17, 2009 (Week
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
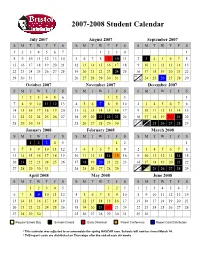
Approved Student Calendar
2007-2008 Student Calendar July 2007 August 2007 September 2007 SMTWT F S SMTWT F S SMTWT F S 1234567 1234 1 8910111213145678910 11 2 3 45678 15 16 17 18 19 20 21 12 13 14 15 16 17 18 9 10 11 12 13 14 15 22 23 24 25 26 27 28 19 20 21 22 23 24 25 16 17 18 19 20 21 22 23 29 30 31 26 27 28 29 30 31 30 24 25 26 27 28 29 October 2007 November 2007 December 2007 SMTWT F S SMTWT F S SMTWT F S 123456 123 1 7891011 12 134567 89102345678 14 15 16 17 18 19 20 11 12 13 14 15 16 17 9 10 11 12 13 14 15 21 22 23 24 25 26 27 18 19 20 21 22 23 24 16 17 18 19 20 21 22 23 24 28 29 30 31 25 26 27 28 29 30 30 31 25 26 27 28 29 January 2008 February 2008 March 2008 SMTWT F S SMTWT F S SMTWT F S 12345 12 1 67891011123456789 2345678 13 14 15 16 17 18 19 10 11 12 13 14 1516 9 1011121314 15 20 21 22 23 24 25 26 17 18 19 20 21 22 23 16 17 18 19 20 21 22 23 24 27 28 29 30 31 24 25 26 27 28 29 30 31 25 26 27 28 29 April 2008 May 2008 June 2008 SMTWT F S SMTWT F S SMTWT F S 12345 123 1234567 6789 10111245678910891011121314 13 14 15 16 17 18 19 11 12 13 14 15 16 17 15 16 17 18 19 20 21 20 21 22 23 24 25 26 18 19 20 21 22 23 24 22 23 24 25 26 27 28 27 28 29 30 25 26 27 28 29 30 31 29 30 Regular School Day Schools Closed Early Dismissal Parent Conference Report Card Distribution * This calendar was adjusted to accommodate the spring NASCAR race. -

October 11, 2011 / Rules and Regulations 62607
Federal Register / Vol. 76, No. 196 / Tuesday, October 11, 2011 / Rules and Regulations 62607 drain is ‘‘unblockable’’ if the suction DEPARTMENT OF THE TREASURY Analyses’’, lines 6 and 7 from the outlet, including the sump, has a bottom of the second paragraph, the perforated (open) area that cannot be Internal Revenue Service phrase ‘‘$2.80 and registered mail can shadowed by the area of the 18″ x 23″ be used for as little as $10.60’’ is Body Blocking Element of ANSI/APSP– 26 CFR Part 301 corrected to read ‘‘$2.85 and registered 16 2011 and the rated flow through any [TD 9543] mail can be used for as little as $10.75.’’ portion of the remaining open area 4. On page 52562, column 3, in the RIN 1545–BA99 (beyond the shadowed portion) cannot preamble, the caption ‘‘List of Subjects in 26 CFR part 301’’ is corrected to read create a suction force in excess of the Timely Mailing Treated as Timely Filing removal force values in Table 1 of that as follows: AGENCY: Standard. The Staff Technical Guidance Internal Revenue Service (IRS), List of Subjects of June 2008 will be updated to clarify Treasury. 26 CFR Part 301 that placing a removable, unblockable ACTION: Correction to final regulations. Employment taxes, Estate taxes, Gift drain cover over a blockable drain does SUMMARY: This document contains taxes, Income taxes, Penalties, Reporting not constitute an unblockable drain. corrections to final regulations that were This revocation corrects the previous published in the Federal Register on and recordkeeping requirements. interpretation, which the Commission Tuesday, August 23, 2011, the 26 CFR Part 602 now believes was in error and thwarts regulations provide that the proper use Reporting and recordkeeping the intent of the law to require layers of of registered or certified mail, or a requirements. -

October 11, 2019
