Pulp Therapy for Primary and Immature Permanent Teeth
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pdf (930.25 K)
EGYPTIAN Vol. 64, 951:962, April, 2018 DENTAL JOURNAL I.S.S.N 0070-9484 Orthodontics, Pediatric and Preventive Dentistry www.eda-egypt.org • Codex : 214/1804 CLINICAL AND RADIOGRAPHIC ASSESSMENT OF PULPOTOMY MATERIALS IN PRIMARY MOLARS Gihan Abuelniel* and Sherif Eltawil* ABSTRACT Aim or purpose: Clinical and radiographic evaluation of four different materials utilized in vital pulpotomy in mandibular primary molars Materials and methods: one hundred and sixty mandibular primary molars in forty children were included as split mouth design. Patients were medically free with an age range from 4-6 years. Inclusion criteria: patients presented with deep carious lesions including the first and second primary molars bilaterally, no evidence of any clinical pathology, mobility and had no tenderness to percussion. Pre-operative radiographs showed no evidence of external or internal root resorption, absence of furcal, periapical radiolucency or widened periodontal ligament space and no more than one-third root resorption detected. The included molars undergone vital pulp therapy and bilaterally randomly divided into four equal groups, group (1) formocresol, group (2) ferric sulphate, group (3) MTA (mineral trioxide aggregate) and group (4) Metapex (calcium hydroxide &iodoform). All treated molars were evaluated both clinically and radiographically for 12 months evaluation period. Data were collected and analysed statistically. Results: It was shown that, at base line, there was no statistically significant difference between clinical as well as radiographic success rates among the four groups. After 3 as well as 6 months, there was a statistically significant difference between clinical and radiographic success rates among the four groups. FS, MTA and Metapex groups showed higher clinical and radiographic success rates than FC group. -

Scientific Article
Scientific Article Prosthodontic and surgical considerations for pediatric patients requiring maxillectomy Jack W. Martin, DDS, MS Mark S. Chambers, DMD, MS James C. Lemon, DDS Bela B. Toth, MS, DDS John F. Helfrick, DDS, MS Abstract head and neck tumors of the maxillofacial region. In The quality of treatment and rehabilitation for the head such diseases, the principal treatment option is surgi- and neck cancer patient, especially the pediatric patient, cal resection of the maxilla (maxillectomy), which may has progressed markedly over the years due to the coopera- produce pronounced deficits and cosmetic deformi- tion of specialists involved in the total care of the patient. ties. Consequently, when a maxillectomy is required Defects of the oral cavity caused by trauma or removal of for treating benign or malignant disease, the maxillofa- malignant or benign tissue require special treatment con- cial prosthodontist must be included in the assessment siderations with the pediatric patient. Aside from radiation of the patient prior to surgery. Many articles describe and chemotherapy, other forms of adjuvant therapy, such the surgical and prosthodontic management of the adult as physical therapy, and patient and family counseling, are maxillectomy patient, but little information exists about needed for proper rehabilitation. In addition, oral hygiene management of the pediatric maxillectomy patient. This is essential in the overall rehabilitative process. Pediatric article discusses preoperative evaluation, and surgical dental, orthodontic, prosthodontic, and oral and maxillofa- and prosthodontic considerations of children diagnosed cial surgery specialties become integrated in treating the with maxillary cancer or benign disease. Postsurgical pediatricpatient. The concentrated multidisciplinary treat- care and growth considerations also are presented. -

