Prevalence and Associated Risk Factors of Soil
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Biology and Management of Fish Stocks in Bahir Dar Gulf, Lake Tana, Ethiopia
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Wageningen University & Research Publications Biology and management of fish stocks in Bahir Dar Gulf, Lake Tana, Ethiopia Tesfaye Wudneh Promotor: dr. E.A. Huisman, Hoogleraar in de Visteelt en Visserij Co-promotor: dr. ir. M.A.M. Machiels Universitair docent bij leerstoelgroep Visteelt en Visserij Biology and management of fish stocks in Bahir Dar Gulf, Lake Tana, Ethiopia Tesfaye Wudneh Proefschrift ter verkrijging van de graad van doctor op gezag van de rector magnificus van de Landbouwuniversiteit Wageningen, dr. C.M. Karssen, in het openbaar te verdedigen op maandag 22 juni 1998 des namiddags te half twee in de Aula van de Landbouwuniversiteit te Wageningen. Cover : Traditional fishing with reed boat and a motorised fishing boat (back-cover) on Lake Tana. Photo: Courtesy Interchurch Foundation Ethiopia/Eritrea (ISEE), Urk, the Netherlands. Cover design: Wim Valen. Printing: Grafisch Service Centrum Van Gils b.v., Wageningen CIP-DATA KONINKLIJKE BIBLIOTHEEK, DEN HAAG Wudneh, Tesfaye Biology and management of fish stocks in Bahir Dar Gulf, Lake Tana, Ethiopia / Tesfaye Wudneh. - [S.I. : s.n.]. - III. Thesis Landbouwuniversiteit Wageningen. - With ref. - With summary in Dutch. ISBN 90-5485-886-9 Tesfaye Wudneh 1998. Biology and management of fish stocks in Bahir Dar Gulf, Lake Tana, Ethiopia. The biology of the fish stocks of the major species in the Bahir Dar Gulf of Lake Tana, the largest lake in Ethiopia, has been studied based on data collected during August 1990 to September 1993. The distribution, reproduction patterns, growth and mortality dynamics and gillnet selectivity of these stocks are described. -
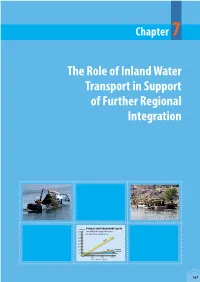
The Role of Inland Water Transport in Support of Further Regional Integration
Chapter 7 The Role of Inland Water Transport in Support of Further Regional Integration unit cost TYPICAL UNIT TRANSPORT COSTS 8,000 For dierent transport means 7,000 as a function of distance 6,000 5,000 truck 4,000 3,000 2,000 rail long-haul container 1,000 ship 0 1,000 2,000 3,000 distance (km) 187 KEY MESSAGES • The land-locked economies of the upper Nile region • Several reaches of the Nile could form elements of are hampered by expensive road transportation a comprehensive bulk cargo transportation system and logistics that have generally reduced their that could provide cost-effective access to internal economic opportunities. and external markets. • Efforts under the African Union and regional • Developing the inland navigation potential of the economic communities have resulted in (especially) river Nile – in particular the ‘southern reach’ from improved road interconnections between the Nile Kosti to Juba – may provide a low-cost transport countries. However, the transport and trade links route for bulk cargo from South Sudan and the Nile between upstream and downstream riparians remain weak. Equatorial Lakes region to The Sudan and Egypt; it could thus encourage north–south intra-basin • The absence of a reliable and cost-effective north– trade and regional integration. south transportation link has constrained trade relations between the upstream and downstream • Lake Victoria could provide a critical link between riparians, and represents a lost opportunity for the Northern Corridor (Kigali–Kampala–Mombasa) regional integration. and the Central Corridor (Dar es Salaam–Tabora– • Economic development in the Nile countries, Mwanza), and enlarge the economic impact zone combined with prospective mineral resources, of the respective corridors; improved Lake Victoria fossil fuels, and agricultural potential, justify navigation would also strengthen inter-regional investment in bulk cargo transport infrastructure. -

Group Organisers Manual
