Prospective Multicenter Study on the Incidence of Surgical Site Infection
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
SGS-Safeguards 04910- Minimum Wages Increased in Jiangsu -EN-10
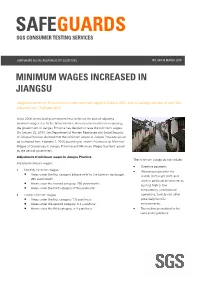
SAFEGUARDS SGS CONSUMER TESTING SERVICES CORPORATE SOCIAL RESPONSIILITY SOLUTIONS NO. 049/10 MARCH 2010 MINIMUM WAGES INCREASED IN JIANGSU Jiangsu becomes the first province to raise minimum wages in China in 2010, with an average increase of over 12% effective from 1 February 2010. Since 2008, many local governments have deferred the plan of adjusting minimum wages due to the financial crisis. As economic results are improving, the government of Jiangsu Province has decided to raise the minimum wages. On January 23, 2010, the Department of Human Resources and Social Security of Jiangsu Province declared that the minimum wages in Jiangsu Province would be increased from February 1, 2010 according to Interim Provisions on Minimum Wages of Enterprises in Jiangsu Province and Minimum Wages Standard issued by the central government. Adjustment of minimum wages in Jiangsu Province The minimum wages do not include: Adjusted minimum wages: • Overtime payment; • Monthly minimum wages: • Allowances given for the Areas under the first category (please refer to the table on next page): middle shift, night shift, and 960 yuan/month; work in particular environments Areas under the second category: 790 yuan/month; such as high or low Areas under the third category: 670 yuan/month temperature, underground • Hourly minimum wages: operations, toxicity and other Areas under the first category: 7.8 yuan/hour; potentially harmful Areas under the second category: 6.4 yuan/hour; environments; Areas under the third category: 5.4 yuan/hour. • The welfare prescribed in the laws and regulations. CORPORATE SOCIAL RESPONSIILITY SOLUTIONS NO. 049/10 MARCH 2010 P.2 Hourly minimum wages are calculated on the basis of the announced monthly minimum wages, taking into account: • The basic pension insurance premiums and the basic medical insurance premiums that shall be paid by the employers. -

BANK of JIANGSU CO., LTD.Annual Report 2015
BANK OF JIANGSU CO., LTD.Annual Report 2015 Address:No. 26, Zhonghua Road, Nanjing, Jiangsu Province, China PC:210001 Tel:025-58587122 Web:http://www.jsbchina.cn Copyright of this annual report is reserved by Bank of Jiangsu, and this report cannot be reprinted or reproduced without getting permission. Welcome your opinions and suggestions on this report. Important Notice I. Board of Directors, Board of Supervisors as well as directors, supervisors and senior administrative officers of the Company warrant that there are no false representations or misleading statements contained in this report, and severally and jointly take responsibility for authenticity, accuracy and completeness of the information contained in this report. II. The report was deliberated and approved in the 19th board meeting of the Third Board of Directors on February 1, 2016. III. Except otherwise noted, financial data and indexes set forth in the Annual Report are consolidated financial data of Bank of Jiangsu Co., Ltd., its subsidiary corporation Jiangsu Danyang Baode Rural Bank Co., Ltd. and Suxing Financial Leasing Co., Ltd. IV. Annual financial report of the Company was audited by BDO China Shu Lun Pan Certified Accountants LLP, and the auditor issued an unqualified opinion. V. Xia Ping, legal representative of the Company, Ji Ming, person in charge of accounting work, and Luo Feng, director of the accounting unit, warrant the authenticity, accuracy and integrality of the financial report in the Annual Report. Signatures of directors: Xia Ping Ji Ming Zhu Qilon Gu Xian Hu Jun Wang Weihong Jiang Jian Tang Jinsong Shen Bin Du Wenyi Gu Yingbin Liu Yuhui Yan Yan Yu Chen Yang Tingdong Message from the Chairman and service innovation, made great efforts to risk prevention and control, promoted endogenous growth, improved service efficiency and made outstanding achievements. -

