HIV Vaccine Development: the Importance of Gp120 Variable Loop
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
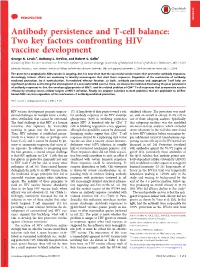
Two Key Factors Confronting HIV Vaccine Development George K
PERSPECTIVE PERSPECTIVE Antibody persistence and T-cell balance: Two key factors confronting HIV vaccine development George K. Lewis1, Anthony L. DeVico, and Robert C. Gallo1 Division of Basic Science and Vaccine Research Institute of Human Virology, University of Maryland School of Medicine, Baltimore, MD 21201 Edited by Anthony S. Fauci, National Institute of Allergy and Infectious Diseases, Bethesda, MD, and approved September 5, 2014 (received for review July 21, 2014) The quest for a prophylactic AIDS vaccine is ongoing, but it is now clear that the successful vaccine must elicit protective antibody responses. Accordingly, intense efforts are underway to identify immunogens that elicit these responses. Regardless of the mechanism of antibody- mediated protection, be it neutralization, Fc-mediated effector function, or both, antibody persistence and appropriate T-cell help are significant problems confronting the development of a successful AIDS vaccine. Here, we discuss the evidence illustrating the poor persistence + of antibody responses to Env, the envelope glycoprotein of HIV-1, and the related problem of CD4 T-cell responses that compromise vaccine efficacy by creating excess cellular targets of HIV-1 infection. Finally, we propose solutions to both problems that are applicable to all Env- based AIDS vaccines regardless of the mechanism of antibody-mediated protection. HIV | vaccine | antibody persistence | AIDS | Tcell HIV vaccine development presents unprece- 17). A large body of data points toward a role exhibited efficacy. The protection was mod- dented challenges on multiple levels, a reality, for antibody responses to the HIV envelope est, with an overall of efficacy 31.2% (21) in often overlooked, that cannot be overstated. -

Phase III HIV Vaccine Trial—Thailand
HIV Vaccine Efficacy Trials; Lessons and Opportunities for Future Research Hannah Kibuuka Makerere University Walter Reed Project, Uganda INTEREST Conference Harare, Zimbabwe Outline . Need for an HIV Vaccine . Efficacy Trials up to date . Lessons from failed Efficacy trials and opportunities for Research . Lessons form RV 144 and P5 follow up studies Before After vaccines vaccines Vaccines work really well! Vaccines are among the most successful medical interventions (eradicated or controlled smallpox, polio, measles…) A Vaccine Is Essential to End AIDS Potential impact of an AIDS vaccine as part of the UNAIDS Enhanced Investment Framework (IFE) Cumulative infections 2.000.000 avoided 2027-70 Current Trend 42.7M Current Trend + Vaccine* 1.500.000 50% Scale-up 27.1M 1.000.000 50% Scale-up + Vaccine* New Infections with HIV HIV with Infections New 500.000 IFE 16.2M IFE + Vaccine* 0 2010 2015 2020 2025 2030 2035 2040 2045 2050 2055 2060 2065 2070 * Illustrative vaccine with an assumed efficacy of 70%, not representative of any specific candidate. Coverage in generalized epidemics: routine 10 years old 70%, catch-up 11-14 years old 60%, 15-17 years old 55%, 18-49 years old 50%; in high risk populations in concentrated epidemics: 50% Modeling project – UNAIDS, Futures Institute, IAVI, AVAC [funded by USAID] 3 Need….. Several new prevention measures have been realized in the last few years. Although efficacious, the interventions are faced with potential challenges of access and adherence . HIV vaccine has potential to address some of these -

Simplified Steps to Heterologous Prime-Boost HIV Vaccine Development?
