Categorization and Classification of Different ABCA3 Variants Causing Interstitial Lung Disease
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
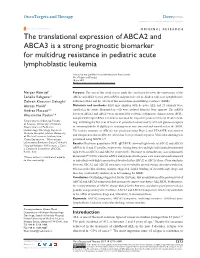
The Translational Expression of ABCA2 and ABCA3 Is a Strong Prognostic Biomarker for Multidrug Resistance in Pediatric Acute Lymphoblastic Leukemia
Journal name: OncoTargets and Therapy Article Designation: Original Research Year: 2017 Volume: 10 OncoTargets and Therapy Dovepress Running head verso: Aberuyi et al Running head recto: ABCA2/A3 transporters and multidrug-resistant ALL open access to scientific and medical research DOI: http://dx.doi.org/10.2147/OTT.S140488 Open Access Full Text Article ORIGINAL RESEARCH The translational expression of ABCA2 and ABCA3 is a strong prognostic biomarker for multidrug resistance in pediatric acute lymphoblastic leukemia Narges Aberuyi1 Purpose: The aim of this work was to study the correlation between the expressions of the Soheila Rahgozar1 ABCA2 and ABCA3 genes at the mRNA and protein levels in children with acute lymphoblastic Zohreh Khosravi Dehaghi1 leukemia (ALL) and the effects of this association on multidrug resistance (MDR). Alireza Moafi2 Materials and methods: Sixty-nine children with de novo ALL and 25 controls were Andrea Masotti3,* enrolled in the study. Mononuclear cells were isolated from the bone marrow. The mRNA Alessandro Paolini3,* levels of ABCA2 and ABCA3 were measured by real-time polymerase chain reaction (PCR). Samples with high mRNA levels were assessed for respective protein levels by Western blot- 1 Department of Biology, Faculty ting. Following the first year of treatment, persistent monoclonality of T-cell gamma receptors of Science, University of Isfahan, 2Department of Pediatric- or immunoglobulin H (IgH) gene rearrangement was assessed and considered as the MDR. Hematology-Oncology, Sayed-ol- The tertiary structure of ABCA2 was predicted using Phyre2 and I-TASSER web systems Shohada Hospital, Isfahan University and compared to that of ABCA3, which has been previously reported. -

EXTENDED CARRIER SCREENING Peace of Mind for Planned Pregnancies
Focusing on Personalised Medicine EXTENDED CARRIER SCREENING Peace of Mind for Planned Pregnancies Extended carrier screening is an important tool for prospective parents to help them determine their risk of having a child affected with a heritable disease. In many cases, parents aren’t aware they are carriers and have no family history due to the rarity of some diseases in the general population. What is covered by the screening? Genomics For Life offers a comprehensive Extended Carrier Screening test, providing prospective parents with the information they require when planning their pregnancy. Extended Carrier Screening has been shown to detect carriers who would not have been considered candidates for traditional risk- based screening. With a simple mouth swab collection, we are able to test for over 419 genes associated with inherited diseases, including Fragile X Syndrome, Cystic Fibrosis and Spinal Muscular Atrophy. The assay has been developed in conjunction with clinical molecular geneticists, and includes genes listed in the NIH Genetic Test Registry. For a list of genes and disorders covered, please see the reverse of this brochure. If your gene of interest is not covered on our Extended Carrier Screening panel, please contact our friendly team to assist you in finding a gene test panel that suits your needs. Why have Extended Carrier Screening? Extended Carrier Screening prior to pregnancy enables couples to learn about their reproductive risk and consider a complete range of reproductive options, including whether or not to become pregnant, whether to use advanced reproductive technologies, such as preimplantation genetic diagnosis, or to use donor gametes. -

