Section 3: Data Definitions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Original Article Comparison of Maternal and Fetal Outcomes of IVF and Spontaneously Conceived Twin Pregnancies: Three Year Experience of a Tertiary Hospital
Int J Clin Exp Med 2015;8(4):6272-6276 www.ijcem.com /ISSN:1940-5901/IJCEM0006677 Original Article Comparison of maternal and fetal outcomes of IVF and spontaneously conceived twin pregnancies: three year experience of a tertiary hospital Ahmet Göçmen1, Şirin Güven2, Simge Bağci1, Yasemin Çekmez1, Fatih Şanlıkan1 1Department of Obstetrics and Gynecology, Ümraniye Medical and Research Hospital, İstanbul, Turkey; 2Depart- ment of Neonatology, Ümraniye Medical and Research Hospital, İstanbul, Turkey Received February 3, 2015; Accepted February 18, 2015; Epub April 15, 2015; Published April 30, 2015 Abstract: Objectives: The aim of this study was to compare maternal and fetal outcomes of spontaneously con- ceived and in-vitro fertilization (IVF) twin pregnancies that were admitted to our obstetric clinic and delivered be- tween January 1, 2011 to November 1, 2014. Material method: A total of 84 twin pregnancies were enrolled for the study and divided into two groups: group 1 as IVF (n = 19) and group 2 as spontaneously conceived (n = 65) twin pregnancies. Data of neonatal various morbidities needs neonatal intensive care unit (NICU) such as necrotizing enterocolitis (NEC), bronchopulmonary dysplasia (BPD), sepsis, retinopathy of prematurity (ROP), and intraventricu- lar hemorrhage (IVH) and maternal morbidities such as preeclampsia, eclampsia, postpartum bleeding, gestational diabetes mellitus(GDM) were collected by hospital records. Results: There were no statistical difference between two groups regarding hypertension related to pregnancy, intrauterine growth retardation, Apgar scores, NICU needs, birth weight and height (P > 0.05). The rate of premature rupture of membranes, maternal age, antenatal anemia and premature birth were detected higher in IVF group when compared with the other group (P < 0.05). -

Prenatal Alcohol Consumption Between Conception and Recognition of Pregnancy
ALCOHOLISM:CLINICAL AND EXPERIMENTAL RESEARCH Vol. 41, No. 2 February 2017 Prenatal Alcohol Consumption Between Conception and Recognition of Pregnancy Clare McCormack, Delyse Hutchinson, Lucy Burns, Judy Wilson, Elizabeth Elliott, Steve Allsop, Jake Najman, Sue Jacobs, Larissa Rossen, Craig Olsson, and Richard Mattick Background: Current estimates of the rates of alcohol-exposed pregnancies may underestimate prenatal alcohol exposure if alcohol consumption in early trimester 1, prior to awareness of pregnancy, is not considered. Extant literature describes predictors of alcohol consumption during pregnancy; how- ever, alcohol consumption prior to awareness of pregnancy is a distinct behavior from consumption after becoming aware of pregnancy and thus may be associated with different predictors. The purpose of this study was therefore to examine prevalence and predictors of alcohol consumption by women prior to awareness of their pregnancy, and trajectories of change to alcohol use following pregnancy recognition. Methods: Pregnant women (n = 1,403) were prospectively recruited from general antenatal clinics of 4 public hospitals in Australian metropolitan areas between 2008 and 2013. Women completed detailed interviews about alcohol use before and after recognition of pregnancy. Results: Most women (n = 850, 60.6%) drank alcohol between conception and pregnancy recogni- tion. Binge and heavy drinking were more prevalent than low-level drinking. The proportion of women who drank alcohol reduced to 18.3% (n = 257) after recognition of pregnancy. Of women who drank alcohol, 70.5% ceased drinking, 18.3% reduced consumption, and 11.1% made no reduction following awareness of pregnancy. Socioeconomic status (SES) was the strongest predictor of alcohol use, with drinkers more likely to be of high rather than low SES compared with abstainers (OR = 3.30, p < 0.001). -