OCTOBER 11, 2019 UPCOMING o Monday, October 14, 3:00 PM - ZORACES Meeting – City Hall o Monday, October 14, 4:00 PM - Environmental Sustainability Subcommittee Meeting – City Hall o Monday, October 14, 6:30 PM - City Council Meeting – City Hall o Monday, October 14, 7:00 PM - Harry Barovsky Memorial Youth Commission – City Hall o Tuesday, October 15, 8:30 AM - Las Virgenes - Malibu Council of Governments Meeting – Agoura Hills City Hall o Wednesday, October 16, – 7:00 PM - Malibu Library Speaker Series featuring Ed Viesturs – City Hall o Thursday, October 17, 6:00 PM - CERT Training – City Hall o Saturday, October 19, 10:00 AM - Electronic & Household Hazardous Waste Collection Event – City Hall SANTA ANA WINDS / RED FLAG FIRE CONDITIONS & PUBLIC SAFETY POWER SHUTOFFS The National Weather Services (NWS) forecasts that Red Flag fire conditions will continue through the end of the day Friday, October 11 in Malibu, and through the end of the day Saturday, October 12 in mountain areas of LA and Ventura Counties including parts of the Santa Monica Mountains, with strong gusty winds and very low humidity. Southern California Edison (SCE) notified the City that it is no longer considering a Public Safety Power Shutoff (PSPS) for western Malibu. However, hazardous fire conditions will continue through the weekend, so residents should stay vigilant. o Learn how to prepare for power outages on LA County's power outage web page and be prepared for any emergency with the County's Ready! Set! Go! guide. o Monitor local news, including KNX AM-1070 and KBUU 99.1-FM on the radio. -

October 11, 2019
[email protected] October 11, 2019 PICTURE DAY MONDAY, OCTOBER 14 October 11, 2019 Dear SMASH 3rd-8th Grade Families, The two weeks of October 14- October 25, SMASH 3rdt-8th graders will be participating in a ~45 minute on- line SMMUSD-selected math interim assessment as well as a ~45 minute on-line SMMUSD-selected English Language Arts interim assessment. (SMASH Core 1 and 2 Teachers and Erin with 5th graders already con- ducted two other literacy assessments, Fastbridge on-line and a 1:1 Teacher’s College teacher/student read- ing assessment) The ELA assessment consists of 12-15 short answer or multiple choice questions in response to text. The Math assessment consists of 12-15 problem-solving questions. How will the results of the interim be used? These are designed to be district wide formative assessments and are intended to be used to monitor stu- dent learning across all sites. Who will see the data? This data will be shared with the Board of Education in a District-wide format by grade levels, individual stu- dent reports will not be provided. If parents are interested in learning about the progress of their student they will be encouraged to speak to their student’s teacher. If you wish to opt your child out of the assessment(s), please email Jessica Rishe at [email protected] by 8:00am Monday, October 14. You message should say: “I would like to opt my child, (first and last name and grade level) out of the October 2019 SMMUSD (math, math and language arts, or just language arts) interim assessments.” If opted out, your child will be given a quiet learning activity in the classroom instead. -

2021 7 Day Working Days Calendar
