EXPERT REPORT of ERIC RIGNOT, Ph.D
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Savor the Cryosphere
Savor the Cryosphere Patrick A. Burkhart, Dept. of Geography, Geology, and the Environment, Slippery Rock University, Slippery Rock, Pennsylvania 16057, USA; Richard B. Alley, Dept. of Geosciences, Pennsylvania State University, University Park, Pennsylvania 16802, USA; Lonnie G. Thompson, School of Earth Sciences, Byrd Polar and Climate Research Center, Ohio State University, Columbus, Ohio 43210, USA; James D. Balog, Earth Vision Institute/Extreme Ice Survey, 2334 Broadway Street, Suite D, Boulder, Colorado 80304, USA; Paul E. Baldauf, Dept. of Marine and Environmental Sciences, Nova Southeastern University, 3301 College Ave., Fort Lauderdale, Florida 33314, USA; and Gregory S. Baker, Dept. of Geology, University of Kansas, 1475 Jayhawk Blvd., Lawrence, Kansas 66045, USA ABSTRACT Cryosphere,” a Pardee Keynote Symposium loss of ice will pass to the future. The This article provides concise documen- at the 2015 Annual Meeting in Baltimore, extent of ice can be measured by satellites tation of the ongoing retreat of glaciers, Maryland, USA, for which the GSA or by ground-based glaciology. While we along with the implications that the ice loss recorded supporting interviews and a provide a brief assessment of the first presents, as well as suggestions for geosci- webinar. method, our focus on the latter is key to ence educators to better convey this story informing broad audiences of non-special- INTRODUCTION to both students and citizens. We present ists. The cornerstone of our approach is the the retreat of glaciers—the loss of ice—as The cryosphere is the portion of Earth use of repeat photography so that the scale emblematic of the recent, rapid contraction that is frozen, which includes glacial and and rate of retreat are vividly depicted. -

Future Iceberg Discharge from Columbia Glacier, Alaska
W.T. Pfeffer Geophysical Consultants, LLC 4 December 2012 Report to Prince William Sound Citizen’s Regional Advisory Council: Future Iceberg Discharge from Columbia Glacier, Alaska Reference PWSRCAC Project #8551 Contractor: W. T. Pfeffer Geophysical Consultants, Nederland, Colorado Report #1 Part I: Data Report 1. Overview Columbia Glacier has the world’s longest and most detailed observational record of an ocean-terminating glacier in rapid retreat. The complexity and volume of data requires that its organization and archiving be managed with care. This report provides a compact overview of the available information, from raw data and imagery to maps, technical reports, and papers published in the scientific literature. The data is organized geographically, with observations of the sea floor and glacial bed followed by observations at the glacier surface and meteorological observations of the local atmosphere. Within each geographic section, observations are categorized by type or source (e.g. ship-borne sonar, aerial photography, ground- based time-lapse camera), and wherever possible, a citation or hyperlink to the data is provided. Finally, certain ancillary data, such as geodetic datum adjustments and photogrammetric control, are listed. A full discussion of the scientific literature on the Columbia Glacier is beyond the scope of this summary. However, a compact bibliography is included, and references are cited whenever necessary to explain the origin of a listed data quantity. History: Credit for the initiation of the Columbia Glacier data record goes to the U.S. Geological Survey (USGS), in particular the efforts of Mark Meier and Austin Post, who anticipated as early as the mid-1960s that Columbia Glacier was likely to begin a rapid retreat. -