Using Aromatherapy and Hydrotherapy in Obstetrics Care – Study on Labouring Women´S Perceptions
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by UEF Electronic Publications USING AROMATHERAPY AND HYDROTHERAPY IN OBSTETRICS CARE – STUDY ON LABOURING WOMEN´S PERCEPTIONS Blanka Tiainen Master's thesis Public Health School of Medicine Faculty of Health Sciences University of Eastern Finland September 2014 2 UNIVERSITY OF EASTERN FINLAND, Faculty of Health Sciences Public health Tiainen, B.: Using Aromatherapy and Hydrotherapy in Obstetric Care – Study on Labour- ing Women´s Perceptions Master's thesis: 43 pages, 1 attachments (9 pages) Instructors: Sohaib Khan, MBBS, MPH, PhD., Jitka Krouželová, MD., Arja Erkkilä, PhD., Adjunct Professor September 2014 Key words: Hydrotherapy, aromatherapy, labour, pain, complementary and alternative medicine USING AROMATHERAPY AND HYDROTHERAPY IN OBSTETRIC CARE - STUDY ON LABOURING WOMEN´S PERCEPTIONS Complementary and alternative medicines and therapies have already been part of obstetrics for a long time. Nowadays, they are getting more and more popular. In some countries and hospitals complementary and alternative medicine is still widely discussed topic. It would help to launch a thorough research in this field to eliminate the polemic. The general aim of the study is to explore the perceived effectiveness of aromatherapy and/or hydrotherapy during childbirth by women in labour. The specific aims of the study were to describe basic childbirth related characteristics of the participants, explore perceptions of the study participants on aromatherapy and/or hydrotherapy and explore reasons why aromatherapy and/or hydrotherapy were used in child labour. Cross sectional study was carried out in delivery ward of Hospital of Merciful Brothers, Brno, Czech Republic. -

1 the Association Between Gravidity, Parity and the Risk of Developing Rheumatoid Arthritis
THE ASSOCIATION BETWEEN GRAVIDITY, PARITY AND THE RISK OF DEVELOPING RHEUMATOID ARTHRITIS: A SYSTEMATIC REVIEW AND META-ANALYSIS Winnie MY Chen1, Sujith Subesinghe, S1,2, Sara Muller3, Samantha L Hider3,4, Christian D Mallen3, Ian C Scott3,4 Affiliations: 1. Department of Academic Rheumatology, King’s College London, London, UK 2. Guy’s and St Thomas’ NHS Trust, London, UK. 3. Arthritis Research UK Primary Care Centre, Research Institute for Primary Care and Health Sciences, Primary Care Sciences, Keele University, Keele, UK 4. Haywood Academic Rheumatology Centre, Haywood Hospital, Midlands Partnership NHS Foundation Trust, High Lane, Burslem, Staffordshire, UK. Abstract Word Count: 245 words Manuscript Word Count: 3,538 words Corresponding Author: Dr Ian Scott; email: [email protected]; ORCHID ID: 0000-0002-1268-9808. 1 ABSTRACT Objective: to establish if gravidity and parity associate with the development of rheumatoid arthritis (RA), and to establish if this effect is influenced by the time elapsed since pregnancy/childbirth, the number of pregnancies/childbirths, and serological status, through systematically reviewing the literature and undertaking a meta-analysis. Methods: we searched Medline/EMBASE (from 1946-2018) using the terms “rheumatoid arthritis.mp” or “arthritis, rheumatoid/” and “pregnancy.mp” or “pregnancy/” or “parity.mp” or “parity/” or “gravidity.mp” or “gravidity/” (observational study filter applied). Case- control/cohort studies that examined the relationship between parity/gravidity and the risk of RA in women were included. Studies reporting effect size data for RA in ever vs. never parous/gravid women as ORs/RRs with 95% confidence intervals were included in a meta- analysis. -

The Effect of Progesterone Use in the First Trimester on Fetal Nuchal Translucency
Original Investigation 29 The effect of progesterone use in the first trimester on fetal nuchal translucency Müberra Namlı Kalem1, Ziya Kalem2, Batuhan Bakırarar3, Ali Ergün1, Timur Gürgan2 1Clinic of Obstetrics and Gynecology, Liv Hospital, Ankara, Turkey 2Gürgan Clinic IVF and Women Health Center, Ankara, Turkey 3Department of Biostatistic, Ankara University School of Medicine, Ankara, Turkey Abstract Objective: To evaluate the possible association between progesterone use in the first trimester of pregnancy and fetal nuchal translucency (NT). Material and Methods: This is an observational case-control study, which was conducted with patients who underwent nuchal scans between March 2015 and February 2016 and consequently delivered live and healthy babies. The study group was composed of assisted reproductive technology pregnancies and used intravaginal progesterone 180 mg/day until gestational week 12. The control group comprised pregnant women who became pregnant spontaneously without using any progesterone preparation in the first trimester. Results: One hundred sixty-four (57.5%) of 285 patients were in the control group and 121 (42.5%) were in the progesterone group. Age, bodyweight, gravidity, and parity number of previous births and abortus, gestational week, crown-rump lengths, free β-human chorionic gonadotropin, pregnancy-associated plasma protein A, and NT values of the progesterone and control groups were recorded and we investigated whether there was a statistically significant difference between the two groups in terms of these parameters; maternal weight was found to be higher in the progesterone group than in the control group and the difference between the groups was statistically significant (p=0.019 and p=0.025). -

