Early Warning Signs of Autism Spectrum Disorder
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Autism Practice Parameters
American Academy of Child and Adolescent Psychiatry AACAP is pleased to offer Practice Parameters as soon as they are approved by the AACAP Council, but prior to their publication in the Journal of the American Academy of Child and Adolescent Psychiatry (JAACAP). This article may be revised during the JAACAP copyediting, author query, and proof reading processes. Any final changes in the document will be made at the time of print publication and will be reflected in the final electronic version of the Practice Parameter. AACAP and JAACAP, and its respective employees, are not responsible or liable for the use of any such inaccurate or misleading data, opinion, or information contained in this iteration of this Practice Parameter. PRACTICE PARAMETER FOR THE ASSESSMENT AND TREATMENT OF CHILDREN AND ADOLESCENTS WITH AUTISM SPECTRUM DISORDER ABSTRACT Autism spectrum disorder (ASD) is characterized by patterns of delay and deviance in the development of social, communicative, and cognitive skills which arise in the first years of life. Although frequently associated with intellectual disability, this condition is distinctive in terms of its course, impact, and treatment. ASD has a wide range of syndrome expression and its management presents particular challenges for clinicians. Individuals with an ASD can present for clinical care at any point in development. The multiple developmental and behavioral problems associated with this condition necessitate multidisciplinary care, coordination of services, and advocacy for individuals and their families. Early, sustained intervention and the use of multiple treatment modalities are indicated. Key Words: autism, practice parameters, guidelines, developmental disorders, pervasive developmental disorders. ATTRIBUTION This parameter was developed by Fred Volkmar, M.D., Matthew Siegel, M.D., Marc Woodbury-Smith, M.D., Bryan King, M.D., James McCracken, M.D., Matthew State, M.D., Ph.D. -

The TEACCH Program in the Era of Evidence-Based Practice
J Autism Dev Disord DOI 10.1007/s10803-009-0901-6 ORIGINAL PAPER The TEACCH Program in the Era of Evidence-Based Practice Gary B. Mesibov • Victoria Shea Ó Springer Science+Business Media, LLC 2009 Abstract ‘Evidence-based practice’ as initially defined in children with autism (e.g., Rogers 1998; Rogers and Vis- medicine and adult psychotherapy had limited applicability mara 2008). to autism interventions, but recent elaborations of the The initial definitions for EST in psychology were quite concept by the American Psychological Association (Am rigid (e.g., requiring evidence from at least two group Psychol 61: 271–285, 2006) and Kazdin (Am Psychol studies using randomized controlled trials or nine single- 63(1):146–159, 2008) have increased its relevance to our case studies, using a treatment manual, and employing a field. This article discusses the TEACCH program (of research design that demonstrated that the intervention which the first author is director) as an example of an being studied was better than another treatment [not just evidence-based practice in light of recent formulations of ‘no treatment’ or a ‘waiting list control group’]). These that concept. criteria, designed to evaluate adult psychotherapy, were not a particularly good fit for evaluating autism interventions Keywords TEACCH Á Evidence-based because of the relatively limited research base and the extremely heterogeneous population of people with autism, among other factors (Mesibov and Shea 2009) (The term Brief History of Evidence-Based Practice autism will be used from this point forward to mean all autism spectrum disorders.). The concept of evidence-based interventions began in the Actually, many psychologists chafed under the early field of medicine in the 1970’s and in recent years has been EST criteria, leading the American Psychological Associ- employed in many other disciplines. -

The Effectiveness of Snoezelen in Reducing
234 The effectiveness of Snoezelen in reducing stereotyping in ARTICLE ORIGINAL adults with intellectual disabilities: a case study of Occupational Therapy intervention in multisensory stimulation rooms A eficácia do Snoezelen na redução das estereotipias em adultos com deficiência intelectual: um estudo de caso da intervenção da terapia ocupacional em salas de estimulação multissensorial* Ana Sofia Pinto Lopes1, Janine Vanessa Martins Araújo1, Marco Paulo Vieira Ferreira1, Jaime Emanuel Moreira Ribeiro2 http://dx.doi.org/10.11606/issn.2238-6149.v26i2p234-243 Lopes ASP, Araújo JVM,Ferreira MPV, Ribeiro JEM. The KEYWORDS: Stereotyped behavior; Intellectual disability; effectiveness of Snoezelen in reducing stereotyping in adults with Occupational Therapy. intellectual disabilities: a case study of Occupational Therapy intervention in multisensory stimulation rooms. Rev Ter Ocup Lopes ASP, Araújo JVM, Ferreira MPV, Ribeiro JEM. Univ São Paulo. 2015 May-Aug.;26(2):234-43. A eficácia do Snoezelen na redução das estereotipias em adultos com deficiência intelectual: um estudo de caso da ABSTRACT: There is little evidence of the effectiveness of intervenção da terapia ocupacional em salas de estimulação intervention in Snoezelen rooms in stereotyping reduction multissensorial. Rev Ter Ocup Univ São Paulo. 2015 in adults with intellectual disabilities. In this direction, the maio-ago.;26(2):234-43. present study sought to evaluate the relationship between this multisensory stimulation and stereotyping reduction RESUMO: Existem escassas evidências sobre a eficácia da in adults with intellectual disabilities. Through the case intervenção em salas de Snoezelen na redução de estereotipias em study methodology, the behavior of a subject was analyzed adultos com deficiência intelectual. Neste sentido, o presente estudo before, during and after the multisensory stimulation in pretendeu avaliar a relação entre esta estimulação multissensorial e Snoezelen rooms for ten biweekly sessions, lasting an hour a redução de estereotipias em adultos com deficiência intelectual. -

