Tyrosine Kinase Inhibitors for Solid Tumors in the Past 20 Years (2001–2020) Liling Huang†, Shiyu Jiang† and Yuankai Shi*
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Identification of Recurrent Mutational Events in Anorectal Melanoma
Modern Pathology (2017) 30, 286–296 286 © 2017 USCAP, Inc All rights reserved 0893-3952/17 $32.00 Identification of recurrent mutational events in anorectal melanoma Hui Min Yang1,2,6, Susan J Hsiao1,6, David F Schaeffer2, Chi Lai3, Helen E Remotti1, David Horst4, Mahesh M Mansukhani1 and Basil A Horst1,5 1Department of Pathology & Cell Biology, Columbia University Medical Center, New York, NY, USA; 2Department of Pathology & Laboratory Medicine, University of British Columbia, Vancouver, BC, Canada; 3Department of Pathology and Laboratory Medicine, University of Ottawa, Ottawa, ON, Canada; 4Pathologisches Institut, Ludwig-Maximilians-Universitaet, Muenchen, Germany and 5Department of Dermatology, Columbia University Medical Center, New York, NY, USA Anorectal melanoma is a rare disease that carries a poor prognosis. To date, limited genetic analyses confirmed KIT mutations as a recurrent genetic event similar to other mucosal melanomas, occurring in up to 30% of anorectal melanomas. Importantly, a subset of tumors harboring activating KIT mutations have been found to respond to c-Kit inhibitor-based therapy, with improved patient survival at advanced tumor stages. We performed comprehensive targeted exon sequencing analysis of 467 cancer-related genes in a larger series of 15 anorectal melanomas, focusing on potentially actionable variants based on gain- and loss-of-function mutations. We report the identification of oncogenic driver events in the majority (93%) of anorectal melanomas. These included variants in canonical MAPK pathway effectors rarely observed in cutaneous melanomas (including an HRAS mutation, as well as a BRAF mutation resulting in duplication of threonine 599), and recurrent mutations in the tumor suppressor NF1 in 20% of cases, which represented the second-most frequently mutated gene after KIT in our series. -
Development of a Test That Measures Real-Time HER2 Signaling Function in Live Breast Cancer Cell Lines and Primary Cells Yao Huang1, David J
Huang et al. BMC Cancer (2017) 17:199 DOI 10.1186/s12885-017-3181-0 RESEARCH ARTICLE Open Access Development of a test that measures real-time HER2 signaling function in live breast cancer cell lines and primary cells Yao Huang1, David J. Burns1, Benjamin E. Rich1, Ian A. MacNeil1, Abhijit Dandapat1, Sajjad M. Soltani1, Samantha Myhre1, Brian F. Sullivan1, Carol A. Lange2, Leo T. Furcht3 and Lance G. Laing1* Abstract Background: Approximately 18–20% of all human breast cancers have overexpressed human epidermal growth factor receptor 2 (HER2). Standard clinical practice is to treat only overexpressed HER2 (HER2+) cancers with targeted anti-HER2 therapies. However, recent analyses of clinical trial data have found evidence that HER2-targeted therapies may benefit a sub-group of breast cancer patients with non-overexpressed HER2. This suggests that measurement of other biological factors associated with HER2 cancer, such as HER2 signaling pathway activity, should be considered as an alternative means of identifying patients eligible for HER2 therapies. Methods: A new biosensor-based test (CELxTM HSF) that measures HER2 signaling activity in live cells is demonstrated using a set of 19 human HER2+ and HER2– breast cancer reference cell lines and primary cell samples derived from two fresh patient tumor specimens. Pathway signaling is elucidated by use of highly specific agonists and antagonists. The test method relies upon well-established phenotypic, adhesion-related, impedance changes detected by the biosensor. Results: The analytical sensitivity and analyte specificity of this method was demonstrated using ligands with high affinity and specificity for HER1 and HER3. The HER2-driven signaling quantified ranged 50-fold between the lowest and highest cell lines. -