Examining the Role of ABC Lipid Transporters in Pulmonary Lipid Homeostasis and Inflammation Amanda B
Chai et al. Respiratory Research (2017) 18:41 DOI 10.1186/s12931-017-0526-9 REVIEW Open Access Examining the role of ABC lipid transporters in pulmonary lipid homeostasis and inflammation Amanda B. Chai1, Alaina J. Ammit2,3* and Ingrid C. Gelissen1 Abstract Respiratory diseases including asthma and chronic obstructive pulmonary disease (COPD) are characterised by excessive and persistent inflammation. Current treatments are often inadequate for symptom and disease control, and hence new therapies are warranted. Recent emerging research has implicated dyslipidaemia in pulmonary inflammation. Three ATP-binding cassette (ABC) transporters are found in the mammalian lung – ABCA1, ABCG1 and ABCA3 – that are involved in movement of cholesterol and phospholipids from lung cells. The aim of this review is to corroborate the current evidence for the role of ABC lipid transporters in pulmonary lipid homeostasis and inflammation. Here, we summarise results from murine knockout studies, human diseases associated with ABC transporter mutations, and in vitro studies. Disruption to ABC transporter activity results in lipid accumulation and elevated levels of inflammatory cytokines in lung tissue. Furthermore, these ABC-knockout mice exhibit signs of respiratory distress. ABC lipid transporters appear to have a crucial and protective role in the lung. However, our knowledge of the underlying molecular mechanisms for these benefits requires further attention. Understanding the relationship between cholesterol and inflammation in the lung, and the role that ABC transporters play in this may illuminate new pathways to target for the treatment of inflammatory lung diseases. Keywords: ABC transporters, ABCA1, ABCG1, ABCA3, Lipids, Surfactant, Pulmonary inflammation Background lung tissue of patients with COPD [5]. -

Seq2pathway Vignette
seq2pathway Vignette Bin Wang, Xinan Holly Yang, Arjun Kinstlick May 19, 2021 Contents 1 Abstract 1 2 Package Installation 2 3 runseq2pathway 2 4 Two main functions 3 4.1 seq2gene . .3 4.1.1 seq2gene flowchart . .3 4.1.2 runseq2gene inputs/parameters . .5 4.1.3 runseq2gene outputs . .8 4.2 gene2pathway . 10 4.2.1 gene2pathway flowchart . 11 4.2.2 gene2pathway test inputs/parameters . 11 4.2.3 gene2pathway test outputs . 12 5 Examples 13 5.1 ChIP-seq data analysis . 13 5.1.1 Map ChIP-seq enriched peaks to genes using runseq2gene .................... 13 5.1.2 Discover enriched GO terms using gene2pathway_test with gene scores . 15 5.1.3 Discover enriched GO terms using Fisher's Exact test without gene scores . 17 5.1.4 Add description for genes . 20 5.2 RNA-seq data analysis . 20 6 R environment session 23 1 Abstract Seq2pathway is a novel computational tool to analyze functional gene-sets (including signaling pathways) using variable next-generation sequencing data[1]. Integral to this tool are the \seq2gene" and \gene2pathway" components in series that infer a quantitative pathway-level profile for each sample. The seq2gene function assigns phenotype-associated significance of genomic regions to gene-level scores, where the significance could be p-values of SNPs or point mutations, protein-binding affinity, or transcriptional expression level. The seq2gene function has the feasibility to assign non-exon regions to a range of neighboring genes besides the nearest one, thus facilitating the study of functional non-coding elements[2]. Then the gene2pathway summarizes gene-level measurements to pathway-level scores, comparing the quantity of significance for gene members within a pathway with those outside a pathway. -

ABCG1 (ABC8), the Human Homolog of the Drosophila White Gene, Is a Regulator of Macrophage Cholesterol and Phospholipid Transport
ABCG1 (ABC8), the human homolog of the Drosophila white gene, is a regulator of macrophage cholesterol and phospholipid transport Jochen Klucken*, Christa Bu¨ chler*, Evelyn Orso´ *, Wolfgang E. Kaminski*, Mustafa Porsch-Ozcu¨ ¨ ru¨ mez*, Gerhard Liebisch*, Michael Kapinsky*, Wendy Diederich*, Wolfgang Drobnik*, Michael Dean†, Rando Allikmets‡, and Gerd Schmitz*§ *Institute for Clinical Chemistry and Laboratory Medicine, University of Regensburg, 93042 Regensburg, Germany; †National Cancer Institute, Laboratory of Genomic Diversity, Frederick, MD 21702-1201; and ‡Departments of Ophthalmology and Pathology, Columbia University, Eye Research Addition, New York, NY 10032 Edited by Jan L. Breslow, The Rockefeller University, New York, NY, and approved November 3, 1999 (received for review June 14, 1999) Excessive uptake of atherogenic lipoproteins such as modified low- lesterol transport. Although several effector molecules have been density lipoprotein complexes by vascular macrophages leads to proposed to participate in macrophage cholesterol efflux (6, 9), foam cell formation, a critical step in atherogenesis. Cholesterol efflux including endogenous apolipoprotein E (10) and the cholesteryl mediated by high-density lipoproteins (HDL) constitutes a protective ester transfer protein (11), the detailed molecular mechanisms mechanism against macrophage lipid overloading. The molecular underlying cholesterol export in these cells have not yet been mechanisms underlying this reverse cholesterol transport process are characterized. currently not fully understood. To identify effector proteins that are Recently, mutations of the ATP-binding cassette (ABC) trans- involved in macrophage lipid uptake and release, we searched for porter ABCA1 gene have been causatively linked to familial HDL genes that are regulated during lipid influx and efflux in human deficiency and Tangier disease (12–14). -

