1,2*, Shuyan Xue1,2, Qifan Nie3, Xueyao Ma1,2, Zeeshan Zafar1,2, Adnan Rayit4 1College of Urban and Environmental Sciences, Northwest University Xi’an 710127, China 2Shaanxi Key Laboratory of Earth Surface System and Environmental Carrying Capacity, Northwest University Xi’an 710127, China *[email protected] 3Department of Civil, Construction and Environmental Engineering, University of Alabama System, Tuscaloosa 35401, USA 4Agricultural Information Institute, Graduate School Chinese Academy of Agricultural Sciences, Haidian District, Beijing 100093, China Keywords: Attended collection and delivery points, China Abstract - E-commerce and online shopping have become more Post stations, Cainiao stations, spatial pattern, convenient due to the rapid growth of the internet logistic influencing factors, Nanjing City. industry in many developed countries and is particularly popular and suitable in China. The method is primarily based on © Copyright 2020 Authors - This is an Open Access article logistic points like attended collection and delivery points published under the Creative Commons Attribution (ACDPs), an emerging industry for economic development. This License terms (http://creativecommons.org/licenses/by/3.0). article includes text analysis, descriptive statistics, and spatial Unrestricted use, distribution, and reproduction in any medium analysis to analyze the operation types, service objects, location are permitted, provided the original work is properly cited. distribution, and influencing factors of ACDPs in Nanjing City using point of interest data (POI) of Cainiao stations and China Post stations.