Ultrasound Therapy for Recurrent Noninfective Olecranon Bursitis: a Case Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Are There Effective Ultrasound Parameters in the Management of Lateral Elbow Tendinopathy? a Systematic Review of the Literature
hysical M f P ed l o ic a in n r e u & International Journal of o Stasinopoulos et al., Int J Phys Med Rehabil 2013, 1:3 R J l e a h n DOI: 10.4172/2329-9096.1000117 a o b i t i l a ISSN: 2329-9096i t a n r t i e o t Physical Medicine & Rehabilitation n n I Research Article Open Access Are there Effective Ultrasound Parameters in the Management of Lateral Elbow Tendinopathy? A Systematic Review of the Literature Stasinopoulos Dimitrios*, Cheimonidou Areti-Zoe and Chatzidamianos Theodoros Program of Physiotherapy, Department of Health Sciences, School of Sciences European University of Cyprus 6, Diogenes Str. Engomi, P. O. Box 22006, 1516, Nicosia, Cyprus Abstract Objective: Lateral elbow tendinopathy (LET) is a common clinical condition, and a wide array of physiotherapy treatments is used for treating LET. One of the most common physiotherapy modality is the ultrasound. Ultrasound is a dose response modality. The aim of the present article was to determine the effective ultrasound parameters in the management of (LET) and to provide recommendations based on this evidence. Methods: Randomized controlled trials (RCTs) identified by a search strategy in six databases were used in combination with reference checking. RCTs that included positive effects with ultrasound, description of ultrasound parameters in details, patients with LET, and at least one of the clinically relevant outcome measure were selected. The Pedro scale was used to analyse the results. Results: None RCTs fulfilled the criteria and therefore all the conducted trials were excluded in the review. -
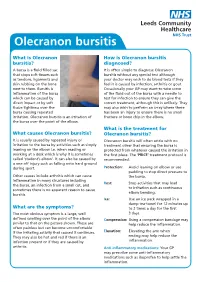
Olecranon Bursitis
Olecranon bursitis What is Olecranon How is Olecranon bursitis bursitis? diagnosed? A bursa is a fluid filled sac It is often simple to diagnose Olecranon that stops soft tissues such bursitis without any special test although as tendons, ligaments and your doctor may wish to do blood tests if they skin rubbing on the bone feel it is caused by infection, arthritis or gout. next to them. Bursitis is Occasionally your GP may want to take some inflammation of the bursa of the fluid out of the bursa with a needle to which can be caused by test for infection to ensure they can give the direct impact or by soft correct treatment, although this is unlikely. They tissue tightness over the may also wish to perform an x-ray where there bursa causing repeated has been an injury to ensure there is no small irritation. Olecranon bursitis is an irritation of fracture or bone chip in the elbow. the bursa over the point of the elbow. What is the treatment for What causes Olecranon bursitis? Olecranon bursitis? It is usually caused by repeated injury or Olecranon bursitis will often settle with no irritation to the bursa by activities such as simply treatment other that ensuring the bursa is leaning on the elbow i.e. when reading or protected from whatever caused the irritation in working at a desk which is why it is sometimes the first place. The ‘PRICE’ treatment protocol is called ‘student’s elbow’. It can also be caused by recommended: a one off injury such as falling onto hard ground during sport. -

OES Site Color Scheme 1
Nuisance Problems You will Grow to Love Thomas V Gocke, MS, ATC, PA-C, DFAAPA President & Founder Orthopaedic Educational Services, Inc. Boone, NC [email protected] www.orthoedu.com Orthopaedic Educational Services, Inc. © 2016 Orthopaedic Educational Services, Inc. all rights reserved. Faculty Disclosures • Orthopaedic Educational Services, Inc. Financial Intellectual Property No off label product discussions American Academy of Physician Assistants Financial PA Course Director, PA’s Guide to the MSK Galaxy Urgent Care Association of America Financial Intellectual Property Faculty, MSK Workshops Ferring Pharmaceuticals Consultant Orthopaedic Educational Services, Inc. © 2016 Orthopaedic Educational Services, Inc. all rights reserved. 