Simplified steps to heterologous prime-boost HIV vaccine development? Nelson L. Michael J Clin Invest. 2019;129(11):4572-4573. https://doi.org/10.1172/JCI132440. Commentary The RV 144 HIV vaccine efficacy study showed a reduction in HIV-1 infection risk in Thai volunteers who received two priming vaccinations of vCP1521 ALVAC (attenuated recombinant canarypox virus expressing HIV group–specific antigen, polymerase, and envelope genes) followed by two additional ALVAC vaccinations and coadministration of purified bivalent gp120 proteins (AIDSVAX B/E). In this issue of the JCI, Rouphael et al. build on these results by substituting a DNA plasmid cocktail expressing HIV-1 subtype C group–specific antigen, polymerase, and envelope antigen genes (DNA-HIV-PT123) for ALVAC in a phase 1b safety and immunogenicity study. The results indicate that the vaccine regimen is safe, elicits promising cross-subtype humoral and cellular responses, and opens up potentially simplified approaches to HIV-1 vaccine development. Find the latest version: https://jci.me/132440/pdf COMMENTARY The Journal of Clinical Investigation Simplified steps to heterologous prime-boost HIV vaccine development? Nelson L. Michael Center for Infectious Diseases Research, Walter Reed Army Institute of Research, Silver Spring, Maryland, USA. replaced in the current study by a cocktail of three DNA plasmids, DNA-HIV-PT123, The RV 144 HIV vaccine efficacy study showed a reduction in HIV-1 which consists of equal amounts of plas- infection risk in Thai volunteers who received two priming vaccinations of mids expressing HIV-1 subtype C sequenc- vCP1521 ALVAC (attenuated recombinant canarypox virus expressing HIV es: HIV-1 gag, HIV-1 gp140, and group–specific antigen, polymerase, and envelope genes) followed by two ZM96 ZM96 HIV-1CN54 pol-nef, delivered at a total dose additional ALVAC vaccinations and coadministration of purified bivalent of 4 mg administered intramuscularly via gp120 proteins (AIDSVAX B/E). -

For First Time, AIDS Vaccine Shows Some Success
27-10-2009 For First Time, AIDS Vaccine Shows S… This copy is for your personal, noncommercial use only. You can order presentation• ready copies for distribution to your colleagues, clients or customers here or use the "Reprints" tool that appears next to any article. Visit www.nytreprints.com for samples and additional information. Order a reprint of this article now. Septem ber 25 , 2009 For First Time, AIDS Vaccine Shows Some Success By DONA LD G. McNEIL Jr. Scientists said Thursday that a new AIDS vaccine, the first ever declared to protect a significant minority of humans against the disease, would be studied to answer two fundamental questions: why it worked in some people but not in others, and why those infected despite vaccination got no benefit at all. The vaccine — known as RV 144, a combination of two genetically engineered vaccines, neither of which had worked before in humans — was declared a qualified success after a six year clinical trial on more than 16,000 volunteers in Thailand. Those who were vaccinated became infected at a rate nearly one•third lower than the others, the sponsors said Thursday morning. “I don’t w ant to use a w ord like ‘breakthrough,’ but I don’t think there’s any doubt that this is a v e r y im p o r ta n t r e s u lt,” s a id D r . Anthony S. Fauci, the director of the National Institute of Allergy and Infectious Diseases, which is one of the trial’s backers. “F or m ore than 20 years now , vaccine trials have essentially been failures,” Dr. -
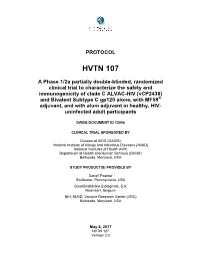
Protocol HVTN 107 Are Described Below
PROTOCOL HVTN 107 A Phase 1/2a partially double-blinded, randomized clinical trial to characterize the safety and immunogenicity of clade C ALVAC-HIV (vCP2438) and Bivalent Subtype C gp120 alone, with MF59® adjuvant, and with alum adjuvant in healthy, HIV- uninfected adult participants DAIDS DOCUMENT ID 12006 CLINICAL TRIAL SPONSORED BY Division of AIDS (DAIDS) National Institute of Allergy and Infectious Diseases (NIAID) National Institutes of Health (NIH) Department of Health and Human Services (DHHS) Bethesda, Maryland, USA STUDY PRODUCT(S) PROVIDED BY Sanofi Pasteur Swiftwater, Pennsylvania, USA GlaxoSmithKline Biologicals, S.A. Rixensart, Belgium NIH, NIAID, Vaccine Research Center (VRC) Bethesda, Maryland, USA May 4, 2017 HVTN 107 Version 3.0 HVTN 107 Version 3.0 / May 4, 2017 Contents 1 Ethical considerations .............................................................................................. 5 2 IRB/EC review considerations ................................................................................. 7 2.1 Minimized risks to participants ..................................................................... 7 2.2 Reasonable risk/benefit balance .................................................................... 8 2.3 Equitable subject selection ............................................................................ 8 2.4 Appropriate informed consent ....................................................................... 8 2.5 Adequate safety monitoring .......................................................................... -
AIDS Vaccines Cannot Cause HIV § No Vaccine Is 100% Effective § Most Vaccines Licensed in the US 70%-95% Effective Why the Interest in an AIDS Vaccine?