The Czech Republic: on Its Way from Emigration to Immigration Country
No. 11, May 2009 The Czech Republic: on its way from emigration to immigration country Dušan Drbohlav Department of Social Geography and Regional Development Charles University in Prague Lenka Lachmanová-Medová Department of Social Geography and Regional Development Charles University in Prague Zden ěk Čermák Department of Social Geography and Regional Development Charles University in Prague Eva Janská Department of Social Geography and Regional Development Charles University in Prague Dita Čermáková Department of Social Geography and Regional Development Charles University in Prague Dagmara Dzúrová Department of Social Geography and Regional Development Charles University in Prague Table of contents List of Tables .............................................................................................................................. 3 List of Figures ............................................................................................................................ 4 Introduction ................................................................................................................................ 6 1. Social and Migration Development until 1989 ...................................................................... 7 1.1. Period until the Second World War ................................................................................ 7 1.2. Period from 1945 to 1989 .............................................................................................. 10 2. Social and Migration Development in the Period -

Autism Spectrum Disorder: an Overview and Update
Autism Spectrum Disorder: An Overview and Update Brandon Rennie, PhD Autism and Other Developmental Disabilities Division Center for Development and Disability University of New Mexico Department of Pediatrics DATE, 2016 Acknowledgements: Courtney Burnette, PHD, Sylvia Acosta, PhD, Maryann Trott, MA, BCBA Introduction to Autism Spectrum Disorder (ASD) • What is ASD? • A complex neurodevelopmental condition • Neurologically based- underlying genetic and neurobiological origins • Developmental- evident early in life and impacts social development • Lifelong- no known cure • Core characteristics • Impairments in social interaction and social communication • Presence of restricted behavior, interests and activities • Wide variations in presentation DSM-5 Diagnostic Criteria • Deficits in social communication and social interaction (3) • Social approach/interaction • Nonverbal communication • Relationships • Presence of restricted, repetitive patterns of behavior, interests, or activities (2) • Stereotyped or repetitive motor movements, objects, speech • Routines • Restricted interests • Sensory* From Rain Man To Sheldon Cooper- Autism in the Media 1910 Bleuler • First use of the word autistic • From “autos”, Greek word meaning “self” 1943 Leo Kanner 1944 Hans Asperger 1975 1:5000 1985 1:2500 1995 1:500 “When my brother trained at Children's Hospital at Harvard in the 1970s, they admitted a child with autism, and the head of the hospital brought all of the residents through to see. He said, 'You've got to see this case; you'll never see it -

Strategies in an Arts Program for Adults with Atypical Communication
STRATEGIES IN AN ARTS PROGRAM FOR ADULTS WITH ATYPICAL COMMUNICATION STRATEGIES AND ADAPTATIONS IN AN ARTS PROGRAM FOR ADULTS WITH ATYPICAL COMMUNICATION A Master’s Degree Thesis by Christina Lukac to Moore College of Art & Design In partial fulfillment of the requirements for the degree of MA in Art Education with an Emphasis in Special Populations Philadelphia, PA August 2017 Accepted: ________________________________ Lauren Stichter | Graduate Program Director Masters in Art Education with an Emphasis in Special Populations STRATEGIES IN AN ARTS PROGRAM FOR ADULTS WITH ATYPICAL ii COMMUNICATION Abstract The purpose of this study was to observe and implement strategies and adaptations in an arts program for adults with atypical communication due to developmental and intellectual disabilities. This study was conducted in the field using an action research approach with triangulated methods of data collection including semi- structured interviews, participant observations, and artwork analysis. While research was conducted in two different art programs with similar populations, the main site of study was at SpArc Service’s Cultural Arts Center located in Philadelphia, Pennsylvania. The secondary site was at Center for Creative Works located in Wynnewood, Pennsylvania. The data collected between these sites produced common trends in strategies and adaptations that are used in the art room. Individual case studies conducted at SpArc Services allowed strategies to be implemented and documented in the art room. When implementing these findings, I saw how these strategies supported the participant’s goals as outlined in their Individual Outcome Summary. While working with the individual participants, areas of art making included textiles, mixed-media materials, and pop culture references. -