2 LEARNING GOALS At the end of this sessions you will be able to: • Recognize nuisance conditions in the Upper Extremity • Recognize nuisance conditions in the Lower Extremity • Recognize common Pediatric Musculoskeletal nuisance problems • Recognize Radiographic changes associates with common MSK nuisance problems • Initiate treatment plans for a variety of MSK nuisance conditions Orthopaedic Educational Services, Inc. © 2016 Orthopaedic Educational Services, Inc. all rights reserved. Inflammatory Response Orthopaedic Educational Services, Inc. © 2016 Orthopaedic Educational Services, Inc. all rights reserved. Inflammatory Response* When does the Inflammatory response occur: • occurs when injury/infection triggers a non-specific immune response • causes proliferation of leukocytes and increase in blood flow secondary to trauma • increased blood flow brings polymorph-nuclear leukocytes (which facilitate removal of the injured cells/tissues), macrophages, and plasma proteins to injured tissues *Knight KL, Pain and Pain relief during Cryotherapy: Cryotherapy: Theory, Technique and Physiology, 1st edition, Chattanooga Corporation, Chattanooga, TN 1985, p 127-137 Orthopaedic Educational Services, Inc. © 2016 Orthopaedic Educational Services, Inc. -

Sports Medicine Examination Outline
Sports Medicine Examination Content I. ROLE OF THE TEAM PHYSICIAN 1% A. Ethics B. Medical-Legal 1. Physician responsibility 2. Physician liability 3. Preparticipation clearance 4. Return to play 5. Waiver of liability C. Administrative Responsibilities II. BASIC SCIENCE OF SPORTS 16% A. Exercise Physiology 1. Training Response/Physical Conditioning a.Aerobic b. Anaerobic c. Resistance d. Flexibility 2. Environmental a. Heat b.Cold c. Altitude d.Recreational diving (scuba) 3. Muscle a. Contraction b. Lactate kinetics c. Delayed onset muscle soreness d. Fiber types 4. Neuroendocrine 5. Respiratory 6. Circulatory 7. Special populations a. Children b. Elderly c. Athletes with chronic disease d. Disabled athletes B. Anatomy 1. Head/Neck a.Bone b. Soft tissue c. Innervation d. Vascular 2. Chest/Abdomen a.Bone b. Soft tissue c. Innervation d. Vascular 3. Back a.Bone b. Soft tissue c. Innervation 1 d. Vascular 4. Shoulder/Upper arm a. Bone b. Soft tissue c. Innervation d. Vascular 5. Elbow/Forearm a. Bone b. Soft tissue c. Innervation d. Vascular 6. Hand/Wrist a. Bone b. Soft tissue c. Innervation d. Vascular 7. Hip/Pelvis/Thigh a. Bone b. Soft tissue c. Innervation d. Vascular 8. Knee a. Bone b. Soft tissue c. Innervation d. Vascular 9. Lower Leg/Foot/Ankle a. Bone b. Soft tissue c. Innervation d. Vascular 10. Immature Skeleton a. Physes b. Apophyses C. Biomechanics 1. Throwing/Overhead activities 2. Swimming 3. Gait/Running 4. Cycling 5. Jumping activities 6. Joint kinematics D. Pharmacology 1. Therapeutic Drugs a. Analgesics b. Antibiotics c. Antidiabetic agents d. Antihypertensives e. -
2019 State of the Field Report in Part Or Its Entirety
State of 20the Field 19 Focused Ultrasound The Focused Ultrasound Foundation encourages widespread No part of this report may be reproduced for commercial purposes in any written, distribution of the 2019 State of the Field Report in part or its entirety. electronic, recording, or photocopy form or stored in a retrieval system without the written permission of the Focused Ultrasound Foundation. Inquiries for reproduction can be directed to Emily White at The Focused Ultrasound Foundation strives to provide the most accurate information [email protected]. possible and therefore works proactively with the manufacturers and research sites to collect the most current data available in advance of the release of this publication. Date 8.6.0019 This report is based on data through December 31, 2018. The Focused Ultrasound © 2019 Focused Ultrasound Foundation. All rights reserved. Foundation assumes no responsibility for any errors or omissions as every precaution has been taken to verify the accuracy of the information contained herein. No liability is assumed for damages that may result from the use of information contained within. If you note something out of date or inaccurate, please submit the new information/updates to: [email protected]. 3 Focused Ultrasound Foundation | State of the Field 2019 CONTENTS 2 Introduction 59 Veterinary Medicine 2 Letter From the Chairman 59 FUS Veterinary Applications 3 Focused Ultrasound in Brief 60 State of Research by Indication 4 Overview 60 Developmental Landscape 4 State of Research and -

