Measles Virus Outbreak in District Karak, KP, Pakistan
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Asian Pacific Journal of Tropical Disease
Asian Pac J Trop Dis 2017; 7(9): 531-535 531 Asian Pacific Journal of Tropical Disease journal homepage: http://www.apjtcm.com Original article https://doi.org/10.12980/apjtd.7.2017D7-89 ©2017 by the Asian Pacific Journal of Tropical Disease. All rights reserved. First detection on prevalence of Anaplasma marginale in sheep and goat in Karak District, Pakistan Mubashir Hussain1, Asif Junaid1, Rukhsana Gul2, Muhammad Ameen Jamal3, Irfan Ahmed4, Mir Zulqarnain Talpur4, Kashif Rahim5, Madiha Fatima6, Shahzad Munir7* 1Vector Borne Diseases Management Center, Department of Microbiology, Kohat University of Science and Technology, Kohat, KP, 26000, Pakistan 2Department of Chemistry, Kohat University of Science and Technology, Kohat, KP, 26000, Pakistan 3Department of Animal Breeding, Genetics and Reproduction, Yunnan Agricultural University, Kunming 650201, Yunnan, PR China 4Yunnan Provincial Key Laboratory of Animal Nutrition and Feed, Yunnan Agricultural University, Kunming 650201, Yunnan, PR China 5Beijing Key Laboratory of Genetic Engineering Drug and Biotechnology, Institute of Biochemistry and Biotechnology, College of Life Sciences, Beijing Normal University, Beijing 100875, PR China 6State Key Laboratory of Veterinary Biotechnology, Harbin Veterinary Research Institute, Chinese Academy of Agricultural Sciences, 678 Haping Road, Harbin 150069, PR China 7Faculty of Plant Protection, Yunnan Agricultural University, Kunming 650201, Yunnan, PR China ARTICLE INFO ABSTRACT Article history: Objective: To evaluate prevalence of Anaplasma marginale (A. marginale) and associated risk Received 4 May 2017 factors in sheep and goat. Received in revised form 19 May 2017 Methods: A total of 500 blood samples (250 from sheep and 250 from goat) were collected Accepted 25 Jun 2017 from three different tehsils of Karak District and analyzed for presence of A. -
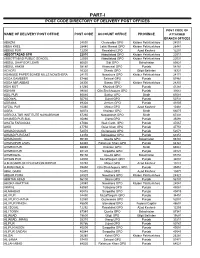
Part-I: Post Code Directory of Delivery Post Offices
PART-I POST CODE DIRECTORY OF DELIVERY POST OFFICES POST CODE OF NAME OF DELIVERY POST OFFICE POST CODE ACCOUNT OFFICE PROVINCE ATTACHED BRANCH OFFICES ABAZAI 24550 Charsadda GPO Khyber Pakhtunkhwa 24551 ABBA KHEL 28440 Lakki Marwat GPO Khyber Pakhtunkhwa 28441 ABBAS PUR 12200 Rawalakot GPO Azad Kashmir 12201 ABBOTTABAD GPO 22010 Abbottabad GPO Khyber Pakhtunkhwa 22011 ABBOTTABAD PUBLIC SCHOOL 22030 Abbottabad GPO Khyber Pakhtunkhwa 22031 ABDUL GHAFOOR LEHRI 80820 Sibi GPO Balochistan 80821 ABDUL HAKIM 58180 Khanewal GPO Punjab 58181 ACHORI 16320 Skardu GPO Gilgit Baltistan 16321 ADAMJEE PAPER BOARD MILLS NOWSHERA 24170 Nowshera GPO Khyber Pakhtunkhwa 24171 ADDA GAMBEER 57460 Sahiwal GPO Punjab 57461 ADDA MIR ABBAS 28300 Bannu GPO Khyber Pakhtunkhwa 28301 ADHI KOT 41260 Khushab GPO Punjab 41261 ADHIAN 39060 Qila Sheikhupura GPO Punjab 39061 ADIL PUR 65080 Sukkur GPO Sindh 65081 ADOWAL 50730 Gujrat GPO Punjab 50731 ADRANA 49304 Jhelum GPO Punjab 49305 AFZAL PUR 10360 Mirpur GPO Azad Kashmir 10361 AGRA 66074 Khairpur GPO Sindh 66075 AGRICULTUR INSTITUTE NAWABSHAH 67230 Nawabshah GPO Sindh 67231 AHAMED PUR SIAL 35090 Jhang GPO Punjab 35091 AHATA FAROOQIA 47066 Wah Cantt. GPO Punjab 47067 AHDI 47750 Gujar Khan GPO Punjab 47751 AHMAD NAGAR 52070 Gujranwala GPO Punjab 52071 AHMAD PUR EAST 63350 Bahawalpur GPO Punjab 63351 AHMADOON 96100 Quetta GPO Balochistan 96101 AHMADPUR LAMA 64380 Rahimyar Khan GPO Punjab 64381 AHMED PUR 66040 Khairpur GPO Sindh 66041 AHMED PUR 40120 Sargodha GPO Punjab 40121 AHMEDWAL 95150 Quetta GPO Balochistan 95151 -