Autism Terminology Guidelines
The language we use to talk about autism is important. A paper published in our journal (Kenny, Hattersley, Molins, Buckley, Povey & Pellicano, 2016) reported the results of a survey of UK stakeholders connected to autism, to enquire about preferences regarding the use of language. Based on the survey results, we have created guidelines on terms which are most acceptable to stakeholders in writing about autism. Whilst these guidelines are flexible, we would like researchers to be sensitive to the preferences expressed to us by the UK autism community. Preferred language The survey highlighted that there is no one preferred way to talk about autism, and researchers must be sensitive to the differing perspectives on this issue. Amongst autistic adults, the term ‘autistic person/people’ was the most commonly preferred term. The most preferred term amongst all stakeholders, on average, was ‘people on the autism spectrum’. Non-preferred language: 1. Suffers from OR is a victim of autism. Consider using the following terms instead: o is autistic o is on the autism spectrum o has autism / an autism spectrum disorder (ASD) / an autism spectrum condition (ASC) (Note: The term ASD is used by many people but some prefer the term 'autism spectrum condition' or 'on the autism spectrum' because it avoids the negative connotations of 'disability' or 'disorder'.) 2. Kanner’s autism 3. Referring to autism as a disease / illness. Consider using the following instead: o autism is a disability o autism is a condition 4. Retarded / mentally handicapped / backward. These terms are considered derogatory and offensive by members of the autism community and we would advise that they not be used. -
What Is Autism? Autism Is a Complex Brain Disorder That Affects a Child’S Ability to Communicate, Respond to Surroundings, Or Form Relationships with Others
What is autism? Autism is a complex brain disorder that affects a child’s ability to communicate, respond to surroundings, or form relationships with others. Autism is a developmental disorder of the brain that occurs in people of all racial, ethnic and social backgrounds. Children with autism are not unruly kids who choose not to behave. Generally diagnosed at age 2 or 3, few disorders are as devastating to a child and his or her family. Many children with autism will never be able to tell their parents they love them. While some people with autism are mildly affected, most people with the condition will require lifelong supervision and care and have significant language impairments. In the most severe cases, affected children exhibit repetitive, aggressive and self-injurious behavior. This behavior may persist over time and prove very difficult to change, posing a tremendous challenge to those who must live with, treat, teach and care for these individuals. The mildest forms of autism resemble a personality disorder associated with a perceived learning disability. First described over 50 years ago, the incidence of autism is rising steadily. While criteria for diagnosing autism have changed over time and the number of cases reported have increased, studies indicate that: . An estimated one in 1,000 children have autism . Two to five children per 1,000 show some form the disorder . As many as 1.5 million Americans today are believed to have some form of autism. Based on statistics from the U.S. Department of Education and other governmental agencies, autism is growing at a rate of 10-17 percent per year. -

Psychosis and Schizophrenia in Children and Young People'
PSYCHOSIS AND SCHIZOPHRENIA IN CHILDREN AND YOUNG PEOPLE' THE NICE GUIDELINE ON RECOGNITION and MANAGEMENT PSYCHOSIS AND SCHIZOPHRENIA IN CHILDREN AND YOUNG PEOPLE RECOGNITION AND MANAGEMENT National Clinical Guideline Number 155 National Collaborating Centre for Mental Health commissioned by The National Institute for Health and Care Excellence published by The British Psychological Society and The Royal College of Psychiatrists 2572_Book.indb 1 6/27/2013 3:50:03 PM Project3 27/06/2013 15:14 Page 1 © The British Psychological Society & The Royal College of Psychiatrists, 2013 The views presented in this book do not necessarily refl ect those of the British Psychological Society, and the publishers are not responsible for any error of omission or fact. The British Psychological Society is a registered charity (no. 229642). All rights reserved. No part of this book may be reprinted or reproduced or utilised in any form or by any electronic, mechanical, or other means, now known or hereafter invented, including photocopying and recording, or in any information storage or retrieval system, without permission in writing from the publishers. Enquiries in this regard should be directed to the British Psychological Society. British Library Cataloguing-in-Publication Data A catalogue record for this book is available from the British Library. ISBN-: 978-1-908020-60-4 Printed in Great Britain by Stanley L. Hunt (Printers) Ltd. Additional material: data CD-Rom created by Pix18 (www.pix18.co.uk) developed by National Collaborating Centre for Mental -