On the Craft of Fiction—EL Doctorow at 80
Interview Focus Interview VOLUME 29 | NUMBER 1 | FALL 2012 | $10.00 Deriving from the German weben—to weave—weber translates into the literal and figurative “weaver” of textiles and texts. Weber (the word is the same in singular and plural) are the artisans of textures and discourse, the artists of the beautiful fabricating the warp and weft of language into everchanging pattterns. Weber, the journal, understands itself as a tapestry of verbal and visual texts, a weave made from the threads of words and images. This issue of Weber - The Contemporary West spotlights three long-standing themes (and forms) of interest to many of our readers: fiction, water, and poetry. If our interviews, texts, and artwork, as always, speak for themselves, the observations below might serve as an appropriate opener for some of the deeper resonances that bind these contributions. THE NOVEL We live in a world ruled by fictions of every kind -- mass merchandising, advertising, politics conducted as a branch of advertising, the instant translation of science and technology into popular imagery, the increasing blurring and intermingling of identities within the realm of consumer goods, the preempting of any free or original imaginative response to experience by the television screen. We live inside an enormous novel. For the writer in particular it is less and less necessary for him to invent the fictional content of his novel. The fiction is already there. The writer’s task is to invent the reality. --- J. G. Ballard WATER Anything else you’re interested in is not going to happen if you can’t breathe the air and drink the water. -

Extreme Ice Press Release
Contact: Renee Mailhiot, [email protected], 773-947-3133 Amy Patti, [email protected], 773-947-6005 EXTREME ICE OPENS AT MUSEUM OF SCIENCE AND INDUSTRY, CHICAGO New temporary exhibit showcases effects of climate change through stunning footage CHICAGO, Ill. (March 23, 2017)—The Museum of Science and Industry, Chicago (MSI) will open Extreme Ice, a new temporary exhibit illustrating the immediacy of climate change and how it is altering our world, on March 23, 2017. American photographer James Balog captured thought-provoking images over a multi-year period that showcase the dramatic extent of melting glaciers around the world. Through stunning photographic documentation and time-lapse videography of these glaciers, Extreme Ice provides guests an emotionally visual representation of climate change. This exhibit encourages and educates guests on how they can make a difference in their daily lives. Balog is the founder and director of the Earth Vision Institute and Extreme Ice Survey (EIS), the most wide-ranging, ground-based, photographic study of glaciers. Extreme Ice features the EIS team’s global documentation of glacier melt—alongside other hands-on interactive and informative elements—to illustrate what is happening around the world at a rapid rate. “MSI has a responsibility to our guests, schools and communities to showcase exhibits that present complex scientific concepts in an accessible way,” said Dr. Patricia Ward, director of science and technology at MSI. “Extreme Ice showcases James Balog’s beautifully powerful photography to illustrate the real and alarming speed at which glaciers are melting around the world. The exhibit presents a unique and emotional way to educate guests about climate change.” Nearly 200,000 known glaciers have been mapped and catalogued around the world, according to an international team from the University of Colorado Boulder and Trent University in Ontario, Canada. -