Deciduous Teeth Overview
Deciduous Teeth Overview: ● Deciduous teeth are the first set of teeth a person has. They are a total of 20. ● It is important to learn about the teething stage to help make it a less painful and irritating experience for children. ● Most common problems for deciduous teeth: Caries (cavities), pain and infection, thumb sucking and using a pacifier for longer than the average age. ● A child’s face and teeth may also be injured, affecting the permanent tooth that would replace the injured primary tooth. ● Care guidelines for children’s teeth and mouths should be followed and taken seriously. What are primary teeth? They are the first set of teeth a person has and they remain until it is time for them to fall and be replaced by permanent teeth. Number: 20 teeth Other names: Baby teeth, shed teeth, temporary teeth, primary teeth, milk teeth. Importance of deciduous teeth: ● They help the child chew food. ● They aid speed and enunciation. ● Primary teeth occupy a place in the mouth so they can later allow permanent teeth to appear in their correct place. When a child loses a primary tooth prematurely, this may affect the shape and order of the permanent teeth. ● They help with a child’s aesthetic and increase confidence while smiling When do deciduous teeth appear and when do they shed? Deciduous teeth start appearing gradually starting the age of 6-7 months, beginning with the lower jaw. They are fully developed at the age of 2.5. Development of deciduous teeth (teething): Teething is when a child starts to develop his/her first teeth. -
Clinical SHOWCASE Unintentional Replantation: a Technique to Avoid
Clinical SHOWCASE Unintentional Replantation: A Technique to Avoid Robert S. Roda, DDS, MS any times in a dentist’s career, he the greatest contour of the alveolar or she will make a decision that swelling was over the upper left cuspid. Mhas unintended consequences. In Both teeth had been prepared as bridge the case reported here, some quick abutments, but the temporary bridge was thinking was required to resolve the out- not present. There was an open come of an unexpected series of events. endodontic access in the premolar with Because clinical learning is best achieved no pulp exposure and a small composite by retrospective analysis, a list of lessons resin restoration in the cuspid. Both the to be learned from this case is also pro- cuspid and the second premolar were vided, in the hope that it helps readers to tender to percussion. The cuspid was also avoid this particular situation. very tender to bite (determined with a Tooth Slooth instrument, Professional Case Report Results Inc, Laguna Niguel, Calif.) and to A 63-year-old woman presented with buccal alveolar palpation. The premolar severe pain and extraoral facial swelling in The articles for this was not tender to bite or palpation. The the upper left quadrant, which had begun month’s “Clinical cuspid did not respond to cold tests, the day before the visit and was wors- Showcase” section were whereas the premolar was hyperrespon- ening. Her medical history was noncon- written by speakers sive but with nonlingering pain consistent at the 2006 CDA Annual tributory except for mitral valve prolapse with reversible pulpitis. -

Oral Diagnosis: the Clinician's Guide
Wright An imprint of Elsevier Science Limited Robert Stevenson House, 1-3 Baxter's Place, Leith Walk, Edinburgh EH I 3AF First published :WOO Reprinted 2002. 238 7X69. fax: (+ 1) 215 238 2239, e-mail: [email protected]. You may also complete your request on-line via the Elsevier Science homepage (http://www.elsevier.com). by selecting'Customer Support' and then 'Obtaining Permissions·. British Library Cataloguing in Publication Data A catalogue record for this book is available from the British Library Library of Congress Cataloging in Publication Data A catalog record for this book is available from the Library of Congress ISBN 0 7236 1040 I _ your source for books. journals and multimedia in the health sciences www.elsevierhealth.com Composition by Scribe Design, Gillingham, Kent Printed and bound in China Contents Preface vii Acknowledgements ix 1 The challenge of diagnosis 1 2 The history 4 3 Examination 11 4 Diagnostic tests 33 5 Pain of dental origin 71 6 Pain of non-dental origin 99 7 Trauma 124 8 Infection 140 9 Cysts 160 10 Ulcers 185 11 White patches 210 12 Bumps, lumps and swellings 226 13 Oral changes in systemic disease 263 14 Oral consequences of medication 290 Index 299 Preface The foundation of any form of successful treatment is accurate diagnosis. Though scientifically based, dentistry is also an art. This is evident in the provision of operative dental care and also in the diagnosis of oral and dental diseases. While diagnostic skills will be developed and enhanced by experience, it is essential that every prospective dentist is taught how to develop a structured and comprehensive approach to oral diagnosis. -