Of Well at Moh: Noor Ahamd Khan Koroona Sabir Abad
District. Project Description BE 2016-17 KARAK KK15D00001-Pavement of street / PCC at UC Jandari - KARAK KK15D00002-Const: of Well at Moh: Noor Ahamd Khan Koroona Sabir Abad - KARAK KK15D00004-Const: of open Well at Paidal Khel - KARAK KK15D00008-Street Pavement at Shawa Nari Panoos - KARAK KK15D00009-Pavement of street at Sher khan kala Zebi - KARAK KK15D00011-Pavement of Street PCC at Faqiri Banda Rasool Badshah Koroona UC - Jatta Ismail Khel KARAK KK15D00012-Replacement / Maintenace of Transformer in Karak PK 40 - KARAK KK15D00013-P/Pumps functioned by Solar system for Hilly area in Tehsil BD shah - KARAK KK15D00016-Inst: / Purchase of W.S Pipeline at Pk 40 - KARAK KK15D00017-PCC road from Tormirch to Algada Bilan Kalae (Additional work) - KARAK KK15D00018-Construction of T/Well at Qabila Shakhan Alam Gul Khel Shafiq ur - Rehman Koroona KARAK KK15D00030-Solarization of EducationalInstitutions. SH: 1.GHS Sabir Abad 2. GGHS - Sabir Abad 3. GMS Sabir Abad.VC Sabir Abad KARAK KK15D00031-"Provision of missing facilities inMiddle/High Schools in UC - ShanwaGudiKhel,SH: 1.Procurement of equipmen,2. Pressure Pumps. (As per PC-I) 1. GHS: Gumbati Mina Khel. KARAK KK15D00032-Solarization of EducationalInstitutions. SH: 1.GHS: MithaKhel Rs: 0.5 - (M) 2. GHS:Tapi Kanda Rs:0.5(M) 3.GHS:Esaf Khel Rs:0.5(M)4.GGHS:Mitha Khel Rs:0.5(M) KARAK KK15D00033-Constuction of Additional Class Roomsin1.GMS: Faqir Abad. VC - KandoKhel KARAK KK15D00034-Provision of missing facilities to GHSDabbSangani. 1- Procurement of - equipment 2. Group Laterin. (As per PC-I)VC EsakChuntra. KARAK KK15D00035-"Solarization of EducationalInstitutions SH: 1-GHS: Teri 2.GMS Shagi - Teri as per PC-I. -

JLC'líl1 V 4)Ir
JLC'LíL1 V 4)ir /2O182O133 JJ 1Ji)LOJL (')S(J tIJjJI )J_IJ • 'i --- (Rs. in million) Year of Receipt 10% Share of Year of Revival of Fresh Total District Karak Release unutilized Release Release Fund (10% share) 2012-13 1321410 2013-14 271.743 1321.410 1593.153 2013-14 2047,212 2014-15 94.671 1023.500 1118.171 2014-15 1680.641 2015-16 337.718 587.445 925.163 2015-16 1216.891 2016-17 111.482 549.359 660.841 2016-17 1500.776 2017-18 0.000 315.372 315.372 2017-18 1492.960 2018-19 75.919 0.000 0.000 Grand Total 9,259.890 891 .533 3797.086 4688.619 3); ii117O.445 fli,.2O1 5-1 6iil2Ol 3-142 Financial year Fund Released (Rs. in million) 2013-14 700.000 2015-16 470.445 Total 1170.445 STATEMENT SHOWING LAST 5 YRS RECEII'TS AND RELEASES ON ACCOUNT OF 10% OIL & GAS ROYALTY TO KOHAT DIVISION (/Zc. In Miion) Actual Received from Federal Govt ADP Allocation Releases Un-released 10% District Balance Out Financial Share Financial of District District Rs. Rs. Revival Fresh Total year Year Share Kohat 4649.240 464.924 63.310 464,924 528.234 0.000 2012-13 Karak 13214.100 1321.410 271.743 1321.410 1593.153 0.000 2013-14 1960.045 Hangu 1767.367 176.736 5.177 176,736 181.913 0.000 Sub-Total 19630.707 1963.070 340.230 1963.070 2303.300 0.000 Kohat 6128.298 612.830 325.562 612.618 938.180 0.212 2013-14 Karak 20472.118 2047.212 94.671 1023.500 1118.171 1023.712 2014-15 1960.397 Hangu 4744.527 474.453 58.693 474.241 532.934 0.212 Sub-Total 31344.943 3134.494 478.926 2110.359 2589.285 1024.135 Kohat 2770.910 277.091 365.044 0.000 365.044 277.091 2014-15 Karak 16806.410 -