Supplemental Material
Supplemental material The treatment effects of systematic two-stent and provisional stenting techniques in patients with complex coronary bifurcation lesions: Rationale and design of a prospective, randomized, and multicenter DEFINITION Ⅱ Trial Jun-Jie Zhang,1 Xiao-Fei Gao,1 Ya-Ling Han,2 Jing Kan,3 Ling Tao,4 Zhen Ge,1 Damras Tresukosol,5 Shu Lu,6 Li-Kun Ma,7 Feng Li,8 Song Yang,9 Jun Zhang,10 Muhammad Munawar,11 Li Li,12 Rui-Yan Zhang,13 He-Song Zeng,14 Teguh Santoso,15 Ping Xie,16 Ze-Ning Jin,17 Leng Han,18 Wei-Hsian Yin,19 Xue-Song Qian,20 Qi-Hua Li,21 Lang Hong,22 Chotnoparatpat Paiboon,23 Yan Wang,24 Li-Jun Liu,25 Lei Zhou,26 Xue-Ming Wu,27 Shang-Yu Wen,28 Qing-Hua Lu,29 Jun-Qiang Yuan,30 Liang-Long Chen,31 Francesco Lavarra,32 Alfredo E. Rodríguez,33 Li-Min Zhou,34 Shi-Qin Ding,35 Kitigon Vichairuangthum,36 Yuan-Sheng Zhu,37 Meng-Yue Yu,38 Chan Chen,39 Imad Sheiban,40 Yong Xia,41 Yu-Long Tian,42 Zheng-Lu Shang,43 Qing Jiang,44 Yong-Hong Zhen,45 Xin Wang,46 Fei Ye,1 Nai-Liang Tian,1 Song Lin,1 Zhi-Zhong Liu,1 Shao-Liang Chen,1,3* Zhang JJ and Gao XF contributed equally to this work. *Correspondence author: Shao-Liang Chen, Department of cardiology, Nanjing First Hospital, Nanjing Medical University; No. 68 Changle road, 210006 Nanjing, China; Tel & Fax: +86-25-52208048; E-mail: [email protected]. 1Department of Cardiology, Nanjing First Hospital, Nanjing Medical University, Nanjing, China; 2Department of Cardiology, The General Hospital of Shenyang Military, Shenyang, China; 3Department of Cardiology, Nanjing Heart Center, Nanjing, -

Everbright and the Government of Liyang, Jiangsu Jointly Establish a Fund of Funds with a Targeted Size of RMB 2 Billion
Everbright and the Government of Liyang, Jiangsu Jointly Establish a Fund of Funds with a targeted size of RMB 2 Billion. The AUM of Everbright’s FoF reached RMB 17.1 Billion A strategic co-operation signing ceremony was held at China Everbright Limited (“Everbright”, stock code: 165.HK) with the People’s Government of Liyang, Jiangsu (“Liyang Government”) and China Everbright bank, Changzhou branch on 20th November. 2018. At the ceremony, Everbright and Liyang Government have signed a series of legal documents including Limited Partnership Agreement to establish the Liyang-Everbright fund of funds with a targeted size of RMB 2 billion. Jiangsu Pingling Construction Investment Group Co., Ltd.(Pingling Group) , a wholly owned subsidiary subscribed RMB 1 billion and Everbright subscribed RMB 1 billion (RMB 980 million from its LP and RMB 20 million from its GP). The Fund will be managed by the team of Everbright with extensive experience and professional fund managers. Dedicated to emerging industries investment, Liyang- Everbright fund of funds will focus on areas such as intelligent manufacturing, information technology, clean energy, new materials, health care, tourism and entertainment industry, aeronautical and space technologies. The investment fund aims to carry out extensive cooperation in the emerging industry with the support of domestic and global resources, as well as Everbright’s extensive experience in cross border asset management. 中國光大控股有限公司 China Everbright Limited 香港夏愨道 16 號遠東金融中心 46 樓 46/F, Far East Finance Centre,16 Harcourt Road, Hong Kong 電話 T +852 2528 9882 傳真 F +852 2529 0177 www.everbright.com Mr. Xu Huaqin, Mayor of Liyang,Mr. -