PARITY” Amongst Obstetricians and Midwives in Wales
Interpretation of the word “PARITY” amongst Obstetricians and Midwives in Wales. Bwrdd Iechyd Prifysgol Betsi Cadwaladr Dr. Sujatha Kumari, Speciality Doctor O&G, Wrexham Maelor Hospital University Health Board Mr. Hemant Maraj, Consultant O&G, Wrexham Maelor Hospital AIM Q1 OCCUPATION Answered 143 Skipped 0 To evaluate the interpretation of the term ‘parity’ in clinical practice within Wales. METHOD Midwife Clinician survey and literature review. 55.94% 44.08% Doctor Survey conducted by electronic questionnaire sent to all O&G doctors in Wales and midwives in North Wales. RESULTS Q2 GRADE FOR DOCTORS 143 responses received (63 doctors and 80 midwives). Answered 66 Skipped 77 9.15% defined parity as number of previous pregnancies irrespective of ST1-ST2 19.70% outcome. ST3-ST7 19.70% 61.27% (44.30% midwives, 95.24% doctor) defined as number of previous Speciality 19.70% pregnancies, after 24 completed weeks irrespective of outcome. Doctor 29.58% (49.36% midwives, 4.76% doctors) as number of previous Consultant 19.70% pregnancies ending in live births after 24 completed weeks. 83.92% (95% midwives, 69.85% doctors) described having a previous twin delivery as G2P2. Q3 GRADE FOR MIDWIVES Answered 78 Skipped 65 16.08% (5% midwives, 30.15% doctors) responded G2P1. Band 5 11.54% Band 6 55.13% DISCUSSION Band 7 33.33% Parity is considered during risk assessment for VTE and postpartum haemorrhage or when assessing suitability for midwife lead care. Literature review (medical dictionaries, text books, RCOG enquiry, patient information Q4 Which of the following best leaflet, journals) consistently defined parity as the number of pregnancies explains the word PARITY that attained the gestation of viability irrespective of outcome. -
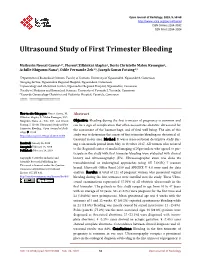
Ultrasound Study of First Trimester Bleeding
Open Journal of Radiology, 2019, 9, 58-68 http://www.scirp.org/journal/ojrad ISSN Online: 2164-3032 ISSN Print: 2164-3024 Ultrasound Study of First Trimester Bleeding Mathurin Neossi Guena1,2*, Florent Zilbinkai Alapha2, Doris Christelle Maleu Kemegne1, Achille Nkigoum Nana3, Odile Fernande Zeh4,5, Joseph Gonsu Fotsing4,5 1Department of Biomedical Sciences, Faculty of Sciences, University of Ngaoundéré, Ngaoundéré, Cameroon 2Imaging Service, Ngaoundéré Regional Hospital, Ngaoundéré, Cameroon 3Gyneacology and Obstetrical Service, Ngaoundéré Regional Hospital, Ngaoundéré, Cameroon 4Faculty of Medicine and Biomedical Sciences, University of Yaounde I, Yaounde, Cameroon 5Yaounde Gynaecology Obstetrics and Pediatrics Hospital, Yaounde, Cameroon How to cite this paper: Neossi Guena, M., Abstract Zilbinkai Alapha, F., Maleu Kemegne, D.C., Nkigoum Nana, A., Zeh, O.F. and Gonsu Objective: Bleeding during the first trimester of pregnancy is common and Fotsing, J. (2019) Ultrasound Study of First can be a sign of complication that often necessitates obstetric ultrasound for Trimester Bleeding. Open Journal of Radi- the assessment of the haemorrhage, and of fetal well being. The aim of this ology, 9, 58-68. https://doi.org/10.4236/ojrad.2019.91006 study was to determine the causes of first trimester bleeding on obstetrical ul- trasound in our area. Method: It was a cross-sectional descriptive study dur- Received: January 16, 2019 ing a six-month period from May to October 2017. All women who referred Accepted: February 25, 2019 to the Regional center of medical imaging of Ngaoundere who agreed to par- Published: February 28, 2019 ticipate in the study with first trimester bleeding were evaluated with clinical Copyright © 2019 by author(s) and history and ultrasonography (US). -

