Impacts of the Stimulate, Appreciate, Learn, and Transfer Community Engagement Approach to Increase Immunisation Coverage in Assam, India
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Oih Government of India Ministry of Environment, Forest and Climate Change
OIH GOVERNMENT OF INDIA MINISTRY OF ENVIRONMENT, FOREST AND CLIMATE CHANGE LOK SABHA UNSTARRED QUESTION No. 1871 TO BE ANSWERED ON 29.11.2019 Reserve Forests in Assam 1871. SHRI NABA KUMAR SARANIA: Will the Minister of ENVIRONMENT, FOREST AND CLIMATE CHANGE be pleased to state: (a) the details of the total forest land and such land falling in the sixth schedule area and also those declared as reserve forest land in the State of Assam; (b) whether lease has been granted by the Government to the villages located in the forest land of Assam including Lungsung area of Kokrajhar of BTC and if so, the details thereof; (c) the details of the number of villages in Assam from where people have been evicted including those located in Nonai forest in Udalgiri district; (d) whether the people living in the forests receive the benefits of Government schemes; and (e) if so, the details thereof, scheme-wise and village name-wise and if not, the reasons therefor? ANSWER MINISTER OF STATE IN THE MINISTRY OF ENVIRONMENT, FOREST AND CLIMATE CHANGE (SHRI BABUL SUPRIYO) (a) As per India State of Forest Report (ISFR) 2017, area of total Recorded Forest in the State of Assam is 2683200 ha and total Forest Cover constitutes an area of 2810500 ha in the State of Assam, which is 35.83% of the State’s geographical area. As informed by Government of Assam, there are 312 declared Reserved Forests covering a total forest area of 1359026.70 ha in the State of Assam. Out of which 56 no. -

Tezpur Building Division
Thecom Statement showing the flagship programs currently operational and some of completed works under P.W.D., Tezpur Building Division : Tezpur *Name of work :- Construction of Girls' Hostel at Pavoi High School in Biswanath District (Gr. No. - 49). *Year of sanction : 2012 *Sanction Amount : Rs. 155.35 (L) *Physical progress : - 100% *Financial progress :- Rs. 12005173.00 *Name of work :- Construction of Additional Class Room 1 (One) No. under Multi Sectoral Development Programme (MSDP) in Biswanath District for the year 2015-16 at :- Golia Gerenta LPS *Year of sanction : 2015-16 *Sanction Amount : 4.80 L *Physical progress : - 100% *Financial progress :- Rs. 213840.00 *Name of work :- Improvement of Public facilities including Public Toilet in SDO (C) Office premises at Biswanath Chariali. *Year of sanction : 2017 * Sanction Amount : Rs. 1744500.00 *Physical progress : - 100% *Financial progress :- Nil *Name of work :- Construction of Barrack for Security Personnel at Judicial Officers Qtrs. at Biswanath Chariali. *Year of sanction : 2017-18 * sanction Amount : Rs.1366500.00 *Physical progress : - 100% *Financial progress :- Rs. 1352342.00 *Name of work :- Construction of Girls' Hostel at Janata H.S. School campus under Bihali Block in Sonitpur District. (Gr. No. - 47) *Year of sanction : 2012 * Sanction Amount : Rs. 155.35 (L) *Physical progress : - 100% *Financial progress :- Rs. 9237826.00 *Name of work :- Construction of Garage for Mobile Kit Van received from Govt. of India in the office of the Inspector of Legal Metrology, Biswanath Chariali during the financial year 2016-17 under Plan scheme. *Year of sanction : 2016-17 * Sanction Amount : 4.452 L *Physical progress : - 100% *Financial progress :-Rs. -

Assam, ICTC July-2010.Pdf
Name of the ICTC Name of the Incharge / Medical S. No Name & Address of the ICTC District Counsellor Contact No Officer Contact No Barpeta Civil Hospital ICTC(G), Barpeta District PIN- 1 781301 Barpeta Bipul Barman 98643-97708 Dr.D.Ramchiary 94351-23881 Barpeta Civil Hospital ICTC(PPTCT), barpeta District 2 PIN- 781301 Barpeta Dolly Barman 98544-03032 Dr. T. Pathak 94350-24998 3 Barpeta Rd FRU, Barpeta District PIN -781315 Barpeta Baby Deka 97070-16371 Dr. Narayan Das 94351-23788 4 Pathsala CHC,Barpeta District PIN-781325 Barpeta Sonali Devi 94351-24228 Dr. R. K. Deka 94351-24228 5 Tamulpur CHC,Barpeta District PIN-781367 Baksa Mahesh Sarma 94359-75133 Dr. P. Sarma 97077-27394 Bongaigaon Civil Hospital ICTC(G) , Bongaigoan 6 District, PIN 783380 Bongaigoan Sahidul Islam 94353-12112 Dr.S.N.Das 94353-11561 Bongaigaon Civil Hospital ICTC(PPTCT) , 7 Bongaigoan District, PIN-783380 Bongaigoan Kritanjali Das 94353-02013 Dr. S. Baruah 94350-22594 8 Abhayapuri CHC, Bongaigoan District, PIN-783384 Bongaigoan Rinku Sarma 98642-93724 Dr. M.K.Kakaty 94350-22778 Anup Kr. Silchar Medical College Hospital ICTC(G), Cachar Dutta,Deepanwita 94352-31254,94353- 9 District PIN-788014 Cachar Bhowmik 73829 Dr. Silpi Rani Barman 94350-71289 Silchar Medical College Hospital 10 ICTC(PPTCT)Cachar District PIN-788014 Cachar Radha Rani Das 94358-08408 Dr. Pronoy Nath 94350-70133 11 Kalain CHC,Cachar District PIN-788812 Cachar Biplob Das 94356-81425 Dr. Badal Das 94356-81425 Mangaldoi Civil Hospital ICTC(G), DarrangDistrict 12 PIN-784125 Darrang Deepak Saikia 94010-58128 Dr. J.K. Sarma 94350-87342 Mangaldoi Civil Hospital ICTC(PPTCT), Darrang 13 District PIN-784125 Darrang Debajani Deka 98641-41779 Dr. -