Annual Report 2019
HAITONG SECURITIES CO., LTD. 海通證券股份有限公司 Annual Report 2019 2019 年度報告 2019 年度報告 Annual Report CONTENTS Section I DEFINITIONS AND MATERIAL RISK WARNINGS 4 Section II COMPANY PROFILE AND KEY FINANCIAL INDICATORS 8 Section III SUMMARY OF THE COMPANY’S BUSINESS 25 Section IV REPORT OF THE BOARD OF DIRECTORS 33 Section V SIGNIFICANT EVENTS 85 Section VI CHANGES IN ORDINARY SHARES AND PARTICULARS ABOUT SHAREHOLDERS 123 Section VII PREFERENCE SHARES 134 Section VIII DIRECTORS, SUPERVISORS, SENIOR MANAGEMENT AND EMPLOYEES 135 Section IX CORPORATE GOVERNANCE 191 Section X CORPORATE BONDS 233 Section XI FINANCIAL REPORT 242 Section XII DOCUMENTS AVAILABLE FOR INSPECTION 243 Section XIII INFORMATION DISCLOSURES OF SECURITIES COMPANY 244 IMPORTANT NOTICE The Board, the Supervisory Committee, Directors, Supervisors and senior management of the Company warrant the truthfulness, accuracy and completeness of contents of this annual report (the “Report”) and that there is no false representation, misleading statement contained herein or material omission from this Report, for which they will assume joint and several liabilities. This Report was considered and approved at the seventh meeting of the seventh session of the Board. All the Directors of the Company attended the Board meeting. None of the Directors or Supervisors has made any objection to this Report. Deloitte Touche Tohmatsu (Deloitte Touche Tohmatsu and Deloitte Touche Tohmatsu Certified Public Accountants LLP (Special General Partnership)) have audited the annual financial reports of the Company prepared in accordance with PRC GAAP and IFRS respectively, and issued a standard and unqualified audit report of the Company. All financial data in this Report are denominated in RMB unless otherwise indicated. -

Results Announcement for the Year Ended December 31, 2020
(GDR under the symbol "HTSC") RESULTS ANNOUNCEMENT FOR THE YEAR ENDED DECEMBER 31, 2020 The Board of Huatai Securities Co., Ltd. (the "Company") hereby announces the audited results of the Company and its subsidiaries for the year ended December 31, 2020. This announcement contains the full text of the annual results announcement of the Company for 2020. PUBLICATION OF THE ANNUAL RESULTS ANNOUNCEMENT AND THE ANNUAL REPORT This results announcement of the Company will be available on the website of London Stock Exchange (www.londonstockexchange.com), the website of National Storage Mechanism (data.fca.org.uk/#/nsm/nationalstoragemechanism), and the website of the Company (www.htsc.com.cn), respectively. The annual report of the Company for 2020 will be available on the website of London Stock Exchange (www.londonstockexchange.com), the website of the National Storage Mechanism (data.fca.org.uk/#/nsm/nationalstoragemechanism) and the website of the Company in due course on or before April 30, 2021. DEFINITIONS Unless the context otherwise requires, capitalized terms used in this announcement shall have the same meanings as those defined in the section headed “Definitions” in the annual report of the Company for 2020 as set out in this announcement. By order of the Board Zhang Hui Joint Company Secretary Jiangsu, the PRC, March 23, 2021 CONTENTS Important Notice ........................................................... 3 Definitions ............................................................... 6 CEO’s Letter .............................................................. 11 Company Profile ........................................................... 15 Summary of the Company’s Business ........................................... 27 Management Discussion and Analysis and Report of the Board ....................... 40 Major Events.............................................................. 112 Changes in Ordinary Shares and Shareholders .................................... 149 Directors, Supervisors, Senior Management and Staff.............................. -

Effects Analysis in Abuse of Dominance Cases in China – Is Qihoo 360 V Tencent a Game-Changer?*
Effects Analysis in Abuse of Dominance Cases in China – Is Qihoo 360 v Tencent a Game-Changer?* Adrian Emch Introduction In June 2014, the General Court of the European Union (EU) issued its judgment in the Intel case. The judgment created quite some controversy in antitrust circles. One of the reasons was that the General Court concluded, essentially, that a showing of actual anti-competitive effects was not required for Intel’s conduct to be illegal.1 This position contrasts with US antitrust law, where an analysis of competitive effects is generally required for monopolisation cases – ie, the equivalent to abuse of dominance cases in the EU.2 With these divergent EU and US approaches, this article examines where Chinese antitrust law positions itself on this key issue. In particular, the article focuses on two questions: (1) are Chinese antitrust authorities and courts required to examine effects before finding an illegal abuse of dominance; and (2) what kind of effects are examined? * A version of this article will appear in Philip Lowe, Mel Marquis and Giorgio Monti (eds), What is a Uniform Application of EU Competition Law? Hart Publishing (forthcoming). The author would like to thank Thomas Cheng and Liyang Hou for their invaluable comments on earlier drafts of this article, and Qing Lyu for her support in putting it together. 1 Case T-286/09, Intel v European Commission, 12 June 2014, [2014] ECR II-0000, paras 103–104, for example. 2 See, for example, United States v Microsoft Corp, 253 F.3d 34, 58 (DC Cir 2001) (en banc) (per curiam). -