Extracorporeal Shockwave Therapy Versus Ultrasound Therapy For
medRxiv preprint doi: https://doi.org/10.1101/2020.09.20.20198168; this version posted September 22, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. It is made available under a CC-BY-ND 4.0 International license . Extracorporeal Shockwave Therapy Versus Ultrasound Therapy for Plantar Fasciitis: Systematic Review and Meta-Analysis Zeyana Al-Siyabi1*, Mohammad Karam2*, Ethar Al-Hajri1, Abdulmalik Alsaif2 1 Podiatry BSc (Hons), University of Huddersfield, Huddersfield, United Kingdom. 2 Department of Medicine, University of Leeds, Leeds, United Kingdom. * Z.A. and M.K. contributed equally as first co-authors. Corresponding Author: Mohammad Karam Address: Al-Firdous, Block 4, Street 1, Avenue 6, Al-Farwaniyah, State of Kuwait. Phone: +965 9916272, +44 7480644489 Email: [email protected] NOTE: This preprint reports new research that has not been certified by peer review and should not be used to guide clinical practice. 1 medRxiv preprint doi: https://doi.org/10.1101/2020.09.20.20198168; this version posted September 22, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. It is made available under a CC-BY-ND 4.0 International license . Abstract Objective To compare the outcomes of Extracorporeal Shockwave Therapy (ESWT) versus Ultrasound Therapy (UST) in plantar fasciitis. Methods A systematic review and meta-analysis were performed. An electronic search identifying studies comparing ESWT and UST for plantar fasciitis was conducted. -

Download Versus Arthritis
Elbow pain Elbow pain information booklet Contents How does the elbow work? 4 What causes elbow pain and stiffness? 6 Should I see a healthcare professional? 8 What can I do to help myself? 9 How are elbow problems diagnosed? 12 What treatments are there for elbow pain? 14 Specific elbow conditions 18 Glossary 26 Research and new developments 27 Keeping active with elbow pain 28 Where can I find out more? 32 We’re the 10 million people living with arthritis. We’re the carers, researchers, health professionals, friends and parents all united in Talk to us 33 our ambition to ensure that one day, no one will have to live with the pain, fatigue and isolation that arthritis causes. We understand that every day is different. We know that what works for one person may not help someone else. Our information is a collaboration of experiences, research and facts. We aim to give you everything you need to know about your condition, the treatments available and the many options you can try, so you can make the best and most informed choices for your lifestyle. We’re always happy to hear from you whether it’s with feedback on our information, to share your story, or just to find out more about the work of Versus Arthritis. Contact us at [email protected] Words shown are explained in the glossary on p.26. Registered office: Versus Arthritis, Copeman House, St Mary’s Gate, Chesterfield S41 7TD in bold Registered Charity England and Wales No. 207711, Scotland No. SC041156. -
Malignant Olecranon Bursitis in the Setting of Multiple Myeloma Relapse