Presentation Overview § What is a vaccine? § How would an AIDS vaccine work? § Where are we in the search? § What is needed now? What is a vaccine? § A substance that teaches the immune system how to protect itself against a virus or bacteria § No effective AIDS vaccine available today § AIDS vaccines cannot cause HIV § No vaccine is 100% effective § Most vaccines licensed in the US 70%-95% effective Why the interest in an AIDS vaccine? § Proven prevention options have slowed HIV’s spread but thousands of people continue to get infected daily § There is a need for a range of HIV prevention methods; there is no silver bullet § Vaccines are one of the world’s most effective public health tools § Cost-effective – single or several doses likely provide protection for years How vaccines are crucial to ending AIDS Deliver proven tools for immediate impact • End confusion about “combination • Testing prevention” • Treatment • Narrow gaps in treatment cascade • Voluntary Medical Male Circumcision GOAL: A sustained • Prepare for new non-surgical male • Female and male condoms decline in HIV circumcision devices • Prevention of pediatric infection infections (now at 2.5 million/year) Demonstrate proven tools for immediate impact • Define and initiate the “core • Daily oral TDF/FTC as PrEP package” of PrEP • 1% tenofovir gel demonstration projects Develop long-term solutions to end the epidemic COMBINE • AIDS vaccines • Safeguard HIV Prevention Research Funding • Cure • Multi-purpose prevention technologies • Next generation ARV-based prevention -
Status of HIV Vaccine Development Update on Advanced Projects
Status of HIV vaccine development Update on advanced projects Kundai Chinyenze, MBChB, MPH Medical Director, Medical Affairs, Kenya 2017 WHO Product Development for Vaccines Advisory Committee Consultation 22 June, 2017 Geneva HIV/AIDS Continues to Devastate 2.1 million 78 million infected HALF of all people since discovery in early 1980s living with HIV don’t know they have it 35 million deaths 20 million don’t have since discovery in early 1980s access to treatment Leading killer of women in Many of those who reproductive age do, don’t adhere well 37 million live with 2.1 million new HIV annual HIV infections UNAIDS, 2015 2 Number of New HIV infections globally – all ages Source: http://aidsinfo.unaids.org/ A vaccine could prevent millions of additional HIV infections on top of scale-up of existing interventions Projected reductions of new annual HIV infections (millions) in low- and middle- income countries in years after vaccine introduction “Without an AIDS vaccine we will not end AIDS.” Peter Piot, BMGF Global Health Forum 2015 Modeling – UNAIDS, Avenir Health, IAVI, AVAC [funded by USAID] Illustrative vaccine with an assumed efficacy of 70%, not representative of any specific candidate. Coverage in generalized epidemics: routine 10 years old 70%, catch-up 11-14 years old 60%, 15-17 years old 55%, 18-49 years old 50%; in high risk populations in concentrated epidemics: 50% 4 AIDS Vaccine Development Efficacy Trials: Summary of Past Trials Control of Prevention of HIV Vaccine Candidate HIV Infection Infection 2003 VaxGen : gp120 No No No – more infections in 2007 STEP Merck rAd5: Gag, Pol, Nef No vaccinees than placebo RV144 (Sanofi/Vaxgen) 31% efficacy - first signal 2009 Canarypox Gag, Pol, Env /gp120 in humans for benefit by No boost HIV vaccine HVTN 505 2013 NIAID-VRC: DNA + Ad5 No No gag-pol-nef; Env A, B,C RV-144: Evidence that an AIDS Vaccine Can Prevent HIV-1 Infection in Humans Vaccination with ALVAC and AIDSVAX to Prevent HIV-1 Infection in Thailand. -

PHASE III AIDS VACCINE TRIAL in THAILAND Preparing for Results from the ALVAC-AIDSVAX Prime-Boost Vaccine Trial
ANTICIPATING THE RESULTS OF THE PHASE III AIDS VACCINE TRIAL IN THAILAND Preparing for results from the ALVAC-AIDSVAX Prime-Boost vaccine trial September 2009 PREPARING FOR DATA: TABLE OF CONTENTS WHAT WILL WE KNOW, AND WHEN? Preparing for data: What will we know, and when? ...........................1 In September 2009 results will be released from an AIDS vaccine phase III trial in Thailand. This What vaccine regimen did the Thai vaccine trial test? ......................2 test-of-concept trial is the largest AIDS vaccine trial ever conducted. The study, known as RV 144, Historical perspectives on the trial ........2 began in 2003 and enrolled more than 16,000 HIV-negative Thai men and women between the HIV subtype and vaccine design ..........3 ages of 18 and 30. The study was conducted by What was the trial design? ..............4 the Thai Ministry of Public Health (MOPH), sponsored by the US Army Surgeon General, What kinds of results might come from the trial? .............................5 and managed by the US Military HIV Research Program. The US National Institute of Allergy What happens if there is no effect? ........5 and Infectious Diseases (NIAID) and the US Army Medical Research and Materiel Command What happens if there is a positive result? ........................6 provided funding, with in-kind contributions from vaccine manufacturers Sanofi Pasteur and Global Looking ahead ........................7 Solutions for Infectious Diseases (GSID). (GSID now holds the intellectual property rights to the BOXES, FIGURES & TABLES: AIDSVAX vaccine included in the trial which was originally manufactured by Genentech, and Box: Advocates’ Guide to Statistical Terms .......................3 developed and previously owned by VaxGen.) Box: Why is the trial looking for vaccine In late September, the first announcement of impact on viral load? ...................5 data will focus on the general findings: whether there was any evidence of vaccine impact on Map: Thai Trial Locations ................7 HIV infection and/or viral load.