Anatomy and Physiology of Pregnancy 209
208-230_CH08_Lowdermilk.qxd 11/1/05 5:26 PM Page 208 Chapter Anatomy and Physiology8 of Pregnancy DEITRA LEONARD LOWDERMILK LEARNING OBJECTIVES • Determine gravidity and parity by using the five- • Compare normal adult laboratory values with and four-digit systems. values for pregnant women. • Describe the various types of pregnancy tests • Identify the maternal hormones produced during including the timing of tests and interpretation pregnancy, their target organs, and their major of results. effects on pregnancy. • Explain the expected maternal anatomic and • Compare the characteristics of the abdomen, physiologic adaptations to pregnancy for each vulva, and cervix of the nullipara and multipara. body system. • Differentiate among presumptive, probable, and positive signs of pregnancy. KEY TERMS AND DEFINITIONS ballottement Diagnostic technique using palpation: diastasis recti abdominis Separation of the two rec- a floating fetus, when tapped or pushed, moves tus muscles along the median line of the abdom- away and then returns to touch the examiner’s inal wall; often seen in women with repeated child- hand births or with a multiple gestation (e.g., triplets) Braxton Hicks sign Mild, intermittent, painless uter- epulis Tumorlike benign lesion of the gingiva seen ine contractions that occur during pregnancy; oc- in pregnant women cur more frequently as pregnancy advances but do funic souffle Soft, muffled, blowing sound pro- not represent true labor; however, they should be duced by blood rushing through the umbilical ves- distinguished -

A Pilot Cross-Sectional Study of Pregnant Women Attending Prenatal Care in an Urban City Imelda K
Moise BMC Pregnancy and Childbirth (2019) 19:472 https://doi.org/10.1186/s12884-019-2652-5 RESEARCH ARTICLE Open Access Alcohol use, pregnancy and associated risk factors: a pilot cross-sectional study of pregnant women attending prenatal care in an urban city Imelda K. Moise Abstract Background: Alcohol consumption during pregnancy is associated with adverse pregnancy outcomes such as preventable alcohol-related developmental disability fetal alcohol syndrome. In Zambia, alcohol use and associated risk factors have not been investigated, and screening in prenatal care is nonexistent. This study determined individual correlates and the prevalence of alcohol use in pregnant women attending prenatal care at two health clinics in Lusaka, Zambia. Methods: A study adopted a cross-sectional design and recruited 188 pregnant women after seeking their informed consent from July 19 to 31, 2017. Participants aged 18 or over completed the T-ACE (Tolerance, Annoyance, Cut Down and Eye Opener) screening tool and validated alcohol-screening questionnaires on self- reported alcohol use periconceptional and during conception period while at their regular prenatal visit. The T-ACE screening tool assessed the risk of alcohol dependence in four short questions. The questionnaires included demographic questions. Bivariate analyses were performed using the χ2 test for dichotomous variables and the t- test for continuous variables. Mixed-effects linear models were used to evaluate the effect of outcome variables with patient-level variables. Results: About 40 (21.2%) pregnant women were identified by the T-ACE as at-risk for problem drinking during pregnancy. Except for regular prenatal care and distance, there was no difference in the demographic factors between pregnant women who scored < 2 on the T-ACE and those that scored > 2 points (all p’s > 0.05). -