2021 7 Day Working Days Calendar The Working Day Calendar is used to compute the estimated completion date of a contract. To use the calendar, find the start date of the contract, add the working days to the number of the calendar date (a number from 1 to 1000), and subtract 1, find that calculated number in the calendar and that will be the completion date of the contract Date Number of the Calendar Date Friday, January 1, 2021 133 Saturday, January 2, 2021 134 Sunday, January 3, 2021 135 Monday, January 4, 2021 136 Tuesday, January 5, 2021 137 Wednesday, January 6, 2021 138 Thursday, January 7, 2021 139 Friday, January 8, 2021 140 Saturday, January 9, 2021 141 Sunday, January 10, 2021 142 Monday, January 11, 2021 143 Tuesday, January 12, 2021 144 Wednesday, January 13, 2021 145 Thursday, January 14, 2021 146 Friday, January 15, 2021 147 Saturday, January 16, 2021 148 Sunday, January 17, 2021 149 Monday, January 18, 2021 150 Tuesday, January 19, 2021 151 Wednesday, January 20, 2021 152 Thursday, January 21, 2021 153 Friday, January 22, 2021 154 Saturday, January 23, 2021 155 Sunday, January 24, 2021 156 Monday, January 25, 2021 157 Tuesday, January 26, 2021 158 Wednesday, January 27, 2021 159 Thursday, January 28, 2021 160 Friday, January 29, 2021 161 Saturday, January 30, 2021 162 Sunday, January 31, 2021 163 Monday, February 1, 2021 164 Tuesday, February 2, 2021 165 Wednesday, February 3, 2021 166 Thursday, February 4, 2021 167 Date Number of the Calendar Date Friday, February 5, 2021 168 Saturday, February 6, 2021 169 Sunday, February -

Vol. 44, No. 3, October 11, 1993 University of Michigan Law School
University of Michigan Law School University of Michigan Law School Scholarship Repository Res Gestae Law School History and Publications 1993 Vol. 44, No. 3, October 11, 1993 University of Michigan Law School Follow this and additional works at: http://repository.law.umich.edu/res_gestae Part of the Legal Education Commons Recommended Citation University of Michigan Law School, "Vol. 44, No. 3, October 11, 1993" (1993). Res Gestae. Paper 32. http://repository.law.umich.edu/res_gestae/32 This Article is brought to you for free and open access by the Law School History and Publications at University of Michigan Law School Scholarship Repository. It has been accepted for inclusion in Res Gestae by an authorized administrator of University of Michigan Law School Scholarship Repository. For more information, please contact [email protected]. ' -~-~---OL-L----------------------------------------------------------------------------------------------------------------- UNIV. OF Mlf OCT 1 4 1993 estae LAW LIBRAI Voi.~No . 3 The University of Michigan Law School October 11 , 1993 Survey: Some Claim Sex Harassment By Julie Beck Anolher administration concern RG News Writer which surfaced after lhe survey was In lhesummerof 1992, at a major that women may not speak up about corporation, a second-year law stu thetr experiences because "it can be dent from Michigan "-<IS kissed by a dangerous tocomplain," said Eklund. supervising auomey. After coming One survey response echoed this forward about lhe incident, lhe stu concern: "W h~.:n I came to lhis school, dent worked out a moneta!) settle I was very naJ\·e. I believed lhatthc ment wilh lhe corporauon. work place inevitably was a horrible, That same summer, anolhcr stu d1scriminatOC) place for women and dent associate in a big city was ver thauo 'make it' as a lawyer,you have bally harassed by an attorney wilh to learn to 'take it.' As a result, I d1d whom she worked; he was "let go" as not report lhis firm [where sexual a result of her complaints to senior harassment had occurred to a house auomeys. -