Entrectinib (Interim Monograph)
Entrectinib (interim monograph) DRUG NAME: Entrectinib SYNONYM(S): RXDX-1011, NMS-E6282 COMMON TRADE NAME(S): ROZLYTREK® CLASSIFICATION: molecular targeted therapy Special pediatric considerations are noted when applicable, otherwise adult provisions apply. MECHANISM OF ACTION: Entrectinib is an orally administered, small molecule, multi-target tyrosine kinase inhibitor which targets tropomyosin- related kinase (Trk) proteins TrkA, TrkB, and TrkC, proto-oncogene tyrosine-protein kinase ROS (ROS1) and anaplastic lymphoma kinase (ALK). TrkA, TrkB, and TrkC are receptor tyrosine kinases encoded by the neurotrophic tyrosine receptor kinase (NTRK) genes NTRK1, NTRK2, and NTRK3, respectively. Fusion proteins that include Trk, ROS1, or ALK kinase domains drive tumorigenic potential through hyperactivation of downstream signalling pathways leading to unconstrained cell proliferation. By potently inhibiting the Trk kinases, ROS1, and ALK, entrectinib inhibits downstream signalling pathways, cell proliferation and induces tumour cell apoptosis.3-5 PHARMACOKINETICS: Oral Absorption bioavailability = 55%; Tmax = 4-6 hours; Tmax delayed 2 h by high-fat, high-calorie food intake Distribution highly bound to human plasma proteins cross blood brain barrier? yes volume of distribution 551 L (entrectinib); 81.1 L (M5) plasma protein binding >99% (entrectinib and M5) Metabolism primarily metabolized by CYP 3A4 active metabolite(s) M5 inactive metabolite(s) M11 Excretion primarily via hepatic clearance urine 3.06% feces 82.9% (36% as unchanged entrectinib, 22% as M5) terminal half life 20 h (entrectinib); 40 h (M5) clearance 19.6 L/h (entrectinib); 52.4 L/h (M5) Elderly no clinically significant difference Children comparable pharmacokinetics of entrectinib and M5 in adults and children Ethnicity no clinically significant difference Adapted from standard reference3,4 unless specified otherwise. -

Adaptive Stress Signaling in Targeted Cancer Therapy Resistance
Oncogene (2015) 34, 5599–5606 © 2015 Macmillan Publishers Limited All rights reserved 0950-9232/15 www.nature.com/onc REVIEW Adaptive stress signaling in targeted cancer therapy resistance E Pazarentzos1,2 and TG Bivona1,2 The identification of specific genetic alterations that drive the initiation and progression of cancer and the development of targeted drugs that act against these driver alterations has revolutionized the treatment of many human cancers. Although substantial progress has been achieved with the use of such targeted cancer therapies, resistance remains a major challenge that limits the overall clinical impact. Hence, despite progress, new strategies are needed to enhance response and eliminate resistance to targeted cancer therapies in order to achieve durable or curative responses in patients. To date, efforts to characterize mechanisms of resistance have primarily focused on molecular events that mediate primary or secondary resistance in patients. Less is known about the initial molecular response and adaptation that may occur in tumor cells early upon exposure to a targeted agent. Although understudied, emerging evidence indicates that the early adaptive changes by which tumor cells respond to the stress of a targeted therapy may be crucial for tumo r cell survival during treatment and the development of resistance. Here we review recent data illuminating the molecular architecture underlying adaptive stress signaling in tumor cells. We highlight how leveraging this knowledge could catalyze novel strategies to minimize -

Targeted Therapies in Advanced Cholangiocarcinoma: a Focus on FGFR Inhibitors