Group Organisers Manual Welcome to McCabe Pilgrimages Alistair McCabe’s involvement in pilgrimage dates back to 1976 when, straight out of university, he was appointed assistant warden of the then Scots Hospice beside the Sea of Galilee: an opportune introduction to pilgrimage and pilgrim parties. This led to managing the Holy Land department of Inter Church Travel working alongside the great pilgrimage innovator, Canon Arthur Payton. When Arthur retired in 1983, the time was right for McCabe Pilgrimages to be born. Rosemary Nutt joined the company shortly afterwards and Alistair and Rosemary are still the heart and soul of the company. We have an excellent team, and our empathy with the needs of pilgrimage organisers is unrivalled. Make an enquiry Let us send you a no obligation suggestion for a pilgrimage from your church. Email or call us and we will send you ideas. Our website has lots of itineraries for you to browse. www.mccabe-travel.co.uk | 020 8675 6828 [email protected] 2 www.mccabe-travel.co.uk 020 8675 6828 Sponsored Walk by the Sea of Galilee 3 A word about health and fitness McCabe website Preparing to Many pilgrims are elderly. Age itself is not You decide whether you would like us to a barrier, but a certain level of fitness is promote your tour through the McCabe required. Think in terms of being able to website. This can be a way of building up lead a pilgrimage walk unaided for at least thirty minutes on numbers, but you may prefer to only recruit uneven ground. -

Daniel Asmare the MELTING POT of the WORD and the SWORD
Daniel Asmare THE MELTING POT OF THE WORD AND THE SWORD: ROYAL POWER AND MONASTIC ASCETICISM IN THE MEDIEVAL MONASTERIES OF LAKE TANA, ETHIOPIA MA Thesis in Comparative History with the specialization in Interdisciplinary Medieval Studies Central European University CEU eTD Collection Budapest May 2011 THE MELTING POT OF THE WORD AND THE SWORD: ROYAL POWER AND MONASTIC ASCETICISM IN THE MEDIEVAL MONASTERIES OF LAKE TANA, ETHIOPIA by Daniel Asmare (Ethiopia) Thesis submitted to the Department of Medieval Studies, Central European University, Budapest, in partial fulfillment of the requirements of the Master of Arts degree in Comparative History, with the specialization in Interdisciplinary Medieval Studies. Accepted in conformance with the standards of the CEU ____________________________________________________________ Chair, Examination Committee ____________________________________________________________ Thesis Supervisor ____________________________________________________________ Examiner ____________________________________________________________ Examiner CEU eTD Collection Budapest May 2011 THE MELTING POT OF THE WORD AND THE SWORD: ROYAL POWER AND MONASTIC ASCETICISM IN THE MEDIEVAL MONASTERIES OF LAKE TANA, ETHIOPIA by Daniel Asmare (Ethiopia) Thesis submitted to the Department of Medieval Studies, Central European University, Budapest, in partial fulfillment of the requirements of the Master of Arts degree in Comparative History, with the specialization in Interdisciplinary Medieval Studies. Accepted in conformance with the -

Local History of Ethiopia : Raayo
Local History of Ethiopia Raayo - Ryke © Bernhard Lindahl (2005) HFE66 Raayo (Ra'ayo) (mountain) 14°12'/39°00' 2525 m 14/39 [Gz] east of Adwa rab (A) hunger, famine; (Som) 1. narrow place; 2. want, desire JED01 Rab (area & place) c700 m 10/42 [WO Gu] Railway station 25 km inside Ethiopia. raba (O) age grade 24-32 years of the Oromo gada system, regarded as the senior warriors JDJ70 Rabal (area), cf Rabel 09/41 [WO] ?? Rabat ../.. [Yo] In 1982 the TPLF negotiated permission by the Afar to operate a base at Rabat in the isolated Magale area. [Young 1997] rabassa: rabbaas (Som) jump /repeatedly/; rabash (Som) trouble, nuisance JDR10 Rabassa (area) 10/41 [WO] rabbi (O,Som) God HCF65 Rabbi 05°58'/39°48' 1301 m, cf Rebbi .. 05/39 [WO Gz] HEU... Rabea (village) see under Mekele 13/39 [n] HDU54 Rabel 10°27'/39°42' 2390 m, south-east of Were Ilu 10/39 [Gz] HDU63 Rabel (Rabiel) 10°33'/39°36' 2965 m 10/39 [Gz Ad] south-east of Were Ilu (centre in 1964 of Gishe wereda) /this Rabel?:/ The first airdrop of relief food was carried out on 13 February 1985 near Rabel, a village situated on a high plateau about 250 km north-east of Addis Abeba. "RRC agreed to the airdrop and gradually became a strong supporter of the operation which utilised a new airdropping technique developed in the United States. The grain was rebagged into double or triple sacks containing 25 kg each and placed on wooden pallets which were dropped from a height of 6 to 10 metres above the ground. -