Molecular Characterization and Structural Implications of 25 New ABCB4 Mutations in Progressive Familial Intrahepatic Cholestasis Type 3 (PFIC3)
European Journal of Human Genetics (2007) 15, 1230–1238 & 2007 Nature Publishing Group All rights reserved 1018-4813/07 $30.00 www.nature.com/ejhg ARTICLE Molecular characterization and structural implications of 25 new ABCB4 mutations in progressive familial intrahepatic cholestasis type 3 (PFIC3) Dario Degiorgio1, Carla Colombo2, Manuela Seia1, Luigi Porcaro1, Lucy Costantino1, Laura Zazzeron2, Domenico Bordo3 and Domenico A Coviello*,1 1Laboratorio di Genetica Medica, Fondazione IRCCS, Ospedale Maggiore Policlinico, Mangiagalli e Regina Elena, Milano, Italy; 2Centro Fibrosi Cistica, Universita` degli Studi di Milano, Fondazione IRCCS, Ospedale Maggiore Policlinico, Mangiagalli e Regina Elena, Milano, Italy; 3Bioinformatica e Proteomica Strutturale, Istituto Nazionale per la Ricerca sul Cancro, Genova, Italy Progressive familial intrahepatic cholestasis type 3 (PFIC3) is an autosomal-recessive disorder due to mutations in the ATP-binding cassette, subfamily B, member 4 gene (ABCB4). ABCB4 is the liver-specific membrane transporter of phosphatidylcholine, a major and exclusive component of mammalian bile. The disease is characterized by early onset of cholestasis with high serum c-glutamyltranspeptidase activity, which progresses into cirrhosis and liver failure before adulthood. Presently, about 20 distinct ABCB4 mutations associated to PFIC3 have been described. We report the molecular characterization of 68 PFIC3 index cases enrolled in a multicenter study, which represents the largest cohort of PFIC3 patients screened for ABCB4 mutations to date. We observed 31 mutated ABCB4 alleles in 18 index cases with 29 distinct mutations, 25 of which are novel. Despite the lack of structural information on the ABCB4 protein, the elucidation of the three-dimensional structure of bacterial homolog allows the three-dimensional model of ABCB4 to be built by homology modeling and the position of the mutated amino-acids in the protein tertiary structure to be located. -

5' Untranslated Region Elements Show High Abundance and Great
International Journal of Molecular Sciences Article 0 5 Untranslated Region Elements Show High Abundance and Great Variability in Homologous ABCA Subfamily Genes Pavel Dvorak 1,2,* , Viktor Hlavac 2,3 and Pavel Soucek 2,3 1 Department of Biology, Faculty of Medicine in Pilsen, Charles University, 32300 Pilsen, Czech Republic 2 Biomedical Center, Faculty of Medicine in Pilsen, Charles University, 32300 Pilsen, Czech Republic; [email protected] (V.H.); [email protected] (P.S.) 3 Toxicogenomics Unit, National Institute of Public Health, 100 42 Prague, Czech Republic * Correspondence: [email protected]; Tel.: +420-377593263 Received: 7 October 2020; Accepted: 20 November 2020; Published: 23 November 2020 Abstract: The 12 members of the ABCA subfamily in humans are known for their ability to transport cholesterol and its derivatives, vitamins, and xenobiotics across biomembranes. Several ABCA genes are causatively linked to inborn diseases, and the role in cancer progression and metastasis is studied intensively. The regulation of translation initiation is implicated as the major mechanism in the processes of post-transcriptional modifications determining final protein levels. In the current bioinformatics study, we mapped the features of the 50 untranslated regions (50UTR) known to have the potential to regulate translation, such as the length of 50UTRs, upstream ATG codons, upstream open-reading frames, introns, RNA G-quadruplex-forming sequences, stem loops, and Kozak consensus motifs, in the DNA sequences of all members of the subfamily. Subsequently, the conservation of the features, correlations among them, ribosome profiling data as well as protein levels in normal human tissues were examined. The 50UTRs of ABCA genes contain above-average numbers of upstream ATGs, open-reading frames and introns, as well as conserved ones, and these elements probably play important biological roles in this subfamily, unlike RG4s. -