Case Report Malignant olecranon bursitis in the setting of multiple myeloma relapse Maxwell M Krem, MD, PhD,a Samer Z Al-Quran, MD,b Craig L Silverman, MD,c Vallejo Miller, RN,a and William Tse, MD, FACPa aDivision of Blood and Bone Marrow Transplantation, Department of Medicine, and Departments of bPathology and cRadiation Oncology, at the James Graham Brown Cancer Center, University of Louisville School of Medicine, Louisville, Kentucky ultiple myeloma is the most common Case presentation and summary plasma cell neoplasm, with an esti- A 46-year-old man with a longstanding history mated 24,000 cases occurring annu- of multiple myeloma developed swelling of the Mally. 1 Symptomatic multiple myeloma most com- left elbow that was initially painless in September monly presents with one or more of the cardinal 2016. He had been diagnosed with IgA kappa mul- CRAB phenomena of hypercalcemia, renal dys- tiple myeloma and AL deposition in 2011. Over the function, anemia, or lytic bone lesions.2 Less com- course of his disease, he was treated with the follow- monly, patients may present with plasmacytomas ing sequence of therapies: cyclophosphamide, bort- (focal lesions of malignant plasma cells), which may ezomib, and dexamethasone, followed by melphalan- involve bony or soft tissues.1 conditioned autologous peripheral blood stem cell Plasma cell neoplasms occasionally involve the joints, transplant; lenalidomide and dexamethasone; car lzo- including the elbows, typically as plasmacytomas. e mib and dexamethasone; pomalidomide, bortezomib, elbow is an unusual but reported location of plasma- and dexamethasone; and bortezomib, lenalidomide, cytomas.3,4 A case of multiple myeloma and amyloid dexamethasone, doxorubicin, cyclophosphamide, and light-chain (AL) amyloidosis has been reported, with etoposide, followed by second melphalan-conditioned manifestations including pseudomyopathy, bone mar- autologous peripheral blood stem cell transplant. -

Olecranon Bursitis As Initial Presentation of Gout in Asymptomatic Normouricemic Patients
CORE Metadata, citation and similar papers at core.ac.uk Provided by Elsevier - Publisher Connector The Egyptian Rheumatologist (2014) 36, 47–50 Egyptian Society for Joint Diseases and Arthritis The Egyptian Rheumatologist www.rheumatology.eg.net www.sciencedirect.com CASE REPORT Olecranon bursitis as initial presentation of gout in asymptomatic normouricemic patients Yasser Emad a,b,*, Yasser Ragab c,d, Nashwa El-Shaarawy e, J.J. Rasker f a Rheumatology and Rehabilitation Department, Faculty of Medicine, Cairo University, Cairo, Egypt b Rheumatology and Rehabilitation Department, Dr. Erfan and Bagedo General Hospital, Jeddah, Saudi Arabia c Radiology Department, Faculty of Medicine, Cairo University, Cairo, Egypt d Radiology Department, Dr. Erfan and Bagedo General Hospital, Jeddah, Saudi Arabia e Rheumatology and Rehabilitation Department, Suez Canal University, Ismailia, Egypt f Rheumatology Department, University of Twente, The Netherlands Received 25 August 2013; accepted 25 August 2013 Available online 4 October 2013 KEYWORDS Abstract Background: Acute bursitis is a less frequent presentation of gout, especially in Olecranon gouty bursitis; normouricemic subjects compared to the typical pattern of acute gouty arthritis. Olecranon bursitis; Aim of the work: The aim of the current case reports is to describe the clinical and the magnetic Gout; resonance imaging features of acute gouty olecranon bursitis as initial presentation of acute gouty MRI features attack. Case report: In this report we describe the clinical and MRI features of three cases presenting with acute gouty olecranon bursitis, in spite of normal serum uric acid and stable renal function. For all cases diagnostic aspiration was carried out to exclude septic bursitis as initial first step of management. -

10 Soft Tissue Injections
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Repositório Institucional dos Hospitais da Universidade de... Best Practice & Research Clinical Rheumatology Vol. 19, No. 3, pp. 503–527, 2005 doi:10.1016/j.berh.2005.01.003 available online at http://www.sciencedirect.com 10 Soft tissue injections Luı´s P.B.S. Ineˆs MD Rheumatologist Jose´ Anto´nio P. da Silva* MD, PhD Consultant Rheumatologist and Professor of Rheumatology Hospitais da Universidade de Coimbra, 3000-075 Coimbra, Portugal Soft tissue rheumatism includes a wide spectrum of common lesions of the tendons, enthesis, tendon sheaths, bursae, ligaments and fasciae as well as nerve compression syndromes. Studies on the pathogenesis of these lesions do not support a major role for inflammation, thus questioning the rationale for glucocorticoid injections. This chapter