Local History of Ethiopia : Acab Saat
Local History of Ethiopia Acab Saat - Adgura © Bernhard Lindahl (2005) HFE50 Acab Saat, see Akab Saat JFB33 Acacale, see Akakale HDA83 Acachil, see Akakil JDJ63 Acad, see Akad GDF10 Acado, see Akado HEC14 Acaita, see Akayta JED12 Acalei, see Akaley HEK64 Acam, see Akam & HEK66 GDU20 Acamscia, see Akamsha HEJ68 Acara Mariam, see Akara Maryam ?? Accabo, see Akabo HEK17 Accana Gheorghis, see Ackana Giyorgis HCP43 Accevo, see Achevo HED99 Acchera, see Ackera HCN69c Acchiscio, see Akisho HEC67 Acciader, see Achader HCK93 Acciura, see Ashura HCR95 Acco, see Acko JCN05 Accuba, see Ackuba HDD29 Aceber, see Acheber HEB98 Acefer, see Achefer ?? Acel ../.. [Pa x] Described by Alvares in the 1520s as a Muslim settlement situated southwards in Wello. Christians and "Moors" lived apart, but many Christian women went to the Muslim town to carry water and wash clothes for its inhabitants. The place was visited by traders from as far away as Tunis. There was considerable trade in slaves. [Pankhurst (1990)1992 p 56, 65] As visited by the Portuguese party in September 1520 it might have been near modern Dessie or somewhere in Amba Sel. GCU30 Acer, see Acher HCU90 Achaba (Ach'aba) 08°08'/39°21' 2005 m 08/39 [MS] near map code HDF00 HEC67 Achader (Acciader) 20 km SE of Bahir Dar 11/37 [+ Gu] HEC77 Achader Maryam (Acciader Mariam) 11/37 [+ It] (village with church) HCM01 Achafa (Aciafa) (area) 06/39 [+ WO] HET79 Achalako (Ach'alak'o, Ascialaco) 13/39 [Gz WO Gu] 13°18'/39°11' 2107 m (with church Kidane Mihret) Coordinates would give map code HET78 HDJ68 Achane (Ach'ane, Asciani) 09°39'/37°20' 09/37 [Gz WO] HDJ68 Achane Maryam (Achene Mariam) 09/37 [LM x WO] (with church) 2434 m 1970s An elementary school built of concrete elements and with Swedish assistance through ESBU was completed around 1970. -

Lake Tana, Ethiopia
water Article Water Balance for a Tropical Lake in the Volcanic Highlands: Lake Tana, Ethiopia Muluken L. Alemu 1,2, Abeyou W. Worqlul 3 , Fasikaw A. Zimale 1 , Seifu A. Tilahun 1 and Tammo S. Steenhuis 1,4,* 1 Faculty of Civil and Water Resources Engineering, Bahir Dar Institute of Technology, Bahir Dar University, P.O. Box 26 Bahir Dar, Ethiopia; [email protected] (M.L.A.); [email protected] (F.A.Z.); [email protected] (S.A.T.) 2 Ethiopian Construction Works Corporation, P.O. Box 21951/100 Addis Ababa, Ethiopia 3 Texas A&M AgriLife Research, Temple, TX 76502, USA; [email protected] 4 Department of Biological and Environmental Engineering, Cornell University, Ithaca, NY 14853, USA * Correspondence: [email protected]; Tel.: +1-607-255-2489 Received: 3 September 2020; Accepted: 24 September 2020; Published: 30 September 2020 Abstract: Lakes hold most of the freshwater resources in the world. Safeguarding these in a changing environment is a major challenge. The 3000 km2 Lake Tana in the headwaters of the Blue Nile in Ethiopia is one of these lakes. It is situated in a zone destined for rapid development including hydropower and irrigation. Future lake management requires detailed knowledge of the water balance of Lake Tana. Since previous water balances varied greatly this paper takes a fresh look by calculating the inflow and losses of the lake. To improve the accuracy of the amount of precipitation falling on the lake, two new rainfall stations were installed in 2013. The Climate Hazards Group Infrared Precipitation Version two (CHIRPS-v2) dataset was used to extend the data. -

Debre Tabor - Delo Wereda © Bernhard Lindahl (2005)