Obstetric and Neonatal Risk of Pregnancies After Assisted Reproductive Technology: a Matched Control Study
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by SZTE Publicatio Repozitórium - SZTE - Repository of Publications Acta Obstet Gynecol Scand 2003: 82: 850--856 Copyright # Acta Obstet Gynecol Scand 2003 Printed in Denmark. All rights reserved Acta Obstetricia et Gynecologica Scandinavica ISSN 0001-6349 ORIGINAL ARTICLE Obstetric and neonatal risk of pregnancies after assisted reproductive technology: a matched control study 1 2 1 3 1 1 ZOLTA´ N KOZINSZKY ,JA´ NOS ZA´ DORI ,HAJNALKA ORVOS ,MA´ RTA KATONA ,ATTILA PA´ L AND LA´ SZLO´ KOVA´ CS From the 1Department of Obstetrics and Gynecology, the 2Center for Assisted Reproduction, Kaa´li Institute, and the 3Department of Pediatrics, University of Szeged, Albert Szent-Gyo¨rgyi Medical and Pharmacological Center, Szeged, Hungary Acta Obstet Gynecol Scand 2003; 82: 850–856. # Acta Obstet Gynecol Scand 82 2003 Background. The aim of the study was to evaluate the obstetric and neonatal outcome of pregnancies after assisted reproduction technology (ART) in comparison with matched controls from spontaneous pregnancies. Methods. A total of 12 920 deliveries at the Department of Obstetrics and Gynecology, University of Szeged, from 1 January 1995 to 31 December 2001 were subjected to retro- spective analysis. Two hundred and eighty-four singleton, 75 twin and 17 triplet pregnan- cies after ovulation induction (n ¼ 114; 30.3%), intrauterine insemination (n ¼ 33; 8.8%) and in vitro fertilization (n ¼ 229; 60.9%) were evaluated. The pregnancy outcome of the singleton and twin pregnancies was compared with that for controls matched with regard to age, gravidity and parity and previous obstetric outcome after spontaneous pregnan- cies. -
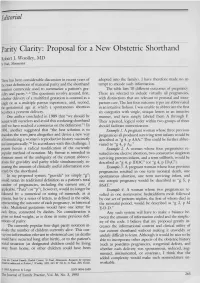
Parity Clarity: Proposal for a New Obstetric Shorthand
Editorial Parity Clarity: Proposal for a New Obstetric Shorthand Robert J. Woolley, MD 51 Paul, M innesota There has been considerable discussion in recent years of adopted into the family). I have therefore made no at the exact definitions of maternal parity and the shorthand tempt to encode such information. notation commonly used to summarize a patient’s gra The table lists 10 different outcomes of pregnancy. vidity and parity.1-6 The questions revolve around, first, These are selected to include virtually all pregnancies, whether delivery of a multifetal gestation is counted as a with distinctions that are relevant to prenatal and intra single or as a multiple parous experience, and, second, partum care. The last four outcome types arc abbreviated the gestational age at which a spontaneous abortion in an intuitive fashion. I was unable to abbreviate the first becomes a preterm delivery. six categories with single, unique letters in an intuitive One author concluded in 1989 that “we should be manner, and have simply labeled them A through F. honest with ourselves and avoid this confusing shorthand Their repeated, logical order within two groups of three until we have reached a consensus on the definition.”1 In should facilitate memorization. 1991, another suggested that “the best solution is to Example 1. A pregnant woman whose three previous abandon the term para altogether and devise a new way pregnancies all produced surviving term infants would be of formulating a woman’s reproductive history succinctly described as “g 4, p AAA.” This could be further abbre and unequivocally.”6 In accordance with this challenge, I viated to “g 4, p A3.” present herein a radical modification of the currently Example 2. -

Donor Age Is Paramount to Success in Oocyte Donation*
Human Reproduction vol.14 no.11 pp. 2755–2758, 1999 Donor age is paramount to success in oocyte donation* Matthew A.Cohen, Steven R.Lindheim and who do not use their own eggs. Of great interest to recipient Mark V.Sauer1 couples are the personal characteristics of their egg donor. To date, there are only a few conflicting studies addressing whether Department of Obstetrics and Gynecology, Division of Reproductive Endocrinology, New York Presbyterian Medical donor age and prior donor fertility significantly influence Center, College of Physicians and Surgeons, Columbia University, pregnancy success. Furthermore, it has been suggested that New York, USA increasing age in oocyte donors decreases the chances of 1To whom correspondence should be addressed at: Columbia recipient success (Rotsztejn and Asch, 1991; Balmaceda et al., Presbyterian Medical Center, Department of Obstetrics and 1994; Faber et al., 1997). Others describe no effect (Abdalla Gynecology, 622 West 168th Street, New York, NY 10032, USA et al., 1993; Wong et al., 1996; Stolwijk et al., 1997). Published Several reports suggest increasing age in oocyte donors data concerning donor gravidity (Darder et al., 1996; Faber decreases the chances of in-vitro fertilization (IVF) success, et al., 1997) and parity (Abdalla et al., 1990; Rotsztejn et al., while others describe no effect. The published data 1992) are similarly difficult to interpret. concerning gravidity and parity are similarly conflicting. We chose to address these questions using a large database To further address these questions, we retrospectively to ascertain which variables (donor age, gravidity, parity, or the studied 445 consecutive donor IVF cycles at two large number of oocytes retrieved), if any, are important predictors of university-based IVF practices.