Endodontic Therapy of Maxillary Second Molar Showing an Unusual Internal Anatomy
ISSN: Printed version: 1806-7727 Electronic version: 1984-5685 RSBO. 2012 Apr-Jun;9(2):213-7 Case Report Article Endodontic therapy of maxillary second molar showing an unusual internal anatomy Carlos Eduardo Fontana1 Carolina Davoli Macedo Ibanéz2 Felipe Davini1 Alexandre Sigrist De Martin1 Cláudia Fernandes de Magalhães Silveira1 Daniel Guimarães Pedro Rocha1 Carlos Eduardo da Silveira Bueno1 Corresponding author: Carlos Eduardo Fontana Avenida 02, n.º 1.220 CEP 13500-411 – Rio Claro – SP – Brasil E-mail: [email protected] 1 Department of Endodontics, São Leopoldo Mandic Post-graduation Center – Campinas – SP – Brazil. 2 Private practice – São Paulo – SP – Brazil. Received for publication: October 10, 2011. Accepted for publication: November 11, 2011. Abstract Keywords: internal anatomy; endodontic Introduction: The knowledge of the complex anatomy of maxillary treatment; maxillary molars and location of extra canals are essential for diagnosis second molar; dental and endodontic treatment success. Objective: The purpose of this operating microscope. study was to report a clinical case showing a varying number of palatal roots in a second maxillary molar with the aid of operating microscope (OM). Case report: A four-rooted maxillary permanent second molar with 2 separated palatal canals undergone endodontic therapy. After endodontic access, examination of the chamber floor using an operating microscope revealed two distinct palatal canals orifices. A radiograph was taken after the working lengths of each canal were estimated by means of an electronic apex locator which clearly identified the four roots with independent four canals. The canals were instrumented with ProTaper™ rotatory instruments under irrigation with 5% sodium hypochlorite, obturated with Pulp Canal Sealer® and continue wave technique. -

Apexification of Immature Permanent Incisors Using MTA and Calcium Hydroxide- Case Report
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 19, Issue 4 Ser.7 (April. 2020), PP 33-37 www.iosrjournals.org Apexification of Immature Permanent Incisors using MTA and Calcium hydroxide- Case Report Tanu Rajain1, Kesang Tsomu2, Ritu Namdev3 1Post Graduate Trainee 2nd year , Department of Pedodontics and Preventive Dentistry, PGIDS , Rohtak, Haryana. 2Post Graduate Trainee 3rd year , Department of Pedodontics and Preventive Dentistry, PGIDS , Rohtak, Haryana. 3Senior Professor and Head, Department of Pedodontics and Preventive Dentistry, PGIDS , Rohtak, Haryana. Corresponding Author: Dr. Tanu Rajain , Department of Pedodontics and Preventive Dentistry, Pt. B.D. Sharma PGIMS , Rohtak , Haryana- 124001, India. Abstract- In young pediatric patient the endodontic management of immature non vital permanent teeth is a great challenge to dentist. There is difficulty in debridement and obturation as the walls of the root canals are frequently divergent and open apexes are present. Apexification is a technique to generate a calcific barrier in a root with an open apex or the sustained apical development of an incomplete root in teeth with necrotic pulp. The most commonly advocated medicament is calcium hydroxide although recently considerable interest has been expressed in the use of MTA. In this case series both calcium hydroxide and MTA were used successfully for apexification procedure in teeth with open apex. Keywords- Young permanent maxillary incisor, open apex, calcium hydroxide, mineral trioxide aggregate, apexification. ----------------------------------------------------------------------------------------------------------------------------- ---------- Date of Submission: 04-04-2020 Date of Acceptance: 20-04-2020 ----------------------------------------------------------------------------------------------------------------------------- ---------- I. Introduction Dental trauma in the young adolescent patient is most common to the anterior dentition. -