ADP 2021-22 Planning and Development Department, Govt of Khyber Pakhtunkhwa Page 1 of 446 NEW PROGRAMME
ONGOING PROGRAMME SECTOR : Agriculture SUB-SECTOR : Agriculture Extension 1.KP (Rs. In Million) Allocation for 2021-22 Code, Name of the Scheme, Cost TF ADP (Status) with forum and Exp. upto Beyond S.#. Local June 21 2021-22 date of last approval Local Foreign Foreign Cap. Rev. Total 1 170071 - Improvement of Govt Seed 288.052 0.000 230.220 23.615 34.217 57.832 0.000 0.000 Production Units in Khyber Pakhtunkhwa. (A) /PDWP /30-11-2017 2 180406 - Strengthening & Improvement of 60.000 0.000 41.457 8.306 10.237 18.543 0.000 0.000 Existing Govt Fruit Nursery Farms (A) /DDWP /01-01-2019 3 180407 - Provision of Offices for newly 172.866 0.000 80.000 25.000 5.296 30.296 0.000 62.570 created Directorates and repair of ATI building damaged through terrorist attack. (A) /PDWP /28-05-2021 4 190097 - Wheat Productivity Enhancement 929.299 0.000 378.000 0.000 108.000 108.000 0.000 443.299 Project in Khyber Pakhtunkhwa (Provincial Share-PM's Agriculture Emergency Program). (A) /ECNEC /29-08-2019 5 190099 - Productivity Enhancement of 173.270 0.000 98.000 0.000 36.000 36.000 0.000 39.270 Rice in the Potential Areas of Khyber Pakhtunkhwa (Provincial Share-PM's Agriculture Emergency Program). (A) /ECNEC /29-08-2019 6 190100 - National Oil Seed Crops 305.228 0.000 113.000 0.000 52.075 52.075 0.000 140.153 Enhancement Programme in Khyber Pakhtunkhwa (Provincial Share-PM's Agriculture Emergency Program). -

1 Annexure - D Names of Village / Neighbourhood Councils Alongwith Seats Detail of Khyber Pakhtunkhwa
1 Annexure - D Names of Village / Neighbourhood Councils alongwith seats detail of Khyber Pakhtunkhwa No. of General Seats in No. of Seats in VC/NC (Categories) Names of S. Names of Tehsil Councils No falling in each Neighbourhood Village N/Hood Total Col Peasants/Work S. No. Village Councils (VC) S. No. Women Youth Minority . district Council Councils (NC) Councils Councils 7+8 ers 1 2 3 4 5 6 7 8 9 10 11 12 13 Abbottabad District Council 1 1 Dalola-I 1 Malik Pura Urban-I 7 7 14 4 2 2 2 2 Dalola-II 2 Malik Pura Urban-II 7 7 14 4 2 2 2 3 Dabban-I 3 Malik Pura Urban-III 5 8 13 4 2 2 2 4 Dabban-II 4 Central Urban-I 7 7 14 4 2 2 2 5 Boi-I 5 Central Urban-II 7 7 14 4 2 2 2 6 Boi-II 6 Central Urban-III 7 7 14 4 2 2 2 7 Sambli Dheri 7 Khola Kehal 7 7 14 4 2 2 2 8 Bandi Pahar 8 Upper Kehal 5 7 12 4 2 2 2 9 Upper Kukmang 9 Kehal 5 8 13 4 2 2 2 10 Central Kukmang 10 Nawa Sher Urban 5 10 15 4 2 2 2 11 Kukmang 11 Nawansher Dhodial 6 10 16 4 2 2 2 12 Pattan Khurd 5 5 2 1 1 1 13 Nambal-I 5 5 2 1 1 1 14 Nambal-II 6 6 2 1 1 1 Abbottabad 15 Majuhan-I 7 7 2 1 1 1 16 Majuhan-II 6 6 2 1 1 1 17 Pattan Kalan-I 5 5 2 1 1 1 18 Pattan Kalan-II 6 6 2 1 1 1 19 Pattan Kalan-III 6 6 2 1 1 1 20 Sialkot 6 6 2 1 1 1 21 Bandi Chamiali 6 6 2 1 1 1 22 Bakot-I 7 7 2 1 1 1 23 Bakot-II 6 6 2 1 1 1 24 Bakot-III 6 6 2 1 1 1 25 Moolia-I 6 6 2 1 1 1 26 Moolia-II 6 6 2 1 1 1 1 Abbottabad No. -

District Karak Jamia Masajids S.No Name F/Name Mosque with Address Domicile Tehsil Sect Qualification Deeni CNIC Mobile Bank Name Branch Code Account No Education