medicina Review Targeted Therapies in Advanced Cholangiocarcinoma: A Focus on FGFR Inhibitors Alessandro Rizzo Department of Experimental, Diagnostic and Specialty Medicine, S. Orsola-Malpighi University Hospital, 40138 Bologna, Italy; [email protected] Abstract: Despite advanced diseases continuing to be associated with grim prognoses, the past decade has witnessed the advent of several novel treatment options for cholangiocarcinoma (CCA) patients. In fact, CCA has emerged as a heterogeneous group of malignancies harboring potentially druggable mutations in approximately 50% of cases, and thus, molecularly targeted therapies have been actively explored in this setting. Among these, fibroblast growth factor receptor (FGFR) inhibitors have reported important results, as witnessed by the FDA approval of pemigatinib in previously treated metastatic CCA patients harboring FGFR2 fusion or other rearrangements. Herein, we provide an overview of available evidence on FGFR inhibitors in CCA, especially focusing on the development, pitfalls and challenges of emerging treatments in this setting. Keywords: FGFR; cholangiocarcinoma; targeted therapies; intrahepatic cholangiocarcinoma; pemi- gatinib 1. Introduction Citation: Rizzo, A. Targeted Cholangiocarcinoma (CCA) encompasses a group of heterogeneous, rare and aggres- Therapies in Advanced sive malignancies, including intrahepatic cholangiocarcinoma (iCCA) and extrahepatic Cholangiocarcinoma: A Focus on cholangiocarcinoma (eCCA), with the latter further subclassified into perihilar (pCCA) FGFR Inhibitors. Medicina 2021, 57, and distal (dCCA) cholangiocarcinoma [1–3]. CCAs account for approximately 3% of 458. https://doi.org/10.3390/ all gastrointestinal cancers worldwide and 10–15% of all primary liver tumors [4–6]. As medicina57050458 suggested by several studies, these subgroups of hepatobiliary tumors not only develop from different anatomical locations, but vary widely in terms of epidemiology, biology, Academic Editor: Zygmunt Warzecha prognosis, and etiology [7–9]. -

Mutant Cancers 2 3 Heinz Hammerlindl1*, Dinoop Ravindran Menon1*, Sabrina Hammerlindl1, Abdullah Al
Author Manuscript Published OnlineFirst on December 1, 2017; DOI: 10.1158/1078-0432.CCR-16-2118 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Hammerlindl et. al 1 Acetylsalicylic Acid Governs the Effect of Sorafenib in RAS Mutant Cancers 2 3 Heinz Hammerlindl1*, Dinoop Ravindran Menon1*, Sabrina Hammerlindl1, Abdullah Al 4 Emran1, Joachim Torrano1, Katrin Sproesser3, Divya Thakkar1, Min Xiao3, Victoria G. 5 Atkinson5, Brian Gabrielli4, Nikolas K. Haass2, Meenhard Herlyn3, Clemens Krepler3, Helmut 6 Schaider1,2† 7 8 1Dermatology Research Centre, The University of Queensland, The University of 9 Queensland Diamantina Institute, Translational Research Institute, Brisbane, Australia; 10 2The University of Queensland, The University of Queensland Diamantina Institute, 11 Translational Research Institute, Brisbane, Australia; 12 3The Wistar Institute, Philadelphia, PA, U.S.A.; 13 4Mater Medical Research Institute, The University of Queensland, Translational Research 14 Institute, Brisbane, Australia; 15 5Division of Cancer Services, Princess Alexandra Hospital, Brisbane, Australia; 16 *These authors contributed equally to the study 17 18 Running title: 19 Combined aspirin and sorafenib for RAS-mutant cancer therapy 20 21 Key words: 22 Melanoma, Lung Cancer, NRAS, Sorafenib, Aspirin, RAS, ERK, AMPK 23 24 25 26 27 28 1 Downloaded from clincancerres.aacrjournals.org on September 24, 2021. © 2017 American Association for Cancer Research. Author Manuscript Published OnlineFirst on December 1, 2017; DOI: 10.1158/1078-0432.CCR-16-2118 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Hammerlindl et. al 1 2 Grant Support 3 This work was funded by the Epiderm Foundation (H.S.), the Princess Alexandra Hospital 4 Research Foundation (PARSS2016_NearMiss) (H.S.), NIH grants PO1 CA114046, P50 5 CA174523, and the Dr. -

