Treating Autism Spectrum Disorder with Gluten-Free and Casein-Free Diet: the Underlying Microbio- Ta-Gut-Brain Axis Mechanisms
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Casomorphins and Gliadorphins Have Diverse Systemic Effects Spanning Gut, Brain and Internal Organs
International Journal of Environmental Research and Public Health Article Casomorphins and Gliadorphins Have Diverse Systemic Effects Spanning Gut, Brain and Internal Organs Keith Bernard Woodford Agri-Food Systems, Lincoln University, Lincoln 7674, New Zealand; [email protected] Abstract: Food-derived opioid peptides include digestive products derived from cereal and dairy diets. If these opioid peptides breach the intestinal barrier, typically linked to permeability and constrained biosynthesis of dipeptidyl peptidase-4 (DPP4), they can attach to opioid receptors. The widespread presence of opioid receptors spanning gut, brain, and internal organs is fundamental to the diverse and systemic effects of food-derived opioids, with effects being evidential across many health conditions. However, manifestation delays following low-intensity long-term exposure create major challenges for clinical trials. Accordingly, it has been easiest to demonstrate causal relationships in digestion-based research where some impacts occur rapidly. Within this environment, the role of the microbiome is evidential but challenging to further elucidate, with microbiome effects ranging across gut-condition indicators and modulators, and potentially as systemic causal factors. Elucidation requires a systemic framework that acknowledges that public-health effects of food- derived opioids are complex with varying genetic susceptibility and confounding factors, together with system-wide interactions and feedbacks. The specific role of the microbiome within -

Epigenetic Effects of Casein-Derived Opioid Peptides in SH-SY5Y Human Neuroblastoma Cells Malav S
Trivedi et al. Nutrition & Metabolism (2015) 12:54 DOI 10.1186/s12986-015-0050-1 RESEARCH Open Access Epigenetic effects of casein-derived opioid peptides in SH-SY5Y human neuroblastoma cells Malav S. Trivedi1*, Nathaniel W. Hodgson2, Stephen J. Walker3, Geert Trooskens4, Vineeth Nair1 and Richard C. Deth1 Abstract Background: Casein-free, gluten-free diets have been reported to mitigate some of the inflammatory gastrointestinal and behavioral traits associated with autism, but the mechanism for this palliative effect has not been elucidated. We recently showed that the opioid peptide beta-casomorphin-7, derived from bovine (bBCM7) milk, decreases cysteine uptake, lowers levels of the antioxidant glutathione (GSH) and decreases the methyl donor S-adenosylmethionine (SAM) in both Caco-2 human GI epithelial cells and SH-SY5Y human neuroblastoma cells. While human breast milk can also release a similar peptide (hBCM-7), the bBCM7 and hBCM-7 vary greatly in potency; as the bBCM-7 is highly potent and similar to morphine in it's effects. Since SAM is required for DNA methylation, we wanted to further investigate the epigenetic effects of these food-derived opioid peptides. In the current study the main objective was to characterize functional pathways and key genes responding to DNA methylation effects of food-derived opioid peptides. Methods: SH-SY5Y neuroblastoma cells were treated with 1 μM hBCM7 and bBCM7 and RNA and DNA were isolated after 4 h with or without treatment. Transcriptional changes were assessed using a microarray approach and CpG methylation status was analyzed at 450,000 CpG sites. Functional implications from both endpoints were evaluated via Ingenuity Pathway Analysis 4.0 and KEGG pathway analysis was performed to identify biological interactions between transcripts that were significantly altered at DNA methylation or transcriptional levels (p < 0.05, FDR <0.1). -