Climate Change and Transmedia Storytelling’
COM Witnessing glaciers melt: climate change and transmedia J storytelling Anita Lam and Matthew Tegelberg Abstract The Extreme Ice Survey (EIS) is an exemplary case for examining how to effectively communicate scientific knowledge about climate change to the general public. Using textual and semiotic analysis, this article analyzes how EIS uses photography to produce demonstrative evidence of glacial retreat which, in turn, anchors a transmedia narrative about climate change. As both scientific and visual evidence, photographs have forensic value because they work within a process and narrative of witnessing. Therefore, we argue that the combination of photographic evidence with transmedia storytelling offers an effective approach for future scientific and environmental communication. Keywords Representations of science and technology; Science communication: theory and models; Visual communication DOI https://doi.org/10.22323/2.18020205 Submitted: 3rd October 2018 Accepted: 4th February 2019 Published: 4th March 2019 Introduction In 2005 and 2006, James Balog embarked on two photographic expeditions for National Geographic to record the rapid recession of the Sólheimajökull Glacier in southern Iceland [Appenzeller, 2007]. What Balog saw on these expeditions was a revelation that would become the source of a continuing obsession. Initially a climate change skeptic, it was seeing and photographing the “dying terminus” of these glaciers that Balog credits with converting him into a believer in climate change. As he explains, “[it] has been a revelation for me, to realize I’m in the midst of monumental geologic change that’s going to change the face of the Earth forever, and I’ve got this tool, this camera, with which to witness the change and to bring the story back” [Ritchin, 2010, p. -
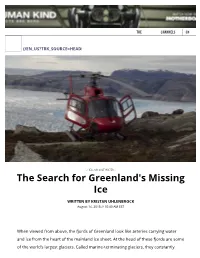
The Search for Greenland's Missing Ice
THE CHANNELS EN (/EN_US?TRK_SOURCE=HEADER-LOGO) - HELL OR SALT WATER - The Search for Greenland's Missing Ice WRITTEN BY KRISTAN UHLENBROCK August 14, 2015 // 10:40 AM EST When viewed from above, the fjords of Greenland look like arteries carrying water and ice from the heart of the mainland ice sheet. At the head of these fjords are some of the world’s largest glaciers. Called marine-terminating glaciers, they constantly recede and advance with the change of the seasons. And every so often, a piece of ice breaks off. The pieces are never trivial. Imagine a chunk of ice miles across and as tall as a skyscraper, most of it submerged below the water’s surface. The ice crumbles into the ocean, rolling and bobbing around like a rubber duck in a bathtub, and slowly floats out to sea. Ice that used to be part of the glacier now drifts around the ocean as large free-floating icebergs, steadily melting. Occasionally, one of these calving events gets caught on film (https://www.youtube.com/watch?v=hC3VTgIPoGU). For a long time scientists focused on warming air temperatures as one of the leading causes of the melting (http://earthobservatory.nasa.gov/Features/PolarIce/polar_ice2.php) of the Greenland ice sheet. Now, researchers have turned their attention to where the ocean and ice meet, typically at the head of fjords that contain these marine-terminating glaciers. By collecting more samples plus using new tools, researchers are shining a light on the complicated underwater picture of how warming Atlantic Ocean waters speed up the melting of the ice, which contributes to sea-level rise. -

Archivist of Ice Earth’S Climate Is Changing
COMMENT BOOKS & ARTS J. BALOG/EXTREME ICE SURVEY J. BALOG/EXTREME James Balog has developed new photographic equipment to monitor changes in glaciers such as the Ilulissat in Greenland. Mountains and at Mount Everest. Shoot- ing every half-hour of daylight year-round, Q&A James Balog each one generates 8,500 frames per year. The footage provides scientists with infor- mation on the mechanics of glacial melting and gives the public evidence of how rapidly Archivist of ice Earth’s climate is changing. For six years, photographer James Balog has trained his lens on ice, capturing time-lapse images that have helped scientists to study how glaciers and ice sheets respond to climate What is the most dramatic moment conditions. With the documentary Chasing Ice soon to debut in US cinemas, Balog talks you’ve caught? about the loss of landscapes. Every year there are calving events in which ice falls off glaciers into the sea. The rate of ice loss in Greenland has doubled during Why are you Portraits of Vanishing Glaciers the past 20 years, and this summer we’ve interested in Rizzoli International: 2012. 288 pp. £29.95 seen unprecedented rates of surface melt- frozen landscapes? ing. We expected the Ilulissat Glacier on the Chasing Ice When I was six years Jeff Orlowski: 2012 west coast of Greenland to have a massive old, I had to walk discharge of ice, so in summer 2008 two of home from school in cover story, ‘The big thaw’, in 2006. The my team members stood watch for weeks. a heavy snowstorm. -