07052020 MR ASCO20 Curtain Raiser
Media Release New data at the ASCO20 Virtual Scientific Program reflects Roche’s commitment to accelerating progress in cancer care First clinical data from tiragolumab, Roche’s novel anti-TIGIT cancer immunotherapy, in combination with Tecentriq® (atezolizumab) in patients with PD-L1-positive metastatic non- small cell lung cancer (NSCLC) Updated overall survival data for Alecensa® (alectinib), in people living with anaplastic lymphoma kinase (ALK)-positive metastatic NSCLC Key highlights to be shared on Roche’s ASCO virtual newsroom, 29 May 2020, 08:00 CEST Basel, 7 May 2020 - Roche (SIX: RO, ROG; OTCQX: RHHBY) today announced that new data from clinical trials of 19 approved and investigational medicines across 21 cancer types, will be presented at the ASCO20 Virtual Scientific Program organised by the American Society of Clinical Oncology (ASCO), which will be held 29-31 May, 2020. A total of 120 abstracts that include a Roche medicine will be presented at this year's meeting. "At ASCO, we will present new data from many investigational and approved medicines across our broad oncology portfolio," said Levi Garraway, M.D., Ph.D., Roche's Chief Medical Officer and Head of Global Product Development. “These efforts exemplify our long-standing commitment to improving outcomes for people with cancer, even during these unprecedented times. By integrating our medicines and diagnostics together with advanced insights and novel platforms, Roche is uniquely positioned to deliver the healthcare solutions of the future." Together with its partners, Roche is pioneering a comprehensive approach to cancer care, combining new diagnostics and treatments with innovative, integrated data and access solutions for approved medicines that will both personalise and transform the outcomes of people affected by this deadly disease. -

The Predictive Values of Advanced Non-Small Cell Lung
ORIGINAL RESEARCH published: 26 August 2021 doi: 10.3389/fonc.2021.646577 The Predictive Values of Advanced Non-Small Cell Lung Cancer Patients Harboring Uncommon EGFR Mutations—The Mutation Patterns, Use of Different Generations of EGFR-TKIs, and Concurrent Edited by: Genetic Alterations Francois X. Claret, University of Texas MD Anderson † † Cancer Center, United States Jiarong Tan , Chengping Hu , Pengbo Deng*, Rongjun Wan, Liming Cao, Min Li, Reviewed by: Huaping Yang, Qihua Gu, Jian An and Juan Jiang Lin Liu, Department of Respiratory Medicine, Xiangya Hospital of Central South University, Changsha, China Nankai University, China Hui Guo, First Affiliated Hospital of Xi’an Introduction: Epidermal growth factor receptor (EGFR) 19del and L858R mutation are Jiaotong University, China “ ” Tony Y. Hu, known as common mutations in non-small cell lung cancer (NSCLC) and predict Tulane University, United States sensitivities to EGFR tyrosine kinase inhibitors (TKIs), whereas 20ins and T790M *Correspondence: mutations confer drug-resistance to EGFR-TKIs. The role of the remaining uncommon Pengbo Deng EGFR mutations remains elusive. [email protected] †These authors have contributed Methods: We retrospectively screened a group of NSCLC patients with uncommon equally to this work EGFR mutations other than 20ins and T790M. The mutation patterns, use of different generations of EGFR-TKIs, and concurrent genetic alterations were analyzed. Meanwhile, Specialty section: This article was submitted to a cohort of patients with single 19del or L858R were included for comparison. Cancer Molecular Targets Results: A total of 180/1,300 (13.8%) patients were identified. There were 102 patients and Therapeutics, a section of the journal with advanced or recurrent NSCLC that received first-line therapy of gefitinib/erlotinib/ Frontiers in Oncology icotinib and afatinib and were eligible for analysis. -

New Horizons for Precision Medicine in Biliary Tract Cancers