From Opiate Pharmacology to Opioid Peptide Physiology
Upsala J Med Sci 105: 1-16,2000 From Opiate Pharmacology to Opioid Peptide Physiology Lars Terenius Experimental Alcohol and Drug Addiction Section, Department of Clinical Neuroscience, Karolinsku Institutet, S-I71 76 Stockholm, Sweden ABSTRACT This is a personal account of how studies of the pharmacology of opiates led to the discovery of a family of endogenous opioid peptides, also called endorphins. The unique pharmacological activity profile of opiates has an endogenous counterpart in the enkephalins and j3-endorphin, peptides which also are powerful analgesics and euphorigenic agents. The enkephalins not only act on the classic morphine (p-) receptor but also on the 6-receptor, which often co-exists with preceptors and mediates pain relief. Other members of the opioid peptide family are the dynor- phins, acting on the K-receptor earlier defined as precipitating unpleasant central nervous system (CNS) side effects in screening for opiate activity, A related peptide, nociceptin is not an opioid and acts on the separate NOR-receptor. Both dynorphins and nociceptin have modulatory effects on several CNS functions, including memory acquisition, stress and movement. In conclusion, a natural product, morphine and a large number of synthetic organic molecules, useful as drugs, have been found to probe a previously unknown physiologic system. This is a unique develop- ment not only in the neuropeptide field, but in physiology in general. INTRODUCTION Historical background Opiates are indispensible drugs in the pharmacologic armamentarium. No other drug family can relieve intense, deep pain and reduce suffering. Morphine, the prototypic opiate is an alkaloid extracted from the capsules of opium poppy. -

Biased Signaling by Endogenous Opioid Peptides
Biased signaling by endogenous opioid peptides Ivone Gomesa, Salvador Sierrab,1, Lindsay Lueptowc,1, Achla Guptaa,1, Shawn Goutyd, Elyssa B. Margolise, Brian M. Coxd, and Lakshmi A. Devia,2 aDepartment of Pharmacological Sciences, Icahn School of Medicine at Mount Sinai, New York, NY 10029; bDepartment of Physiology & Biophysics, Virginia Commonwealth University, Richmond, VA 23298; cSemel Institute for Neuroscience and Human Behavior, University of California, Los Angeles, CA 90095; dDepartment of Pharmacology & Molecular Therapeutics, Uniformed Services University, Bethesda MD 20814; and eDepartment of Neurology, UCSF Weill Institute for Neurosciences, University of California, San Francisco, CA 94143 Edited by Susan G. Amara, National Institutes of Health, Bethesda, MD, and approved April 14, 2020 (received for review January 20, 2020) Opioids, such as morphine and fentanyl, are widely used for the possibility that endogenous opioid peptides could vary in this treatment of severe pain; however, prolonged treatment with manner as well (13). these drugs leads to the development of tolerance and can lead to For opioid receptors, studies showed that mice lacking opioid use disorder. The “Opioid Epidemic” has generated a drive β-arrestin2 exhibited enhanced and prolonged morphine-mediated for a deeper understanding of the fundamental signaling mecha- antinociception, and a reduction in side-effects, such as devel- nisms of opioid receptors. It is generally thought that the three opment of tolerance and acute constipation (15, 16). This led to types of opioid receptors (μ, δ, κ) are activated by endogenous studies examining whether μOR agonists exhibit biased signaling peptides derived from three different precursors: Proopiomelano- (17–20), and to the identification of agonists that preferentially cortin, proenkephalin, and prodynorphin. -

Nutritional Interventions for Autism Spectrum Disorder
Lead Article Nutritional interventions for autism spectrum disorder Downloaded from https://academic.oup.com/nutritionreviews/advance-article-abstract/doi/10.1093/nutrit/nuz092/5687289 by Florida Atlantic University user on 06 January 2020 Elisa Karhu*, Ryan Zukerman*, Rebecca S. Eshraghi, Jeenu Mittal, Richard C. Deth, Ana M. Castejon, Malav Trivedi, Rahul Mittal, and Adrien A. Eshraghi Autism spectrum disorder (ASD) is an increasingly prevalent neurodevelopmental dis- order with considerable clinical heterogeneity. With no cure for the disorder, treat- ments commonly center around speech and behavioral therapies to improve the characteristic social, behavioral, and communicative symptoms of ASD. Gastrointestinal disturbances are commonly encountered comorbidities that are thought to be not only another symptom of ASD but to also play an active role in modulating the expression of social and behavioral symptoms. Therefore, nutritional interventions are used by a majority of those with ASD both with and without clinical supervision to alleviate gastrointestinal and behavioral symptoms. Despite a consider- able interest in dietary interventions, no consensus exists regarding optimal nutritional therapy. Thus, patients and physicians are left to choose from a myriad of dietary pro- tocols. This review, summarizes the state of the current clinical and experimental liter- ature on nutritional interventions for ASD, including gluten-free and casein-free, keto- genic, and specific carbohydrate diets, as well as probiotics, polyunsaturated fatty -