Transmissibility of Hand, Foot, and Mouth Disease in 97 Counties of Jiangsu Province, China, 2015- 2020
Transmissibility of Hand, Foot, and Mouth Disease in 97 Counties of Jiangsu Province, China, 2015- 2020 Wei Zhang Xiamen University Jia Rui Xiamen University Xiaoqing Cheng Jiangsu Provincial Center for Disease Control and Prevention Bin Deng Xiamen University Hesong Zhang Xiamen University Lijing Huang Xiamen University Lexin Zhang Xiamen University Simiao Zuo Xiamen University Junru Li Xiamen University XingCheng Huang Xiamen University Yanhua Su Xiamen University Benhua Zhao Xiamen University Yan Niu Chinese Center for Disease Control and Prevention, Beijing City, People’s Republic of China Hongwei Li Xiamen University Jian-li Hu Jiangsu Provincial Center for Disease Control and Prevention Tianmu Chen ( [email protected] ) Page 1/30 Xiamen University Research Article Keywords: Hand foot mouth disease, Jiangsu Province, model, transmissibility, effective reproduction number Posted Date: July 30th, 2021 DOI: https://doi.org/10.21203/rs.3.rs-752604/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 2/30 Abstract Background: Hand, foot, and mouth disease (HFMD) has been a serious disease burden in the Asia Pacic region represented by China, and the transmission characteristics of HFMD in regions haven’t been clear. This study calculated the transmissibility of HFMD at county levels in Jiangsu Province, China, analyzed the differences of transmissibility and explored the reasons. Methods: We built susceptible-exposed-infectious-asymptomatic-removed (SEIAR) model for seasonal characteristics of HFMD, estimated effective reproduction number (Reff) by tting the incidence of HFMD in 97 counties of Jiangsu Province from 2015 to 2020, compared incidence rate and transmissibility in different counties by non -parametric test, rapid cluster analysis and rank-sum ratio. -

Effectiveness of Live Poultry Market Interventions on Human Infection with Avian Influenza A(H7N9) Virus, China Wei Wang,1 Jean Artois,1 Xiling Wang, Adam J
RESEARCH Effectiveness of Live Poultry Market Interventions on Human Infection with Avian Influenza A(H7N9) Virus, China Wei Wang,1 Jean Artois,1 Xiling Wang, Adam J. Kucharski, Yao Pei, Xin Tong, Victor Virlogeux, Peng Wu, Benjamin J. Cowling, Marius Gilbert,2 Hongjie Yu2 September 2017) as of March 2, 2018 (2). Compared Various interventions for live poultry markets (LPMs) have with the previous 4 epidemic waves, the 2016–17 fifth emerged to control outbreaks of avian influenza A(H7N9) virus in mainland China since March 2013. We assessed wave raised global concerns because of several char- the effectiveness of various LPM interventions in reduc- acteristics. First, a surge in laboratory-confirmed cas- ing transmission of H7N9 virus across 5 annual waves es of H7N9 virus infection was observed in wave 5, during 2013–2018, especially in the final wave. With along with some clusters of limited human-to-human the exception of waves 1 and 4, various LPM interven- transmission (3,4). Second, a highly pathogenic avi- tions reduced daily incidence rates significantly across an influenza H7N9 virus infection was confirmed in waves. Four LPM interventions led to a mean reduction Guangdong Province and has caused further human of 34%–98% in the daily number of infections in wave 5. infections in 3 provinces (5,6). The genetic divergence Of these, permanent closure provided the most effective of H7N9 virus, its geographic spread (7), and a much reduction in human infection with H7N9 virus, followed longer epidemic duration raised concerns about an by long-period, short-period, and recursive closures in enhanced potential pandemic threat in 2016–17. -