New Treatment Option for an Incomplete Vertical Root Fracture-A
Hadrossek and Dammaschke Head & Face Medicine 2014, 10:9 http://www.head-face-med.com/content/10/1/9 HEAD & FACE MEDICINE CASE REPORT Open Access New treatment option for an incomplete vertical root fracture–a preliminary case report Paul Henryk Hadrossek and Till Dammaschke* Abstract Instead of extraction this case report presents an alternative treatment option for a maxillary incisor with a vertical root fracture (VRF) causing pain in a 78-year-old patient. After retreatment of the existing root canal filling the tooth was stabilized with a dentine adhesive and a composite restoration. Then the tooth was extracted, the VRF gap enlarged with a small diamond bur and the existing retrograde root canal filling removed. The enlarged fracture line and the retrograde preparation were filled with a calcium-silicate-cement (Biodentine). Afterwards the tooth was replanted and a titanium trauma splint was applied for 12d. A 24 months clinical and radiological follow-up showed an asymptomatic tooth, reduction of the periodontal probing depths from 7 mm prior to treatment to 3 mm and gingival reattachment in the area of the fracture with no sign of ankylosis. Hence, the treatment of VRF with Biodentine seems to be a possible and promising option. Keywords: Biodentine, Calcium silicate cement, MTA, Treatment, Vertical root fracture Background attempt to preserve teeth with VRF by using MTA was Vertical root fractures (VRF) are fractures of enamel and rejected [4]. Hence, until today, no valid treatment op- dentine along the long axis of the tooth towards the apex tion to preserve teeth with VRF can be recommended. -

June 2000 Issue the Providers' News 1 To
To: All Providers From: Provider Network Operations Date: June 21, 2000 Please Note: This newsletter contains information pertaining to Arkansas Blue Cross Blue Shield, a mutual insurance company, it’s wholly owned subsidiaries and affiliates (ABCBS). This newsletter does not pertain to Medicare. Medicare policies are outlined in the Medicare Providers’ News bulletins. If you have any questions, please feel free to call (501)378-2307 or (800)827-4814. What’s Inside? "Any five-digit Physician's Current Procedural Terminology (CPT) codes, descriptions, numeric ABCBS Fee Schedule Change 1 modifiers, instructions, guidelines, and other material are copyright 1999 American Medical Association. All Anesthesia Base Units 2 Rights Reserved." Claims Imaging and Eligibility 2 ABCBS Fee Schedule Change Reminder: Effective July 1, 2000 Arkansas Blue Cross Claims Payment Issues 3 Blue Shield is updating the fee schedule used to price professional claims. The update includes changes in the Coronary Artery Intervention 2 Relative Value Units used to calculate the maximum allowances as well as the implementation of Site-Of - CPT Code 99070 2 Service (SOS) pricing. Dental Fee Schedule 2 Under SOS pricing, a given procedure may have different allowances when provided in a setting other Electronic Filing Reminder 2 than the office. Health Advantage Referral Reminder 2 The Place Of Service reported in block 24b on the HCFA 1500 claim form indicates which allowance should be Type of Service Corrections 3 applied. An “11” in this field indicates that the service was delivered in the office setting. Any value other than Attachments “11” in block 24b will result in the application of the SOS A Guide to the HCFA - 1500 Claim Form pricing, if there is an applicable SOS allowance for that (Paper Claims) 7 service. -

Maxillary Lateral Incisor Agenesis and Its Relationship to Overall Tooth Size Jane Wright, DDS, MS,A Jose A
RESEARCH AND EDUCATION Maxillary lateral incisor agenesis and its relationship to overall tooth size Jane Wright, DDS, MS,a Jose A. Bosio, BDS, MS,b Jang-Ching Chou, DDS, MS,c and Shuying S. Jiang, MSd Prosthodontists, orthodontists, ABSTRACT and general dentists frequently fi Statement of problem. Agenesis of the maxillary lateral incisor has been linked to differences in encounter dif culties when the size of the remaining teeth. Thus, the mesiodistal space required for definitive esthetic resto- attempting to restore the oc- ration in patients with missing maxillary lateral incisors may be reduced. clusion if unilateral or bilateral Purpose. The purpose of this study was to determine whether a tooth size discrepancy exists in maxillary lateral incisors are orthodontic patients with agenesis of one or both maxillary lateral incisors. congenitally missing. Restora- tion of the missing lateral Material and methods. Forty sets of dental casts from orthodontic patients (19 men and 21 women; mean 15.9 years of age; all of European origin) were collected. All casts had agenesis of one incisor using an implant- or both maxillary lateral incisors. Teeth were measured with a digital caliper at their greatest supported crown, a partial mesiodistal width and then compared with those of a control group matched for ethnicity, age, and fi xed dental prosthesis, or sex. Four-factor ANOVA with repeated measures of 2 factors was used for statistical analysis (a=.05). mesial movement of the Results. Orthodontic patients with agenesis of one or both maxillary lateral incisors exhibited canine are treatment options. smaller than normal tooth size compared with the control group. -