A Qualitative Assessment of Eating Behaviors in Adults with Autism
Illinois State University ISU ReD: Research and eData Theses and Dissertations 2-21-2015 A Qualitative Assessment Of Eating Behaviors In Adults With Autism Samantha Barbier Illinois State University, [email protected] Follow this and additional works at: https://ir.library.illinoisstate.edu/etd Part of the Human and Clinical Nutrition Commons Recommended Citation Barbier, Samantha, "A Qualitative Assessment Of Eating Behaviors In Adults With Autism" (2015). Theses and Dissertations. 317. https://ir.library.illinoisstate.edu/etd/317 This Thesis is brought to you for free and open access by ISU ReD: Research and eData. It has been accepted for inclusion in Theses and Dissertations by an authorized administrator of ISU ReD: Research and eData. For more information, please contact [email protected]. A QUALITATIVE ASSESSMENT OF EATING BEHAVIORS IN ADULTS WITH AUTISM Samantha J. Barbier 45 Pages May 2015 Diagnosis of autism has increased ten-fold in the last 40 years, and adults with autism remain an underrepresented population in research. The purpose of this study was to qualitatively explore the relationship between eating behaviors and autism using a questionnaire and interviews with adults diagnosed with autism spectrum disorder. Four males aged 22-27 were interviewed with their mothers present and completed the Swedish Eating Assessment for Autism Spectrum Disorders (SWEAA). Interviews were analyzed through the process of open coding, and the questionnaires were analyzed to determine consistent findings between the interview and the SWEAA questionnaire. Participants generally recognized hunger and satiety and were consuming a high carbohydrate, high fat diet low in vegetables. Variety in food choices was highly dependent upon encouragement from family members. -
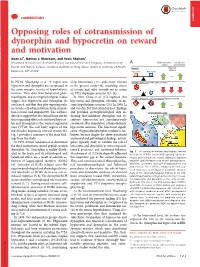
Opposing Roles of Cotransmission of Dynorphin and Hypocretin on Reward and Motivation Xuan Li1, Nathan J
COMMENTARY COMMENTARY Opposing roles of cotransmission of dynorphin and hypocretin on reward and motivation Xuan Li1, Nathan J. Marchant, and Yavin Shaham1 Behavioral Neuroscience Research Branch, Intramural Research Program, Department of A Brain stimulation Cocaine self- reward administration Health and Human Services, National Institute on Drug Abuse, National Institutes of Health, Baseline Impulsive behavior Baltimore, MD 21224 Hypocretin Dynorphin In PNAS, Muschamp et al. (1) report that sleep homeostasis (12), and—most relevant HCRTR1 antagonist: KOR signal dominates hypocretin and dynorphin are coexpressed in to the present study—the rewarding effects the same synaptic vesicles of hypothalamic of cocaine and other rewards via its action neurons. Their data from behavioral, phar- on VTA dopamine neurons (13, 14). macological, and electrophysiological studies In 2001, Chou et al. (15) reported that HCRTR1 antagonist + KOR antagonist: Balance restored suggest that hypocretin and dynorphin are hypocretin and dynorphin colocalize in the coreleased, and that they play opposing roles same hypothalamic neurons (15). In 2006, Li in cocaine self-administration, brain stimula- and van den Pol (16) extended these findings ’ tion reward, and impulsivity. The authors and provided electrophysiological data in- B Ventral tegmental area: data also suggest that the critical brain site for dicating that inhibitory dynorphin and ex- these opposing effects of coreleased hypocre- citatory hypocretin are simultaneously tin and dynorphin is the ventral tegmental coreleased after stimulation of hypothalamic area (VTA), the cell body region of the hypocretin neurons. The functional signifi- mesolimbic dopamine reward system (2). cance of hypocretin/dynorphin corelease is un- Fig. 1 provides a summary of the main find- known, because despite the above-mentioned ings from the study. -