2018 - 2019 Days of Rotation Calendar
2018 - 2019 DAYS OF ROTATION CALENDAR Day # Date Rotation Day Type Notes Day # Date Rotation Day Type Notes Saturday, October 13, 2018 Sunday, October 14, 2018 Monday, September 3, 2018 Holiday/Vaca Labor Day 27 Monday, October 15, 2018 Day 3 In Session 1 Tuesday, September 4, 2018 Day 1 In Session 28 Tuesday, October 16, 2018 Day 4 In Session 2 Wednesday, September 5, 2018 Day 2 In Session 29 Wednesday, October 17, 2018 Day 5 In Session 3 Thursday, September 6, 2018 Day 3 In Session 30 Thursday, October 18, 2018 Day 6 In Session 4 Friday, September 7, 2018 Day 4 In Session 31 Friday, October 19, 2018 Day 1 In Session Saturday, September 8, 2018 Saturday, October 20, 2018 Sunday, September 9, 2018 Sunday, October 21, 2018 Monday, September 10, 2018 Day Holiday/Vaca Rosh Hashanah 32 Monday, October 22, 2018 Day 2 In Session 5 Tuesday, September 11, 2018 Day 5 In Session 33 Tuesday, October 23, 2018 Day 3 In Session 6 Wednesday, September 12, 2018 Day 6 In Session 34 Wednesday, October 24, 2018 Day 4 In Session 7 Thursday, September 13, 2018 Day 1 In Session 35 Thursday, October 25, 2018 Day 5 In Session 8 Friday, September 14, 2018 Day 2 In Session 36 Friday, October 26, 2018 Day 6 In Session Saturday, September 15, 2018 Saturday, October 27, 2018 Sunday, September 16, 2018 Sunday, October 28, 2018 9 Monday, September 17, 2018 Day 3 In Session 37 Monday, October 29, 2018 Day 1 In Session 10 Tuesday, September 18, 2018 Day 4 In Session 38 Tuesday, October 30, 2018 Day 2 In Session Wednesday, September 19, 2018 Day Holiday/Vaca Yom Kippur 39 Wednesday, October 31, 2018 Day 3 In Session 11 Thursday, September 20, 2018 Day 5 In Session 40 Thursday, November 1, 2018 Day 4 In Session 12 Friday, September 21, 2018 Day 6 In Session 41 Friday, November 2, 2018 Day 5 In Session Saturday, September 22, 2018 Saturday, November 3, 2018 Sunday, September 23, 2018 Sunday, November 4, 2018 13 Monday, September 24, 2018 Day 1 In Session 42 Monday, November 5, 2018 Day 6 In Session 14 Tuesday, September 25, 2018 Day 2 In Session Tuesday, November 6, 2018 Prof Dev. -
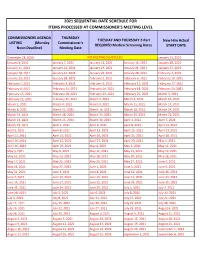
2021 Sequential Date List
2021 SEQUENTIAL DATE SCHEDULE FOR ITEMS PROCESSED AT COMMISSIONER'S MEETING LEVEL COMMISSIONERS AGENDA THURSDAY TUESDAY AND THURSDAY 2-Part New Hire Actual LISTING (Monday Commissioner's REQUIRED Medical Screening Dates START DATE Noon Deadline) Meeting Date December 28, 2020 NO MEETING SCHEDULED January 13, 2021 January 4, 2021 January 7, 2021 January 12, 2021 January 14, 2021 January 20, 2021 January 11, 2021 January 14, 2021 January 19, 2021 January 21, 2021 January 27, 2021 January 18, 2021 January 21, 2021 January 26, 2021 January 28, 2021 February 3, 2021 January 25, 2021 January 28, 2021 February 2, 2021 February 4, 2021 February 10, 2021 February 1, 2021 February 4, 2021 February 9, 2021 February 11, 2021 February 17, 2021 February 8, 2021 February 11, 2021 February 16, 2021 February 18, 2021 February 24, 2021 February 15, 2021 February 18, 2021 February 23, 2021 February 25, 2021 March 3, 2021 February 22, 2021 February 25, 2021 March 2, 2021 March 4, 2021 March 10, 2021 March 1, 2021 March 4, 2021 March 9, 2021 March 11, 2021 March 17, 2021 March 8, 2021 March 11, 2021 March 16, 2021 March 18, 2021 March 24, 2021 March 15, 2021 March 18, 2021 March 23, 2021 March 25, 2021 March 31, 2021 March 22, 2021 March 25, 2021 March 30, 2021 April 1, 2021 April 7, 2021 March 29, 2021 April 1, 2021 April 6, 2021 April 8, 2021 April 14, 2021 April 5, 2021 April 8, 2021 April 13, 2021 April 15, 2021 April 21, 2021 April 12, 2021 April 15, 2021 April 20, 2021 April 22, 2021 April 28, 2021 April 19, 2021 April 22, 2021 April 27, 2021 April -