Published OnlineFirst August 17, 2017; DOI: 10.1158/2159-8290.CD-17-0245 REVIEW New Horizons for Precision Medicine in Biliary Tract Cancers Juan W. Valle1,2, Angela Lamarca1, Lipika Goyal3, Jorge Barriuso1,4, and Andrew X. Zhu3 ABSTRACT Biliary tract cancers (BTC), including cholangiocarcinoma and gallbladder cancer, are poor-prognosis and low-incidence cancers, although the incidence of intrahe- patic cholangiocarcinoma is rising. A minority of patients present with resectable disease but relapse rates are high; benefit from adjuvant capecitabine chemotherapy has been demonstrated.Cisplatin/ gemcitabine combination chemotherapy has emerged as the reference first-line treatment regimen; there is no standard second-line therapy. Selected patients may be suitable for liver-directed therapy (e.g., radioembolization or external beam radiation), pending confirmation of benefit in randomized studies. Initial trials targeting the epithelial growth factor receptor and angiogenesis pathways have failed to deliver new treatments. Emerging data from next-generation sequencing analyses have iden- tified actionable mutations (e.g.,FGFR fusion rearrangements and IDH1 and IDH2 mutations), with several targeted drugs entering clinical development with encouraging results. The role of systemic therapies, including targeted therapies and immunotherapy for BTC, is rapidly evolving and is the sub- ject of this review. Significance: The authors address genetic drivers and molecular biology from a translational per- spective, in an intent to offer a clear view of the recent past, present, and future of BTC. The review describes a state-of-the-art update of the current status and future directions of research and therapy in advanced BTC. Cancer Discov; 7(9); 1–20. -

Therapeutic Targeting of the IGF Axis
cells Review Therapeutic Targeting of the IGF Axis Eliot Osher and Valentine M. Macaulay * Department of Oncology, University of Oxford, Oxford, OX3 7DQ, UK * Correspondence: [email protected]; Tel.: +44-1865617337 Received: 8 July 2019; Accepted: 9 August 2019; Published: 14 August 2019 Abstract: The insulin like growth factor (IGF) axis plays a fundamental role in normal growth and development, and when deregulated makes an important contribution to disease. Here, we review the functions mediated by ligand-induced IGF axis activation, and discuss the evidence for the involvement of IGF signaling in the pathogenesis of cancer, endocrine disorders including acromegaly, diabetes and thyroid eye disease, skin diseases such as acne and psoriasis, and the frailty that accompanies aging. We discuss the use of IGF axis inhibitors, focusing on the different approaches that have been taken to develop effective and tolerable ways to block this important signaling pathway. We outline the advantages and disadvantages of each approach, and discuss progress in evaluating these agents, including factors that contributed to the failure of many of these novel therapeutics in early phase cancer trials. Finally, we summarize grounds for cautious optimism for ongoing and future studies of IGF blockade in cancer and non-malignant disorders including thyroid eye disease and aging. Keywords: IGF; type 1 IGF receptor; IGF-1R; cancer; acromegaly; ophthalmopathy; IGF inhibitor 1. Introduction Insulin like growth factors (IGFs) are small (~7.5 kDa) ligands that play a critical role in many biological processes including proliferation and protection from apoptosis and normal somatic growth and development [1]. IGFs are members of a ligand family that includes insulin, a dipeptide comprised of A and B chains linked via two disulfide bonds, with a third disulfide linkage within the A chain. -
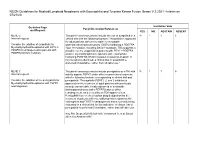
NCCN Guidelines for Myeloid/Lymphoid Neoplasms with Eosinophilia and Tyrosine Kinase Fusion Genes V.2.2021 –Interim on 07/21/20