Identifying the Inflammatory Pathways of Genes Upregulated in LADMAC Cells Exposed to BCM7 Oumlissa Persaud [email protected]
Molloy College DigitalCommons@Molloy Biology Undergraduate Thesis Biology, Chemistry, and Environmental Science Fall 2017 Identifying the inflammatory pathways of genes upregulated in LADMAC cells exposed to BCM7 Oumlissa Persaud [email protected] Mary Kusenda Molloy College, [email protected] This research was completed as part of the degree requirements for the Biology Department at Molloy College. Follow this and additional works at: https://digitalcommons.molloy.edu/bio_ug_etd Part of the Biology Commons, and the Food Science Commons DigitalCommons@Molloy Feedback Recommended Citation Persaud, Oumlissa and Kusenda, Mary, "Identifying the inflammatory pathways of genes upregulated in LADMAC cells exposed to BCM7" (2017). Biology Undergraduate Thesis. 1. https://digitalcommons.molloy.edu/bio_ug_etd/1 This Thesis is brought to you for free and open access by the Biology, Chemistry, and Environmental Science at DigitalCommons@Molloy. It has been accepted for inclusion in Biology Undergraduate Thesis by an authorized administrator of DigitalCommons@Molloy. For more information, please contact [email protected],[email protected]. Biology, Chemistry, and Environmental Studies Department i The official copy of the thesis Identifying the inflammatory genes and pathways upregulated in LADMAC cells exposed to BCM7 A Thesis Presented by Oumlissa Persaud To The Undergraduate School in Partial Fulfillment of the Requirements for the Degree of Bachelors of Science Major in Biology at Molloy College 12/18/2017 ii Molloy College Biology, Chemistry and Environmental Studies Department Signature page I certify that I have read the thesis and that, in my humble opinion, I feel it successfully meets the requirements outlined by the thesis board in both scope and quality for the completion of the research track in biology at Molloy College. -

Efficacy and Safety of Gluten-Free and Casein-Free Diets Proposed in Children Presenting with Pervasive Developmental Disorders (Autism and Related Syndromes)
FRENCH FOOD SAFETY AGENCY Efficacy and safety of gluten-free and casein-free diets proposed in children presenting with pervasive developmental disorders (autism and related syndromes) April 2009 1 Chairmanship of the working group Professor Jean-Louis Bresson Scientific coordination Ms. Raphaëlle Ancellin and Ms. Sabine Houdart, under the direction of Professor Irène Margaritis 2 TABLE OF CONTENTS Table of contents ................................................................................................................... 3 Table of illustrations .............................................................................................................. 5 Composition of the working group ......................................................................................... 6 List of abbreviations .............................................................................................................. 7 1 Introduction .................................................................................................................... 8 1.1 Context of request ................................................................................................... 8 1.2 Autism: definition, origin, practical implications ........................................................ 8 1.2.1 Definition of autism and related disorders ......................................................... 8 1.2.2 Origins of autism .............................................................................................. 8 1.1.2.1 Neurobiological -

Medication-Assisted Treatment for Opioid Addiction in Opioid Treatment Programs
Medication-Assisted Treatment For Opioid Addiction in Opioid Treatment Programs A Treatment Improvement Protocol TIP 43 U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Substance Abuse and Mental Health Services Administration Center for Substance Abuse Treatment MEDICATION- www.samhsa.gov ASSISTED TREATMENT Medication-Assisted Treatment For Opioid Addiction in Opioid Treatment Programs Steven L. Batki, M.D. Consensus Panel Chair Janice F. Kauffman, R.N., M.P.H., LADC, CAS Consensus Panel Co-Chair Ira Marion, M.A. Consensus Panel Co-Chair Mark W. Parrino, M.P.A. Consensus Panel Co-Chair George E. Woody, M.D. Consensus Panel Co-Chair A Treatment Improvement Protocol TIP 43 U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Substance Abuse and Mental Health Services Administration Center for Substance Abuse Treatment 1 Choke Cherry Road Rockville, MD 20857 Acknowledgments The guidelines in this document should not be considered substitutes for individualized client Numerous people contributed to the care and treatment decisions. development of this Treatment Improvement Protocol (see pp. xi and xiii as well as Appendixes E and F). This publication was Public Domain Notice produced by Johnson, Bassin & Shaw, Inc. All materials appearing in this volume except (JBS), under the Knowledge Application those taken directly from copyrighted sources Program (KAP) contract numbers 270-99- are in the public domain and may be reproduced 7072 and 270-04-7049 with the Substance or copied without permission from SAMHSA/ Abuse and Mental Health Services CSAT or the authors. Do not reproduce or Administration (SAMHSA), U.S. Department distribute this publication for a fee without of Health and Human Services (DHHS). -