Lesson 5: Ice in Action
Everest Education Expedition Curriculum Lesson 5: Ice in Action Created by Montana State University Extended University and Montana NSF EPSCoR http://www.montana.edu/everest Lesson Overview: Explore glaciers and how they have shaped landscapes around them. Watch glaciers in Montana and those near Mount Everest change over several years through photographs and time-lapse images. Identify parts of a glacier and compare the d3ecline of Himalayan and American glaciers. See how Mount Everest has been shaped by ice in action in the past and how the possible absence of glaciers in the future could change this mountain and those living in its shadows forever. Objectives: Students will be able to: 1. Explain what a glacier is and how glacial movement affects the surrounding landscape. 2. Compare and analyze photographs of Himalayan and Rocky Mountain glaciers to evaluate melting and recession. 3. Explain factors that contribute to glacial ice melt. Vocabulary: albedo (al-BEE-do) - the amount of light reflected by an object alpine (valley) glacier - a glacier confined to a mountain valley climate change - a significant change in the Earth’s climate including temperature, precipitation and wind, as recorded over an extended period of time. continental glacier - very large glaciers that hide the topography underneath them (also called ice sheets) crevasse (kruh-VAS) - a crack in the glacier’s surface that can be very deep and covered by snow glacier - a massive river of ice that moves slowly downward from the high mountains Background Information: Glaciers are large masses of ice that form from the accumulation of snowfall over a long period of time. -

Our Speaker By/With Dr. Joshua Willis Instruments
The Ocean In A Warming Climate Workshop, March 21, 2009 Website Resources OUR SPEAKER Dr. Joshua Willis http://science.jpl.nasa.gov/people/Willis/ “Willis honored for climate change publicity” (October 2008) http://sealevel.jpl.nasa.gov/newsroom/features/200810-2.html BY/WITH DR. JOSHUA WILLIS Jet Propulsion Laboratory podcasts (June 2008) “Tall Oceans and Global Warming” http://www.jpl.nasa.gov/podcast/ostm20080617.cfm From National Public Radio (NPR) “The Mystery of Global Warming’s Missing Heat” http://www.npr.org/templates/story/story.php?storyId=88520025 From EarthSky: A Clear Voice for Science “Josh Willis on oceans and Earth’s energy balance” An interview with Dr. Josh Willis (~8 minutes) http://www.earthsky.org/clear-voices/52704/josh-willis-on-earths-energy-balance INSTRUMENTS & MISSIONS ECCO: Estimating the Circulation and Climate of the Ocean Using data gathered from multiple sources, satellites and in situ measurements (as from Argo floats), this project aims to produce a three-dimensional global state of the ocean. http://science.jpl.nasa.gov/projects/ECCO/ Argo: A global array of 3,000 free-drifting floats that measure the temperature and salinity of the upper 2000m of the ocean. http://www.argo.ucsd.edu/ CLIMATE CHANGE Intergovernmental Panel on Climate Change http://www.ipcc.ch/ NASA’s Global Climate Change website http://climate.jpl.nasa.gov US News & World Report “An Atlas of Climate Change” (July 2008) http://www.usnews.com/articles/science/environment/2008/07/25/an-atlas-of-climate- change.html JPL’s Climate Time Machine This series of visualizations show how some of the key indicators of climate change, such as 1 The Ocean In A Warming Climate Workshop, March 21, 2009 Website Resources temperature, sea ice extent and carbon dioxide concentrations, have changed in Earth’s recent history. -

Research Gear and Equipment Photo Monitoring/Repeat Photography (Includes Montana Case Study)
Everest Education Expedition Curriculum Classroom Activity: Research Gear and Equipment Photo Monitoring/Repeat Photography (includes Montana Case Study) Created by Montana State University Extended University and Montana NSF EPSCoR with support from Scott Powell at Montana State University www.montana.edu/everest Note: This activity requires your classroom to purchase or borrow a standard digital camera or a timeplapse camera such as the TimeLapseCam by Wingscapes http://www.wingscapes.com/timelapse-cameras/timelapsecam8 Overview of the activity: Students will use a digital camera to conduct a photo-monitoring project of approximately three months in duration. Each school day (or every day, if possible) students will take one photograph of the same natural object or scene from the exact same position. Over time, the photographs will reveal change that may not be obvious from day today. Photo monitoring / repeat photography is widely used by researchers who study rangelands, glaciers, forests and other natural areas that change over time. This tactic is also widely used in "citizen science," in which individuals or groups of volunteers help scientists and researchers by contributing their own data and observations. Equipment needed: • Digital camera plus needed accessories (e.g., batteries, memory card cord for connecting to computer, etc.) or a timelapse camera such as that sold by Wingscapes (http://www.wingscapes.com) • tripod (optional) Background information: At locations throughout the Himalaya and around the world, digital cameras have been stationed in order to record the impacts of climate change. As part of the Extreme Ice Survey project, these visuals are then transformed into time-lapse videos that condense the movement and demonstrate how glaciers change over time. -