Translocation of the ABC Transporter ABCD4 from the Endoplasmic
www.nature.com/scientificreports OPEN Translocation of the ABC transporter ABCD4 from the endoplasmic reticulum to Received: 31 December 2015 Accepted: 30 June 2016 lysosomes requires the escort Published: 26 July 2016 protein LMBD1 Kosuke Kawaguchi*, Takumi Okamoto*, Masashi Morita & Tsuneo Imanaka We previously demonstrated that ABCD4 does not localize to peroxisomes but rather, the endoplasmic reticulum (ER), because it lacks the NH2-terminal hydrophilic region required for peroxisomal targeting. It was recently reported that mutations in ABCD4 result in a failure to release vitamin B12 from lysosomes. A similar phenotype is caused by mutations in LMBRD1, which encodes the lysosomal membrane protein LMBD1. These findings suggested to us that ABCD4 translocated from the ER to lysosomes in association with LMBD1. In this report, it is demonstrated that ABCD4 interacts with LMBD1 and then localizes to lysosomes, and this translocation depends on the lysosomal targeting ability of LMBD1. Furthermore, endogenous ABCD4 was localized to both lysosomes and the ER, and its lysosomal localization was disturbed by knockout of LMBRD1. To the best of our knowledge, this is the first report demonstrating that the subcellular localization of the ABC transporter is determined by its association with an adaptor protein. The superfamily of ATP-binding cassette (ABC) transporters comprises membrane-bound proteins that catalyze the ATP-dependent transmembrane transport of a wide variety of substrates1. The human ABC transporter fam- ily currently comprises 49 members classified into seven subfamilies, A to G, based on structural organization and amino acid homology2,3. To date, four ABC proteins have been identified in mammals and classified into “subfamily D”4–7. -

Molecular Structure of a Novel Cholesterol-Responsive a Subclass ABC Transporter, ABCA9
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by University of Regensburg Publication Server BBRC Biochemical and Biophysical Research Communications 295 (2002) 408–416 www.academicpress.com Molecular structure of a novel cholesterol-responsive A subclass ABC transporter, ABCA9 Armin Piehler,1 Wolfgang E. Kaminski,1 Juurgen€ J. Wenzel, Thomas Langmann, and Gerd Schmitz* Institute for Clinical Chemistry and Laboratory Medicine, University of Regensburg, Franz-Josef-Strauß-Allee 11, D-93042, Regensburg, Germany Received 25 May 2002 Abstract We recently identified a novel ABC A subclass transporter, ABCA6, in human macrophages. Here, we report the molecular cloning of an additional ABC A subfamily transporter from macrophages denoted ABCA9. The identified coding sequence is 4.9 kb in size and codes for a 1624 amino acid protein product. In accordance with the proposed nomenclature, the novel transporter was designated ABCA9. The putative full-length ABC transporter polypeptide consists of two transmembrane domains and two nu- cleotide binding folds and thus conforms to the group of full-size ABC transporters. We identified alternative ABCA9 mRNA variants in human macrophages that predict the existence of three truncated forms of the novel transporter. Among the human ABC A subfamily transporters, ABCA9 exhibits the highest amino acid sequence homology with ABCA8 (72%) and ABCA6 (60%), respectively. The striking amino acid sequence similarity between these transporter molecules supports the notion that they represent an evolutionary more recently emerged subgroup within the family of ABC A transporters, which we refer to as ‘‘ABCA6-like transporters.’’ ABCA9 mRNA is ubiquitously expressed with the highest mRNA levels in heart, brain, and fetal tissues. -
ABCB6 Is a Porphyrin Transporter with a Novel Trafficking Signal That Is Conserved in Other ABC Transporters Yu Fukuda University of Tennessee Health Science Center
University of Tennessee Health Science Center UTHSC Digital Commons Theses and Dissertations (ETD) College of Graduate Health Sciences 12-2008 ABCB6 Is a Porphyrin Transporter with a Novel Trafficking Signal That Is Conserved in Other ABC Transporters Yu Fukuda University of Tennessee Health Science Center Follow this and additional works at: https://dc.uthsc.edu/dissertations Part of the Chemicals and Drugs Commons, and the Medical Sciences Commons Recommended Citation Fukuda, Yu , "ABCB6 Is a Porphyrin Transporter with a Novel Trafficking Signal That Is Conserved in Other ABC Transporters" (2008). Theses and Dissertations (ETD). Paper 345. http://dx.doi.org/10.21007/etd.cghs.2008.0100. This Dissertation is brought to you for free and open access by the College of Graduate Health Sciences at UTHSC Digital Commons. It has been accepted for inclusion in Theses and Dissertations (ETD) by an authorized administrator of UTHSC Digital Commons. For more information, please contact [email protected]. ABCB6 Is a Porphyrin Transporter with a Novel Trafficking Signal That Is Conserved in Other ABC Transporters Document Type Dissertation Degree Name Doctor of Philosophy (PhD) Program Interdisciplinary Program Research Advisor John D. Schuetz, Ph.D. Committee Linda Hendershot, Ph.D. James I. Morgan, Ph.D. Anjaparavanda P. Naren, Ph.D. Jie Zheng, Ph.D. DOI 10.21007/etd.cghs.2008.0100 This dissertation is available at UTHSC Digital Commons: https://dc.uthsc.edu/dissertations/345 ABCB6 IS A PORPHYRIN TRANSPORTER WITH A NOVEL TRAFFICKING SIGNAL THAT -