The Role of Protein Convertases in Bigdynorphin and Dynorphin a Metabolic Pathway
Université de Montréal The Role of Protein Convertases in Bigdynorphin and Dynorphin A Metabolic Pathway par ALBERTO RUIZ ORDUNA Département de biomédecine vétérinaire Faculté de médecine vétérinaire Mémoire présenté à la Faculté de médecine vétérinaire en vue de l’obtention du grade de maître ès sciences (M.Sc.) en sciences vétérinaires option pharmacologie Décembre, 2015 © Alberto Ruiz Orduna, 2015 Résumé Les dynorphines sont des neuropeptides importants avec un rôle central dans la nociception et l’atténuation de la douleur. De nombreux mécanismes régulent les concentrations de dynorphine endogènes, y compris la protéolyse. Les Proprotéines convertases (PC) sont largement exprimées dans le système nerveux central et clivent spécifiquement le C-terminale de couple acides aminés basiques, ou un résidu basique unique. Le contrôle protéolytique des concentrations endogènes de Big Dynorphine (BDyn) et dynorphine A (Dyn A) a un effet important sur la perception de la douleur et le rôle de PC reste à être déterminée. L'objectif de cette étude était de décrypter le rôle de PC1 et PC2 dans le contrôle protéolytique de BDyn et Dyn A avec l'aide de fractions cellulaires de la moelle épinière de type sauvage (WT), PC1 -/+ et PC2 -/+ de souris et par la spectrométrie de masse. Nos résultats démontrent clairement que PC1 et PC2 sont impliquées dans la protéolyse de BDyn et Dyn A avec un rôle plus significatif pour PC1. Le traitement en C-terminal de BDyn génère des fragments peptidiques spécifiques incluant dynorphine 1-19, dynorphine 1-13, dynorphine 1-11 et dynorphine 1-7 et Dyn A génère les fragments dynorphine 1-13, dynorphine 1-11 et dynorphine 1-7. -

(D-Ala*)Deltorphin II: D,-Dependent Stereotypies and Stimulation of Dopamine Release in the Nucleus Accumbens
The Journal of Neuroscience, June 1991, 17(6): 1565-l 576 (D-Ala*)Deltorphin II: D,-dependent Stereotypies and Stimulation of Dopamine Release in the Nucleus Accumbens R. Longoni,’ L. Spina,’ A. Mulas,’ E. Carboni,’ L. Garau,’ P. Melchiorri,2 and G. Di Chiaral ‘Institute of Experimental Pharmacology and Toxicology, University of Cagliari, 09100 Cagliari, Italy and 21nstitute of Medical Pharmacology, University of Rome “La Sapienza,” 00185 Rome, Italy In order to investigate the relative role of central 6- and has been implicated in the stimulant actions of systemic opiates. F-opioid receptors in behavior, the effects of (D- Morphine-like opiates stimulate DA release preferentially in the Ala*)cleltorphin II, a natural Gopioid peptide, and PL017, nucleus accumbens (Di Chiara and Imperato, 1988a) and elicit a beta-casomorphin derivative specific for mu receptors, hypermotility sensitive to blockade by the DA D, receptor an- were compared after local intracerebral and intraventricular tagonist SCH 23390 (Longoni et al., 1987a). Intra-accumbens administration. lntracerebral infusion of the two peptides was infusion of opioid peptides elicits motor stimulation, but this done bilaterally in the limbic nucleus accumbens and in the action seems independent from DA, being resistant to classic ventral and dorsal caudate putamen of freely moving rats DA-receptor antagonists (neuroleptics; Pert and Sivit, 1977; Ka- through chronic intracerebral cannulas. After intra-accum- livas et al., 1983). Moreover, the syndrome elicited by intra- bens infusion, the two peptides elicited marked but opposite accumbens opiates is biphasic, as motor stimulation is typically behavioral effects: while (o-Ala2)deltorphin II evoked dose- preceded by motor inhibition and catalepsy (Costa11et al., 1978).