Local History of Ethiopia Debre Tabor - Delo wereda © Bernhard Lindahl (2005) Debre Tabor, Mount Tabor of the Bible, (figuratively:) the Transfiguration HEK05 Debre Tabor (Debra T., old name Samara) 11/38 [Gz Pa WO Gu] MS: 11°51'/38°05' = HEK06, 2945 m at the gibbi Gz: 11°51'/38°01' = HEK05, 2706 m Distance 666 km from Addis Abeba. Centre in 1964 of Debre Tabor awraja and Farta wereda and Debre Tabor sub-district. Within a radius of 10 km there are at km 7E Hiruy (Waher, Uaher) (village) 2628 m 8E Amija (Amigia) 10SE Meken Kenia (village) 10SE Semana Giyorgis (S. Ghiorghis) (village) 10SE Amejera Abbo (Ameggera Abbo) (village) 2S Fahart (area) 7SW Grariya Giyorgis (Graria Georgis) (village) 7SW Amba Maryam (A. Mariam) (with church) 6NW Aringo (village) 2515/2574 m 5N Limado (hill) 5?NE Gafat (historical place, cf under its own name) 8NE Guntur (village) ?NE Samara (former ketema) 2706/2782 m ?? Anchim (Anchem) (battle site) ?? Tala Levasi 2558 m Debre Tabor is situated in an amphitheatre of hills. It bears the name of the nearby mountain, which in early medieval times was called Debre Tabor for its resemblance to Mount Tabor in Palestine. On top of the mountain is the Yesus Church, famous for its wood-carvings. The wall paintings are modern. [Jäger 1965 p 75] 1500s The name is known for the first time from the reign of Lebne Dengel, before 1540. 1700s In the last quarter of the 1700s, a man by the name of Ali Gwangul emerged as a powerful figure. He initiated what came to be known as the Yejju dynasty. -
Stakeholder Analysis of the Chara Chara Weir, Lake Tana
Stakeholder Analysis of the Chara Chara Weir, Lake Tana By Ayalew Gebre, Derese Getachew and M. McCartney A Study Report Submitted to The International Water Management Institute (IWMI) January 2008 Table of Contents EXECUTIVE SUMMARY ................................................................................................ 1 1. INTRODUCTION ............................................................................................... 3 1.1 BACKGROUND....................................................................................................... 3 1.2 METHODS ............................................................................................................. 4 2. DATA PRESENTATION AND ANALYSIS ..................................................... 6 2.1 COMMUNITY GROUPS ........................................................................................... 6 2.1.1 FARMERS .............................................................................................................. 6 2.1.1.1 Significance of Lake Tana ................................................................................ 6 2.1.1.2 Interests............................................................................................................. 6 2.1.1.3 Opinions............................................................................................................ 8 2.1.1.4 Concerns ......................................................................................................... 11 2.1.2 FISHERS ............................................................................................................. -

Ethnobotanical Study of Medicinal Plants Used Against Human Ailments in Gubalafto District, Northern Ethiopia Getnet Chekole
Chekole Journal of Ethnobiology and Ethnomedicine (2017) 13:55 DOI 10.1186/s13002-017-0182-7 RESEARCH Open Access Ethnobotanical study of medicinal plants used against human ailments in Gubalafto District, Northern Ethiopia Getnet Chekole Abstract Background: Traditional medicinal plant species documentation is very crucial in Ethiopia for biodiversity conservation, bioactive chemical extractions and indigenous knowledge retention. Having first observed the inhabitants of Gubalafto District (Northern Ethiopia), the author gathered, recorded, and documented the human traditional medicinal plant species and the associated indigenous knowledge. Methods: The study was conducted from February 2013 to January 2015 and used descriptive field survey design. Eighty-four informants were selected from seven study kebeles (sub-districts) in the District through purposive, snowball, and random sampling techniques. Both quantitative and qualitative data were collected through semi-structured interviews, guided field walks, demonstrations, and focus group discussions with the help of guided questions. Data were organized and analyzed by descriptive statistics with SPSS version 20 and Microsoft Office Excel 2007. Results: A total of 135 medicinal plant species within 120 genera