AUQAF, HAJJ, RELIGIOUS & MINORITY AFFAIRS DEPARTMENT, KHYBER PAKHTUNKHWA Website: www.ahrma.kp.gov.pk facebook.com/ahrmadept Phone: 091–9223499 Email: [email protected] District Karak Jamia Masajids S.No Name F/Name Mosque with Address Domicile Tehsil Sect Qualification Deeni CNIC Mobile Bank Name Branch Code Account No Education 1 Farid Ullah Nais Khan Zaman Gul Gundi Killi, Kark Sunni SSC Nil 14203-20441 25-9 2 Irfan Ullah Rizwan Shah Masjid Saif Ur Rehman Kark Sunni Nil Nil 14202-46108 Gundi Killa, Chokara Karak, 49-1 3 Muhammad Mir Abbas Masjid Bilal Naqib Ullah, Kark Sunni Bachelor Shahadat Ul 0315-827697 Asif Village & Post Chokara Alamia 3 Takhte Nasrati Karak 4 Taj Wali Chandan Gul Gul Ghani Shah Gundi Killi, Kark Sunni Master Nil 14203-62303 Khan 64-5 5 Zahid Ullah Teri Khan Jamia Masjid Nasrat Abad, Kark Sunni Nil Nil 14203-24748 Nasrat Abad P/o Takhti 43-7 Nasrati, Karak 6 Masjid Abubaker Sadiq Jogi Nil Nil SSC Nil Nil Khel, 7 Masjid Farooqia, Nil Nil SSC Nil Nil 8 Jama Masjid Bilal, Nil Nil SSC Nil Nil 9 Jama Masjid Qaba., Nil Nil SSC Nil Nil 10 Jamia Masjid Khulafai Nil Nil SSC Nil Nil Rashideen (Ahmadi Banda)., 11 Jamia Masjid Usman Ghani Nil Nil SSC Nil Nil (Ahmadi Banda)., 12 Jamia Masjid Mahalla Taj Ali Nil Nil SSC Nil Nil Khan Koroona (Ahmadi Banda)., 1 / 19 13 Jamia Masjid Hazrat Bilal Nil Nil SSC Nil Nil Teri Chowk (Ahmad Banda)., 14 Jamia Masjid Khari Banda, Nil Nil SSC Nil Nil 15 Jamia Masjid (Bara), Nil Nil SSC Nil Nil 16 Jamia Masjid Qaba, Nil Nil SSC Nil Nil 17 Jamia Masjid Abu Hurera Nil Nil SSC Nil Nil Donga. -

On Students' Academic Achievement and Retention in Chemistry
Journal of Education and Educational Development Article Effects of Information and Communication Technology (ICT) on Students’ Academic Achievement and Retention in Chemistry at Secondary Level Ishtiaq Hussain Kohat University of Science & Technology [email protected] Qaiser Suleman Institute of Education & Research Kohat University of Science & Technology [email protected] Dr. M. Naseer ud Din Assistant Professor, Institute of Education & Research Kohat University of Science & Technology [email protected] [email protected] Farhan Shafique Kohat University of Science & Technology [email protected] Abstract The current paper investigated the effects of information and communication technology on the students’ academic achievement and retention in chemistry. Fifty students of 9th grade were selected randomly from Kohsar Public School and College Latamber Karak. The students were grouped into equivalent groups based on pretest score. In order to collect data, pretest posttest equivalent groups design was used. Mean, standard deviation and independent Vol. 4 No. 1 (June 2017) 73 Effects of Information and Communication Technology (ICT) samples t-test were applied through SPSS for data analysis. Based on statistical analysis, it came to light that information and communication technology positively affects students’ academic achievement and retention and ICT was found more compelling, effective and valuable in teaching of chemistry when contrasted with conventional techniques of teaching. It is recommended that information and communication technology should be used in teaching chemistry for enhancing students’ academic achievement at secondary level. Keywords: academic achievement, chemistry, Information and Communication Technology (ICT), retention, secondary level Introduction Information and technology has a major role to play in forming the new worldwide economy to deliver fast changes in the society. -

Monsoon Contingency Plan 2015