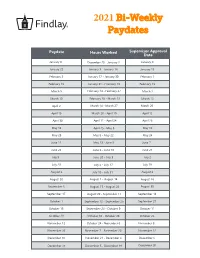
2021 Bi-Weekly Paydates
2021 Bi-Weekly Paydates Paydate Hours Worked Supervisor Approval Date January 8 December 20 - January 2 January 4 January 22 January 3 - January 16 January 15 February 5 January 17 - January 30 February 1 February 19 January 31 - February 13 February 15 March 5 February 14 - February 27 March 1 March 19 February 28 - March 13 March 15 April 2 March 14 - March 27 March 29 April 16 March 28 - April 10 April 12 April 30 April 11 - April 24 April 26 May 14 April 25 - May 8 May 10 May 28 May 9 - May 22 May 24 June 11 May 23 - June 5 June 7 June 25 June 6 - June 19 June 21 July 9 June 20 - July 3 July 2 July 23 July 4 - July 17 July 19 August 6 July 18 - July 31 August 2 August 20 August 1 - August 14 August 16 September 3 August 15 - August 28 August 30 September 17 August 29 - September 11 September 13 October 1 September 12 - September 25 September 27 October 15 September 26 - October 9 October 11 October 29 October 10 - October 23 October 25 November 12 October 24 - November 6 November 8 November 26 November 7 - November 20 November 22 December 10 November 21 - December 4 December 6 December 24 December 5 - December 18 December 20 2021 Bi-Weekly Paydate/Holiday Paydates January February March April Sun Mon Tues Wed Thurs Fri Sat Sun Mon Tues Wed Thurs Fri Sat Sun Mon Tues Wed Thurs Fri Sat Sun Mon Tues Wed Thurs Fri Sat 1 2 1 2 3 4 5 6 1 2 3 4 5 6 1 2 3 4 3 5 6 7 8 9 7 8 9 10 11 12 13 7 8 9 10 11 12 13 4 5 6 7 8 9 10 10 11 12 13 14 15 16 14 15 16 17 18 19 20 14 15 16 17 18 19 20 11 12 13 14 15 16 17 17 18 19 20 21 22 23 21 22 23 24 25 26 -

Pay Date Calendar
Pay Date Information Select the pay period start date that coincides with your first day of employment. Pay Period Pay Period Begins (Sunday) Pay Period Ends (Saturday) Official Pay Date (Thursday)* 1 January 10, 2016 January 23, 2016 February 4, 2016 2 January 24, 2016 February 6, 2016 February 18, 2016 3 February 7, 2016 February 20, 2016 March 3, 2016 4 February 21, 2016 March 5, 2016 March 17, 2016 5 March 6, 2016 March 19, 2016 March 31, 2016 6 March 20, 2016 April 2, 2016 April 14, 2016 7 April 3, 2016 April 16, 2016 April 28, 2016 8 April 17, 2016 April 30, 2016 May 12, 2016 9 May 1, 2016 May 14, 2016 May 26, 2016 10 May 15, 2016 May 28, 2016 June 9, 2016 11 May 29, 2016 June 11, 2016 June 23, 2016 12 June 12, 2016 June 25, 2016 July 7, 2016 13 June 26, 2016 July 9, 2016 July 21, 2016 14 July 10, 2016 July 23, 2016 August 4, 2016 15 July 24, 2016 August 6, 2016 August 18, 2016 16 August 7, 2016 August 20, 2016 September 1, 2016 17 August 21, 2016 September 3, 2016 September 15, 2016 18 September 4, 2016 September 17, 2016 September 29, 2016 19 September 18, 2016 October 1, 2016 October 13, 2016 20 October 2, 2016 October 15, 2016 October 27, 2016 21 October 16, 2016 October 29, 2016 November 10, 2016 22 October 30, 2016 November 12, 2016 November 24, 2016 23 November 13, 2016 November 26, 2016 December 8, 2016 24 November 27, 2016 December 10, 2016 December 22, 2016 25 December 11, 2016 December 24, 2016 January 5, 2017 26 December 25, 2016 January 7, 2017 January 19, 2017 1 January 8, 2017 January 21, 2017 February 2, 2017 2 January -