and 64 families were documented. Among the species, Ocimum lamiifolium and Rhamnus prinoides scored the highest informant citations and fidelity level value, respectively. In the study area, Asteraceae with 8.1% and herbs with 50.4% plant species were the most used sources for their medicinal uses. A total of 65 ailments were identified as being treated by traditional medicinal plants, among which stomachache (abdominal health problems) was frequently reported. Solanum incanum was reported for the treatment of many of the reported diseases. The leaf, fresh parts, and crushed forms of the medicinal plants were the most preferred in remedy preparations. -

Ethnobotanical Study of Medicinal Plants Used to Treat Human Diseases in Gura Damole District, Bale Zone, Southeast Ethiopia
ASIAN JOURNAL OF ETHNOBIOLOGY Volume 4, Number 1, May 2021 E-ISSN: 2580-4510 Pages: 42-52 DOI: 10.13057/asianjethnobiol/y040105 Ethnobotanical study of medicinal plants used to treat human diseases in Gura Damole District, Bale Zone, Southeast Ethiopia BEHAILU ASSEFA1, MOA MEGERSA1,♥, TILAHUN TOLOSSA JIMA2 1Department of Biology, School of Natural Science, Maddawalabu University. P.O. Box 247, Robe, Ethiopia. ♥email: [email protected] 2Department of Biology, College of Natural and Computational Sciences, Ambo University. P.O. Box 19, Ambo, Ethiopia Manuscript received: 8 November 2020. Revision accepted: 5 April 2021. Abstract. Assefa B, Megersa M, Jima TT. 2021. Ethnobotanical study of medicinal plants used to treat human diseases in Gura Damole District, Bale Zone, Southeast Ethiopia. Asian J Ethnobiol 4: 42-52. Many countries in the world including Ethiopia use medicinal plants for their primary health care system. Plants have been used as a source of medicine to treat human diseases in Ethiopia. The aim of this study was to document medicinal plants used to treat various human diseases in Gura Damole District of Oromia Regional State, southeast Ethiopia. Ethnobotanical study of medicinal plants was carried out from August 05 to November 06, 2019. A total of 90 informants were selected to collect ethnobotanical information from 6 kebeles. Ethnobotanical data were collected using semi-structured interviews, focus group discussion with informants and field observation. Various ethnobotanical ranking indices were used to analyze the importance of some plant species. A total of 30 medicinal plants belonging to 21 families were identified. These medicinal plants comprised shrubs (36.6%), trees (26.6%), herbs (23.3%) and lianas (13.3%). -
Feasibility Study of Renewable Energy Resources for Electrification of Small Islands
ADDIS ABABA UNIVERSITY ADDIS ABABA INSTITUTE OF TECHNOLOGY Department of Electrical and Computer Engineering Feasibility Study of Renewable Energy Resources for Electrification of Small Islands. A Case Study on Tana Lake Islands A thesis Submitted to Addis Ababa Institute of Technology, School of Graduate Studies, Addis Ababa University In partial Fulfillment of the Requirement for the Degree of MASTER OF SCIENCE IN ELECTRICAL AND COMPUTER ENGINEERING (ELECTRICAL POWER ENGINEERING) By Abiyot Mekonnen Advisor:- Prof –WoledeGiorigs WoldeMariyam ADDIS ABABA UNIVERSITY ADDIS ABABA INSTITUTE OF TECHNOLOGY Department of Electrical and Computer Engineering Feasibility Study of Renewable Energy Resources for Electrifications of Small Islands. A Case Study on TanaLake Islands By Abiyot Mekonnen GSR/3203/03 APPROVAL BY BOARD OF EXAMINERS ______________________________ _________________________________ CHAIRMAN DEPARTMENT OF SIGNATURE GRADUATE COMMITTEE _________________________________ ________________________________ ADVISOR SIGNATURE ________________________________ ________________________________ INTERNAL EXAMINER SIGNATURE ________________________________ _______________________________ EXTERNAL EXAMINER SIGNATURE Declaration I, the undersigned, declare that this thesis is my original work, has not been presented for a degree in this or any other university, and all sources of materials used for the thesis have been acknowledged. All examiners’ comments are incorporated. Name: Abiyot Mekonnen W/Giorgis Signature: ____________ Place: Addis