Functional Rescue of Misfolding ABCA3 Mutations by Small Molecular Correctors Susanna Kinting, Stefanie Ho¨ Ppner, Ulrike Schindlbeck, Maria E
Human Molecular Genetics, 2018, Vol. 27, No. 6 943–953 doi: 10.1093/hmg/ddy011 Advance Access Publication Date: 9 January 2018 Original Article ORIGINAL ARTICLE Functional rescue of misfolding ABCA3 mutations by small molecular correctors Susanna Kinting, Stefanie Ho¨ ppner, Ulrike Schindlbeck, Maria E. Forstner, Jacqueline Harfst, Thomas Wittmann and Matthias Griese* Department of Pediatric Pneumology, Dr. von Hauner Children’s Hospital, Ludwig-Maximilians University, German Centre for Lung Research (DZL), 80337 Munich, Germany *To whom correspondence should be addressed at: Department of Pediatric Pneumology, Dr. von Hauner Children’s Hospital, Ludwig-Maximilians University, German Centre for Lung Research (DZL), Lindwurmstraße 4, 80337 Munich, Germany. Tel: þ49 89 440057870; Fax: þ49 89 440057872; Email: [email protected] Abstract Adenosine triphosphate (ATP)-binding cassette subfamily A member 3 (ABCA3), a phospholipid transporter in lung lamellar bodies (LBs), is essential for the assembly of pulmonary surfactant and LB biogenesis. Mutations in the ABCA3 gene are an important genetic cause for respiratory distress syndrome in neonates and interstitial lung disease in children and adults, for which there is currently no cure. The aim of this study was to prove that disease causing misfolding ABCA3 mutations can be corrected in vitro and to investigate available options for correction. We stably expressed hemagglutinin (HA)-tagged wild-type ABCA3 or variants p.Q215K, p.M760R, p.A1046E, p.K1388N or p.G1421R in A549 cells and assessed correction by quantitation of ABCA3 processing products, their intracellular localization, resembling LB morphological integrity and analysis of functional transport activity. We showed that all mutant proteins except for M760R ABCA3 were rescued by the bithiazole correctors C13 and C17. -

Blueprint Genetics ABCC11 Single Gene Test
ABCC11 single gene test Test code: S02680 Phenotype information Apocrine gland secretion, variation in Alternative gene names MRP8 Test Strengths The strengths of this test include: CAP accredited laboratory CLIA-certified personnel performing clinical testing in a CLIA-certified laboratory Powerful sequencing technologies, advanced target enrichment methods and precision bioinformatics pipelines ensure superior analytical performance Careful construction of clinically effective and scientifically justified gene panels Our Nucleus online portal providing transparent and easy access to quality and performance data at the patient level Our publicly available analytic validation demonstrating complete details of test performance ~2,000 non-coding disease causing variants in our clinical grade NGS assay for panels (please see ‘Non-coding disease causing variants covered by this test’) Our rigorous variant classification scheme Our systematic clinical interpretation workflow using proprietary software enabling accurate and traceable processing of NGS data Our comprehensive clinical statements Test Limitations This test does not detect the following: Complex inversions Gene conversions Balanced translocations Mitochondrial DNA variants Repeat expansion disorders unless specifically mentioned Non-coding variants deeper than ±20 base pairs from exon-intron boundary unless otherwise indicated (please see above non-coding variants covered by the test). This test may not reliably detect the following: Low level mosaicism (variant with a minor allele fraction of 14.6% is detected with 90% probability) Stretches of mononucleotide repeats Indels larger than 50bp Single exon deletions or duplications Variants within pseudogene regions/duplicated segments The sensitivity of this test may be reduced if DNA is extracted by a laboratory other than Blueprint Genetics. For additional information, please refer to the Test performance section and see our Analytic Validation.