God's Creation Cries for Justice. Climate
God’s Creation Cries for Justice. Climate Change: Impacts and Faithful Response Participant Packet A Collaboration between JustFaith Ministries and The Catholic Coalition on Climate Change JustMatters is a program of JustFaith Ministries P.O. Box 221348 Louisville, KY 40252 502-429-0865 www.justfaith.org God’s Creation Cries for Justice. Climate Change: Impacts and Faithful Response Participants Packet This document is intended as a resource for leaders planning a JustMatters module. Please read this document in its entirety. All materials are copyrighted and JustFaith is trademarked; however, this document may be copied and forwarded to registered participants in its entirety without permission. JustFaith Ministries works in cooperation with the organizations listed and receives over half of its funding in the form of charitable contributions from program graduates. Catholic Coalition on Climate Change JustFaith Ministries Box 60205 Box 221348 Washington, DC 20039 Louisville, KY 40253 (301) 920-1442 (502) 429-0865 Email: [email protected] www.justfaith.org 2 This document is intended for use by groups who have registered for God’s Creation Cries for Justice during the 2012-2013 program cycle. All materials are copyrighted ©2012. Do not copy, share, forward, or reuse without express permission. Please refer questions and requests to JustFaith Ministries so that we may assist you. JustFaith Ministries | 502-429-0865 | www.justfaith.org The Catholic Coalition on Climate Change P.O. Box 60205 Washington, DC 20039 301-920-1442 www.catholicclimatecovenant.org [email protected] Dear Participant: Catholic Coalition on Welcome to the newly revised 3rd edition of God’s Creation Cries for Justice: Climate Change Climate Change Impacts & Faithful Response! United States Conference of Catholic Bishops: Thank you for your interest in the moral questions and faith commitments related to our changing climate. -
Drops of Knowledge for Rivers of Change
GLOBAL VERSION GLOBAL DROPS OF KNOWLEDGE FOR RIVERS OF CHANGE GLOBAL TEACHING AND LEARNING MATERIAL A hands-on guide to teaching and learning about water, sanitation, hygiene, and the environment ACKNOWLEDGMENTS Swarovski Waterschool Drops of Knowledge for Rivers of Change teaching and learning material was prepared for D. Swarovski KG by the Swarovski Waterschool International Team led by Donna Goodman, Clemens Scheiber, and Bruno Maia. WITH SPECIAL THANKS TO SWAROVSKI WATERSCHOOL LEADERS WORLDWIDE: Burak Cakmak, Ulrike Braun, Matthew Rusk, Anja Riedmann, Birgit Wirnsberger (NPHT, Austria), Yunhua Liu (SISC, China), Charity Bwiza (AWEC, Uganda), Suresh Babu (WWF, India), Swamini Adityananda Saraswati (IHRF, India), Arati Patel (ECI, USA), and Raquel Luna (FAS, Brazil). Swarovski Waterschool gratefully acknowledges the contribution of the Swarovski family and employees worldwide as well as country teams that have led the development of the national- specific editions of this manual. Art Direction & Design: Swarovski, Corporate Creative Services (CCS) Editor: Catherine Rutgers © 2017 SWAROVSKI WATERSCHOOL Swarovski began making crystal 120 years ago, in a valley high in the Austrian alps. One thing convinced my great-great grandfather to set up his new business here – the abundance of water. Water not only offered the clean sustainable energy of hydro-electricity, it was essential for the technique he had invented to cut and polish crystal. The rivers that flowed from the mountains provided an inexhaustible supply. Today Swarovski is one of the most recognised brands in the world, and our headquarters is still in the same valley. Water continues to be fundamental to our company, and more than ever we understand its place as the source of all life on the planet.