Before You Donate to Autism Speaks, Consider the Facts
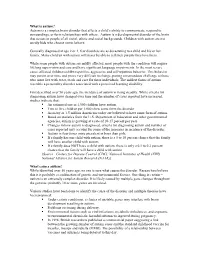
Before you donate to Autism Speaks, Consider the facts Autism Speaks’ Budget Very little money donated to Autism source: Autism Speaks 990 Non-Profit Tax Exemption Form, 2018* Speaks goes toward helping autistic Research “Awareness” & people and families. Lobbying Only 1% of Autism Speaks’ budget goes towards the “Family Service” grants that are the organization’s means of funding services. Autism Speaks spends 20x as much—20%—on fundraising. Although Autism Speaks has not 27% 48% prioritized services with a practical impact for families and individuals in its budget, its rates of executive pay are the highest in the autism world: some salaries exceed $600,000 a year. 20% 4% Autism Speaks talks about us 1% without us. Fundraising Misc. Family Services Autism Speaks has only 1 autistic person out of a total of 28 individuals on its Board of Directors. Instead, donate to organizations By contrast, 23 out of 28 board members represent that help autistic people: major corporations, including current and former Autistic Self Advocacy Network (ASAN) CEOs and senior executives of PayPal, Goldman provides support, community, and public policy Sachs, White Castle, FX Networks, Virgin Mobile, advocacy, by and for people on the autism spectrum. eBay, AMC Networks, L’Oreal, CBS, SiriusXM, autisticadvocacy.org American Express, S.C. Johnson, and Royal Bank Autistic Women & Nonbinary Network (AWN) of Scotland. seeks to share information which works to build acceptance and understanding of disability, while dispelling stereotypes and misinformation which Autism Speaks’ fundraising strategies perpetuate unnecessary fears surrounding an promote fear, stigma, and prejudice autism diagnosis. against autistic people. -

2 the Idea.Pages
THE IDEA ‘Sure I’ve got a minute. What’s your series about?’ Imagine this: through luck or perseverance, you have tracked down the exact producer you want to meet. You’ve done your homework. You know exactly who this person is, what shows they made and why they are perfect to executive produce your series. You’ve got them on the phone or you’ve planted yourself directly in their path outside a screening. However it happens, you’ve got their attention. For about a minute. How you use that minute will determine whether you are invited to come in for a meeting, or whether that producer will excuse themselves with a polite, ‘good luck.’ So what do we say? How do we best answer this basic question: ‘What is your series about?’ I’m going to give you a formula for this in a minute, but before I do, it’s important that you understand that there are at least two levels of communication going on in this situation. There is the WHAT (i.e., basic information that describes your series) and there is the HOW (i.e., the level of confidence and professionalism with which you speak). Which of these two do you think matters most at the outset? You don’t need to be a deep student of psychology or interpersonal relations to know that confidence is crucial in a situation like this. How you communicate matters tremendously. And yet, where is this confidence supposed to come from? You, someone who has never made a tv series? Perhaps never even staffed or written a pilot – how are you supposed to convey the confidence and authority to make this person comfortable enough to trust you? It’s actually pretty simple: practice. -

Teen-Targeted Broadcast TV Can Be Vulgar… but Stranger Things Are
Teen-Targeted Broadcast TV Can Be Vulgar… But Stranger Things Are Happening On Netflix EXECUTIVE SUMMARY The entertainment industry has, for decades, The Parents Television Council renews its call for cautioned parents who want to protect their children wholesale reform to the entertainment industry- from explicit content to rely on the various age- controlled ratings systems and their oversight. based content ratings systems. The movie industry, There should be one uniform age-based content the television industry, the videogame industry rating system for all entertainment media; the and the music industry have, individually, crafted system must be accurate, consistent, transparent medium-specific rating systems as a resource to and accountable to those for whom it is intended to help parents. serve: parents; and oversight of that system should be vested primarily in experts outside of those who In recent years, the Parents Television Council has produce and/or distribute the programming – and produced research documenting a marked increase who might directly or indirectly profit from exposing in profanity airing on primetime broadcast television. children to explicit, adult-themed content. All of the television programming analyzed by the PTC for those research reports was rated as appropriate for children aged 14, or even younger. Today, with much of the nation ostensibly on lockdown as a result of the COVID-19 pandemic, children are at home instead of at school; and as a result, they have far greater access to entertainment media. While all forms of media consumption are up, the volume of entertainment programming being consumed through over-the-top streaming platforms has spiked dramatically.