Entity List; One of These Entities Is of an Autopilot and Stability 3911, Email: [email protected]
83416 Federal Register / Vol. 85, No. 246 / Tuesday, December 22, 2020 / Rules and Regulations under Docket No. FAA–2020–1102. DATES: This rule is effective December illustrative list of activities that could be Those special conditions were 18, 2020. considered contrary to the national published in the Federal Register on FOR FURTHER INFORMATION CONTACT: security or foreign policy interests of the December 11, 2020 (85 FR 79826). Chair, End-User Review Committee, United States. Those special conditions pertain to the Office of the Assistant Secretary, Export This rule implements the decision of Bell Textron Canada Limited Model 505 Administration, Bureau of Industry and the ERC to add seventy-seven entities, helicopter, as modified by Garmin Security, Department of Commerce, under a total of seventy-eight entries, to International, Inc., with the installation Phone: (202) 482–5991, Fax: (202) 482– the Entity List; one of these entities is of an autopilot and stability 3911, Email: [email protected]. being added under two entries. These augmentation system. The effective date SUPPLEMENTARY INFORMATION: seventy-seven entities will be listed on was inadvertently omitted from the final the Entity List under the following special conditions. This correction Background destinations, as applicable, China, includes the effective date for those The Entity List (supplement No. 4 to Bulgaria, France, Germany, Hong Kong, special conditions. There are no part 744 of the Export Administration Italy, Malta, Pakistan, Russia, and the substantive changes to the document. Regulations (EAR)) identifies entities for U.A.E. The ERC made the decision to which there is reasonable cause to add each of the seventy-seven entities Issued in Fort Worth, Texas. -

Spatial and Temporal Evaluation of Ecological Footprint Intensity of Jiangsu Province at the County-Level Scale
International Journal of Environmental Research and Public Health Article Spatial and Temporal Evaluation of Ecological Footprint Intensity of Jiangsu Province at the County-Level Scale Decun Wu 1 and Jinping Liu 2,* 1 School of Public Administration and Sociology, Jiangsu Normal University, Xuzhou 221116, China; [email protected] 2 School of Economics and Management, China University of Mining and Technology, Xuzhou 221116, China * Correspondence: [email protected] Received: 10 September 2020; Accepted: 23 October 2020; Published: 26 October 2020 Abstract: Due to the high ecological pressure that exists in the process of rapid economic development in Jiangsu Province, it is necessary to evaluate its ecological footprint intensity (EFI). This article focuses on ecological footprint intensity analysis at the county scale. We used county-level data to evaluate the spatial distributions and temporal trends of the ecological footprint intensity in Jiangsu’s counties from 1995 to 2015. The temporal trends of counties are divided into five types: linear declining type, N-shape type, inverted-N type, U-shape type and inverted-U shape type. It was discovered that the proportions of the carbon footprint intensity were maintained or increased in most counties. Exploratory spatial data analysis shows that there was a certain regularity of the EFI spatial distributions, i.e., a gradient decrease from north to south, and there was a decline in the spatial heterogeneity of EFI in Jiangsu’s counties over time. The global Moran’s index (Moran’s I) and local spatial association index (LISA) are used to analyze both the global and local spatial correlation of EFIs among counties of Jiangsu Province. -

Serum Zinc Level and Tissue ZIP4 Expression Are Related to the Prognosis of Patients with Stages I–III Colon Cancer
5594 Original Article Serum zinc level and tissue ZIP4 expression are related to the prognosis of patients with stages I–III colon cancer Xin Wu1, Han Wu2, Liyang Liu1, Guanghui Qiang1, Jianwei Zhu3 1Department of General Surgery, the Affiliated Nanjing Jiangbei Hospital of Nantong University, Nanjing, China; 2Department of General Surgery, the Affiliated Hospital of Nantong University, Nantong, China; 3Department of Gastrointestinal Surgery, the Affiliated Hospital of Nantong University, Nantong, China Contributions: (I) Conception and design: X Wu, H Wu, J Zhu; (II) Administrative support: J Zhu; (III) Provision of study materials or patients: X Wu, H Wu, L Liu, G Qiang; (IV) Collection and assembly of data: X Wu, H Wu, L Liu, G Qiang; (V) Data analysis and interpretation: X Wu, H Wu; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: Jianwei Zhu. Department of Gastrointestinal Surgery, the Affiliated Hospital of Nantong University, 20 Xisi Road, Nantong, China. Email: [email protected]. Background: It has been reported that serum Zinc (Zn) and tissue ZRT, IRT-like protein 4 (ZIP4) are involved in the oncogenesis of several cancers. However, the relationship between them and the prognosis of colon cancer is unclear. Methods: This was a prospective study including 116 patients with stages I–III colon cancer. The level of serum Zn was measured using a flame atomic absorption spectrometer. The expressions of ZIP4 in cancer tissues were measured using western blot and normal colon tissues from healthy volunteers were used as a control. The primary outcome was 2-year survival and secondary outcomes included the incidences of locoregional recurrence and distant metastasis.