Apicoectomy Treatment
INFORMED CONSENT DISCUSSION FOR APICOECTOMY TREATMENT Patient Name: Date: DIAGNOSIS: Patient’s initials required Twisted, curved, accessory or blocked canals may prevent removal of all inflamed or infected pulp/nerve during root canal treatment. Since leaving any pulp/nerve in the root canal may cause your symptoms to continue or worsen, this might require an additional procedure called an apicoectomy. Through a small opening cut in the gums and surrounding bone, any infected tissue is removed and the root canal is sealed, which is referred to as a retrofilling procedure. An apicoectomy may also be required if your symptoms continue after root canal therapy and the tooth does not heal. Benefits of Apicoectomy, Not Limited to the Following: Apicoectomy treatment is intended to help you keep your tooth, allowing you to maintain your natural bite and the healthy functioning of your jaw. This treatment has been recommended to relieve the symptoms of the diagnosis described above. Risks of Apicoectomy, Not Limited to the Following: I understand that following treatment I may experience bleeding, pain, swelling and discomfort for several days, which may be treated with pain medication. It is possible that infection may accompany treatment and must be treated with antibiotics. I will immediately contact the office if my condition worsens or if I experience fever, chills, sweats or numbness. I understand that I may receive a local anesthetic and/or other medication. In rare instances patients have a reaction to the anesthetic, which may require emergency medical attention, or find that it reduces their ability to control swallowing. This increases the chance of swallowing foreign objects during treatment. -
A Case of Periradicular Surgery: Apicoectomy and Obturation of the Apex, a Bold Act
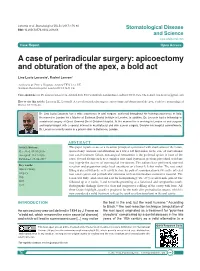
Locurcio et al. Stomatological Dis Sci 2017;1:76-80 DOI: 10.20517/2573-0002.2016.08 Stomatological Disease and Science www.sdsjournal.com Case Report Open Access A case of periradicular surgery: apicoectomy and obturation of the apex, a bold act Lino Lucio Locurcio1, Rachel Leeson2 1Ashford & St. Peter‘s Hospitals, Ashford TW15 3AA, UK. 2Eastman Dental Hospital, London WC1X 8LD, UK. Correspondence to: Dr. Lino Lucio Locurcio, Ashford & St. Peter’s Hospitals, London Road, Ashford TW15 3AA, UK. E-mail: [email protected] How to cite this article: Locurcio LL, Leeson R. A case of periradicular surgery: apicoectomy and obturation of the apex, a bold act. Stomatological Dis Sci 2017;1:76-80. Dr. Lino Lucio Locurcio has a wide experience in oral surgery, achieved throughout his training experience in Italy. He moved to London for a Master at Eastman Dental Institute in London. In addition, Dr. Locurcio had a fellowship in craniofacial surgery at Great Ormond Street Children Hospital. At the moment he is working in London as oral surgeon and implantologist with a special interest in maxillofacial and skin cancer surgery. Besides his hospital commitments, Dr. Locurcio currently works in a private clinic in Battersea, London. ABSTRACT Article history: This paper reports a case of a recurrent periapical cyst treated with enucleation of the lesion, Received: 08-10-2016 apicoectomy, and root end obturation on a lower left first molar. In the case of conventional Accepted: 21-12-2016 root canal treatment failure, non-surgical retreatment is the preferred option in most of the Published: 29-06-2017 cases.