1 | P a g e Table of Contents Executive Summary ...................................................................................................................... 12 Chapter-1 ....................................................................................................................................... 14 Monsoon Contingency Plan 2015 ................................................................................................. 14 1.1 An Overview .................................................................................................................. 14 1.2 Khyber Pakhtunkhwa General and Flood Profile .......................................................... 15 1.3 Contingency Plan for Monsoon 2015............................................................................. 17 Aim ........................................................................................................................................ 17 Objectives: ............................................................................................................................ 17 Scope ..................................................................................................................................... 18 Lessons Learnt from PreviousFloods .................................................................................... 18 1.4 Addressing Vulnerability in Monsoon Contingency Planning ..................................... 20 Chapter-2 ...................................................................................................................................... -

KK15D00056-"Water Supply Schemes Atghsgarangsirajkhel, and Constr GGMS Wankisirajkhel As Per PC-I. Vcwankisirajkhel"
DISTRICT Project Description BE 2018-19 KARAK KK15D00056-"Water Supply Schemes atGHSGarangSirajKhel, and Constr GGMS - WankiSirajKhel as per PC-I. VCWankiSirajKhel" KARAK KK15D00063-Maintenance and repair of BHU jattaIsmail Khel as per PC-I. VC Jatta Ismail - Khel KARAK KK15D00064-Provision of solar panel to RHC HospitalJ.I.Khelas per PC-I. VC Jatta Ismail Khel - KARAK KK15D00111-"Installation of Pressure Pumps in UCJatta Ismail Khel as per PC-I. 1- Jatta - Ismail Khel 2. Makoori 3 MamiKhel " KARAK KK15D00119-"P/F of Pipe dia, 3"", 2"", and1-1/2""as per PC-I VCTeri, VC EsakKhumari - " KARAK KK15D00147-"Construction of PCC Road/Reconstruction/Repair of Streets,as per PC-I. VC - Jehngiri, VCYaghiMuskan, VC Khojaki. " KARAK KK15D00152-"Construction of PCC Road/ pavement ofstreets as per PC-I. VC Janderi, VC - SaratKhel, VC DhodaKhel, VC TarkhaKoi " KARAK KK15D00153-"WSS InstalllationofTubewell at AjabNoor Koroona, Show Banda as per PC-1. - VC Chokara" KARAK KK15D00158-Shingle Road/PCC Road/StreetPavement/Kacha Track as per PC-I EsakChuntra - KARAK KK15D00162-Construction of Group Laterin in GHSGandariKhattak as per PC-I. VC - GandariKhattak. KARAK KK15D00169-Repair/Rehabilitation/Renovation/Furniture of Circuit House Karakas per PC-I - Circuit House Karak KARAK KK15D00175-PCC Road from Main Bazar to GGHSSabirAbadas per PC-I. VC Sabir Abad - KARAK KK15D00178-"District Nazim Directive (SpecialInitiatives) (Installation of Pressure Pumps, - Hand Pumps, Pavement ofstreets, replacement of old pipes, installation of new pipes, KARAK KK16D00030-Installation of Pressure Pumps at Tehsil Karak - KARAK KK16D00031-Pavement of Streets at Tehsil Karak - KARAK KK16D00032-Open Well along with Solarization at GurGuri Eidal Khel - KARAK KK16D00033-Construction of Retaining Wall at Ghundi Shahbaz Khan and Lakkana - KARAK KK16D00034-REpair / Renovation / Improvement / Rehabilitation and solarization of - emergency &children Ward of Women & Children Hospital Karak KARAK KK16D00061-"Provision of Drinking water to BHUShagi Lawagher. -