reviews current indications for local glucocorticoid injections and available evidence on its efficacy, as well as contra- indications and potential risks. Randomised controlled studies of good methodological quality are rare and there is limited scientific evidence to support the superiority of glucocorticoid injections over alternative treatments. The basic principles of the glucocorticoid injection method are outlined, together with a description of the practical procedure for the more common conditions. Key words: soft tissue rheumatism; treatment; glucocorticoid injection. Periarticular soft tissue rheumatic disorders include a wide spectrum of localised lesions of the tendons, enthesis, tendon sheaths, bursae, ligaments and fasciae as well as nerve compression syndromes. They are extremely common in daily practice and result in significant morbidity and socioeconomic impact. These aspects, together with their tendency to chronicity and recurrence, make the treatment of these conditions an important health care issue. -
Olecranon Bursitis
Physician’s Notes Date: Olecranon Bursitis Mission Statement The mission of ASSH is to advance the science and practice of hand surgery through education, research and advocacy on behalf of patients and practitioners. 6300 North River Road Suite 600 Rosemont, IL 60018-4256 Phone: (847) 384-8300 Fax: (847) 384-1435 E-mail: [email protected] www.handcare.org Diagram for Physician’s use www.handcare.org What is olecranon bursitis? Figure 1. Elbow anatomy with swollen olecranon bursa What are the treatments The olecranon (oh-LEH-cruh-nahn) is the “pointy” bone at for olecranon bursitis? the tip of the elbow. A “bursa”—a small sac of fluid—covers Your doctor likely will ask questions to try to determine if you the tip of this bone, allowing soft tissues such as the skin have a systemic disease that might need to be treated in to slide over the bone. Normally, this sac has only a tiny humerus order to treat the olecranon bursitis. Most people do not. amount of fluid inside of it and is essentially flat. However, sometimes, this area gets irritated and the body makes If you do not have pain, your doctor might recommend extra fluid inside the sac (see Figure 1). This can cause a a resting splint and compression to rest the bursa and big “balloon” to form at the tip of the elbow. help speed recovery. Sometimes elbow pads can help, especially if you find that you are one of those people who What causes olecranon bursitis? radius tend to lean on the tip of the elbow a lot. -

Therapeutic Ultrasound
CLINICAL Therapeutic Ultrasound REVIEW Indexing Metadata/Description › Device/equipment: Therapeutic Ultrasound › Synonyms: Ultrasonic therapy; ultrasonic diathermy; ultrasound, therapeutic › Area(s) of specialty: Acute care, hand therapy, neurological rehabilitation, orthopedic rehabilitation, pediatric rehabilitation, sports rehabilitation, women’s health, geriatric rehabilitation › Description/use: A therapeutic modality that uses acoustic energy rather than electromagnetic energy to produce physiological effects.(1,2) It should be differentiated from diagnostic ultrasound, which is used for imaging internal structures • Ultrasound waves have a frequency greater than 20,000 Hz (.02 MHz), which is higher than the audible range of the human ear. The frequency range for therapeutic ultrasound is between 0.75 and 3 MHz(1) • Ultrasound is applied using a transducer, or “soundhead,” that contains a piezoelectric crystal that converts electrical energy to acoustic energy(1) • Thermal and nonthermal physiological effects can be produced by vibrations of the molecules of the biologic medium through which the waves travel(1) • Ultrasound is primarily used for elevating tissue temperature.(1) It is considered a deep heating modality (as compared to other heating modalities such as hot packs or whirlpools) because of its ability to heat to a depth of 5 cm(1) • Depth of tissue penetration is determined by the frequency, not the intensity, of ultrasound. In general, higher frequencies (e.g., 3 MHz) are absorbed more in superficial tissues. Lower