Due Date Chart 201803281304173331.Xlsx
Special Event Permit Application Due Date Chart for Events from January 1, 2019 - June 30, 2020 If due date lands on a Saturday or Sunday, the due date is moved to the next business day Event Date 30 Calendar days 90 Calendar Days Tuesday, January 01, 2019 Sunday, December 02, 2018 Wednesday, October 03, 2018 Wednesday, January 02, 2019 Monday, December 03, 2018 Thursday, October 04, 2018 Thursday, January 03, 2019 Tuesday, December 04, 2018 Friday, October 05, 2018 Friday, January 04, 2019 Wednesday, December 05, 2018 Saturday, October 06, 2018 Saturday, January 05, 2019 Thursday, December 06, 2018 Sunday, October 07, 2018 Sunday, January 06, 2019 Friday, December 07, 2018 Monday, October 08, 2018 Monday, January 07, 2019 Saturday, December 08, 2018 Tuesday, October 09, 2018 Tuesday, January 08, 2019 Sunday, December 09, 2018 Wednesday, October 10, 2018 Wednesday, January 09, 2019 Monday, December 10, 2018 Thursday, October 11, 2018 Thursday, January 10, 2019 Tuesday, December 11, 2018 Friday, October 12, 2018 Friday, January 11, 2019 Wednesday, December 12, 2018 Saturday, October 13, 2018 Saturday, January 12, 2019 Thursday, December 13, 2018 Sunday, October 14, 2018 Sunday, January 13, 2019 Friday, December 14, 2018 Monday, October 15, 2018 Monday, January 14, 2019 Saturday, December 15, 2018 Tuesday, October 16, 2018 2019 Tuesday, January 15, 2019 Sunday, December 16, 2018 Wednesday, October 17, 2018 Wednesday, January 16, 2019 Monday, December 17, 2018 Thursday, October 18, 2018 Thursday, January 17, 2019 Tuesday, December 18, 2018 -

Minutes of Council Regular Meeting – October 11, 2016 -1
MINUTES OF COUNCIL REGULAR MEETING – OCTOBER 11, 2016 -1- THE WEST VALLEY CITY COUNCIL MET IN REGULAR SESSION ON TUESDAY, OCTOBER 11, 2016, AT 6:30 P.M. IN THE COUNCIL CHAMBERS, WEST VALLEY CITY HALL, 3600 CONSTITUTION BOULEVARD, WEST VALLEY CITY, UTAH. THE MEETING WAS CALLED TO ORDER AND CONDUCTED BY MAYOR BIGELOW. THE FOLLOWING MEMBERS WERE PRESENT: Ron Bigelow, Mayor Lars Nordfelt, Councilmember At-Large Don Christensen, Councilmember At-Large Tom Huynh, Councilmember District 1 Karen Lang, Councilmember District 3 Steve Vincent, Councilmember District 4 (Arrived as noted) ABSENT: Steve Buhler, Councilmember District 2 STAFF PRESENT: Wayne Pyle, City Manager Nichole Camac, City Recorder Paul Isaac, Assistant City Manager/ HR Director Steve Pastorik, Acting CED Director Eric Bunderson, City Attorney Jim Welch, Finance Director Lee Russo, Police Chief John Evans, Fire Chief Russell Willardson, Public Works Director Layne Morris, CPD Kevin Astill, Parks and Recreation Director Sam Johnson, Strategic Communications Director Jake Arslanian, Public Works Department OPENING CEREMONY Lars Nordfelt conducted the Opening Ceremony. He requested members of the City Council, City staff, and the audience to rise while students (Selassie O’Dell, Daniel Nordfelt, Hannah Curtis, and Maddie Hall) from the Hunter High School Madrigals sing the National Anthem. MINUTES OF COUNCIL REGULAR MEETING – OCTOBER 11, 2016 -2- SPECIAL RECOGNITIONS- SCOUTS Mayor Bigelow welcomed Scout Troop No. 917 in attendance at the meeting to complete requirements for the Citizenship in the Community merit badge. APPROVAL OF MINUTES OF REGULAR MEETING HELD OCTOBER 4, 2016 The Council considered the Minutes of the Regular Meeting held October 4, 2016.