NCCN Guidelines for Myeloid/Lymphoid Neoplasms with Eosinophilia and Tyrosine Kinase Fusion Genes V.2.2021 –Interim on 07/21/20 Guideline Page Institution Vote Panel Discussion/References and Request YES NO ABSTAIN ABSENT MLNE-5 The panel consensus was to include the use of avapritinib in a 18 1 1 6 Internal request: clinical trial with the following footnote: "Avapritinib is approved for adult patients with unresectable or metastatic Consider the addition of avapritinib for gastrointestinal stromal tumors (GISTs) harboring a PDGFRA Myeloid/lymphoid Neoplasms with FIP1L1- exon 18 mutation, including D842V mutations. This suggests a PDGFRA rearrangement in patients with possible role for avapritinib in patients with FIP1L1-PDGFRA– PDGFRA D842V mutation. positive myeloid/lymphoid neoplasms with eosinophilia harboring PDGFRA D842V mutation resistant to imatinib. If this mutation is identified, a clinical trial of avapritinib is preferred (if available), rather than off-label use." MLNE-7 The panel consensus was to include pemigatinib as a TKI with 18 1 1 6 Internal request: activity against FGFR1 under other recommended regimens with the following footnote corresponding to clinical trial and Consider the addition of the pemigatinib for pemigatinib: "Pemigatinib (FGFR1, 2, and 3 inhibitor) is Myeloid/lymphoid Neoplasms with FGFR1 approved for the treatment of adult patients with previously rearrangement. treated, unresectable, locally advanced or metastatic cholangiocarcinoma and a FGFR2 fusion or other rearrangement, as detected by an FDA-approved test. Pemigatinib has received orphan drug designation for the treatment of patients with myeloid/lymphoid neoplasms with eosinophilia and FGFR1 rearrangement and is currently being evaluated in a clinical trial for this indication. -

Ponatinib Shows Potent Antitumor Activity in Small Cell Carcinoma of the Ovary Hypercalcemic Type (SCCOHT) Through Multikinase Inhibition Jessica D
Published OnlineFirst February 9, 2018; DOI: 10.1158/1078-0432.CCR-17-1928 Cancer Therapy: Preclinical Clinical Cancer Research Ponatinib Shows Potent Antitumor Activity in Small Cell Carcinoma of the Ovary Hypercalcemic Type (SCCOHT) through Multikinase Inhibition Jessica D. Lang1,William P.D. Hendricks1, Krystal A. Orlando2, Hongwei Yin1, Jeffrey Kiefer1, Pilar Ramos1, Ritin Sharma3, Patrick Pirrotte3, Elizabeth A. Raupach1,3, Chris Sereduk1, Nanyun Tang1, Winnie S. Liang1, Megan Washington1, Salvatore J. Facista1, Victoria L. Zismann1, Emily M. Cousins4, Michael B. Major4, Yemin Wang5, Anthony N. Karnezis5, Aleksandar Sekulic1,6, Ralf Hass7, Barbara C. Vanderhyden8, Praveen Nair9, Bernard E. Weissman2, David G. Huntsman5,10, and Jeffrey M. Trent1 Abstract Purpose: Small cell carcinoma of the ovary, hypercalcemic type three SWI/SNF wild-type ovarian cancer cell lines. We further (SCCOHT) is a rare, aggressive ovarian cancer in young women identified ponatinib as the most effective clinically approved that is universally driven by loss of the SWI/SNF ATPase subunits RTK inhibitor. Reexpression of SMARCA4 was shown to confer SMARCA4 and SMARCA2. A great need exists for effective targeted a 1.7-fold increase in resistance to ponatinib. Subsequent therapies for SCCOHT. proteomic assessment of ponatinib target modulation in Experimental Design: To identify underlying therapeutic vul- SCCOHT cell models confirmed inhibition of nine known nerabilities in SCCOHT, we conducted high-throughput siRNA ponatinib target kinases alongside 77 noncanonical ponatinib and drug screens. Complementary proteomics approaches pro- targets in SCCOHT. Finally, ponatinib delayed tumor dou- filed kinases inhibited by ponatinib. Ponatinib was tested for bling time 4-fold in SCCOHT-1 xenografts while reducing efficacy in two patient-derived xenograft (PDX) models and one final tumor volumes in SCCOHT PDX models by 58.6% and cell-line xenograft model of SCCOHT.