Curriculum Vitae
AUDIT REPORT ON THE ACCOUNTS OF DISTRICT GOVERNMENT KARAK AUDIT YEAR 2012-13 AUDITOR GENERAL OF PAKISTAN TABLE OF CONTENTS ABBREVIATIONS AND ACRONYMS .........................................................................................i Preface ............................................................................................................................................. ii EXECUTIVE SUMMARY ............................................................................................................ iii SUMMARY TABLES & CHARTS ............................................................................................. vii Table 1: Audit Work Statistics ................................................................................................. vii Table 2: Audit observation Classified by Categories ............................................................... vii Table 3: Outcome Statistics ..................................................................................................... viii Table 4: Table of Irregularities pointed out ................................................................................ix CHAPTER 1 .................................................................................................................................... 1 1.1 District Government Karak ......................................................................................... 1 1.1.1 Introduction of Departments ....................................................................................... 1 1.1.2 -

Table of Contents
TABLE OF CONTENTS ABBREVIATIONS AND ACRONYMS ............................................................ ii Preface .................................................................................................................. iii EXECUTIVE SUMMARY ................................................................................. iv SUMMARY TABLES & CHARTS .................................................................. vii Table 1: Audit Work Statistics ......................................................................... vii Table 2: Audit observation Classified by Categories ....................................... vii Table 3: Outcome Statistics ............................................................................. viii Table 4: Table of Irregularities pointed out ...................................................... ix Table 5: Cost Benefit Ratio…………………………………………………......x CHAPTER 1 ......................................................................................................... 1 1.1 District Government Karak ................................................................. 1 1.1.1 Introduction ......................................................................................... 1 1.1.2 Brief comments on Budget and Expenditure (Variance Analysis) ...... 1 1.1.3 Brief comments on the status of compliance with ZAC / PAC Directives ........................................................................................................... 2 1.2 AUDIT PARAS ..............................................................................................