Ground Water Information Booklet Baksa District, Assam
Technical Report Series: D No: Ground Water Information Booklet Baksa District, Assam Central Ground Water Board North Eastern Region Ministry of Water Resources Guwahati November 2013 GROUND WATER INFORMATION BOOKLET BAKSA DISTRICT, ASSAM DISTRICT AT A GLANCE Sl. ITEMS STATISTICS No. 1. GENERAL INFORMATION i) Geographical Area (sq.km.) 2,007.50 ii) Population (as per 2011 Census) 9,53,773 iii) Average Annual Rainfall (mm) 2,971.6 2. GEOMORPHOLOGY i) Major Physiographic Units Flood plain & alluvial terrace, swamp. ii) Major Drainages Mara Manas, Palla, Po-Mara, Kaldia, Tihu, Mora Pagladia, Burhadia, Pagladia, Nona, Baralia and Puthimari River. 3. LAND USE (sq. km.) i) Forest Area 830.19 ii) Net Area Sown 660.85 iii) Total cropped area 1276.19 iv) Area sown more than once 615.34 4. MAJOR SOIL TYPES Newer alluvium, older alluvium, loamy & lateritic soil. 5. AREA UNDER PRINCIPAL CROPS Not Available (sq.km.) 6. IRRIGATION BY DIFFERENT SOURCES 65.85 (sq.km.) 7. NUMBERS OF GROUND WATER 1 MONITORING STATIONS OF CGWB (as on March 2013) 8. PREDOMINANT GEOLOGICAL Alluvial formation FORMATIONS 9. HYDROGEOLOGY i) Major water Bearing Formations Alluvial sediments of Quaternary age . ii) Long term Water Level Trend in 20 Rise/Fall during Pre-monsoon (0.005/ yrs (1989 –2008) in m/yr 0.038) m/yr, Rise/Fall during Post- monsoon (0.014-0.43/ 0.00-0.00) m/yr. 10. GROUND WATER EXPLORATION BY CGWB (as on 28.02.2013) i) No of Wells Drilled 1 Exploratory Well & 1 Slim Hole ii) Depth Range (m) 72-159.9 iii) Discharge (m3/hr) 16.32 with drawdown of 0.43 m iv) Transmissivity (m2/day) 958.0 11. -

Heavy Floods in Assam Have Affected All the 27 Districts of the State
SITUATION REPORT - ASSAM FLOODS NATURE OF HAZARD : FLOODS DATE: 03.08.04 at 9.30 AM Heavy floods in Assam have affected all the 27 districts of the state. These districts are Tinsukia, Dibrugarh, Shivsagar, Jorhat, Golaghat, Nagoan, Morigaon, Kamrup, Kamrup Metro, Darrang, Sonitpur, Dhemaji, Lakhimpur, Nalbari, Berpetta, Bongaigaon, Kokrajhar, Goalpara, Dhubri, Chirang, Karbi Anglong, Karimganj, Hailakhandi, Cachar, Udalguri, North Cachar Hills and Baska. Heavy rainfall over the state and in neighboring uphill states and countries for a sustained period since the last week of June has resulted in the rise of water level in the whole river network – Brahmaputra and it’s tributaries in the state. Large no. of villages got submerged with the overflowing of these rivers.The worst affected districts during the current flood are Barpeta, Cachar, Dhemaji, Dhubari, Goalpara, Kamrup ( rural), Morigaon, Nagaon, Nalbari, Sonitpur, Udalguri. The rise in the water level, breaches along the river & dam embankments, release of water from upper catchment areas (Bhutan), landslides and sudden change of course by rivers, aggravated and deteriorated overall flood situation of the state. The flood has also caused widespread damages to human life, property, standing crops, flood control embankments, tea gardens and other basic infrastructure in the state. Most of the wild life sanctuaries - Kaziranga National Park, National Parks of Manas, Orang and Dibru-Saikhowa, and Wild Life Sanctuaries Burha Chapori, Pobitora, Laokhowa and Bornodi were affected under the grip of the flood. CURRENT SITUATION : Overall flood situation of the state is improving with the receding of the rivers and less rainfall over the state and adjoining areas in the past few days and there has been no fresh damages reported except the increase in the death toll. -

LIST of the DESIGNATED Apios, Pios and APPELLATE AUTHORITIES of ASSAM POLICE UNDER RIGHT to INFORMATION ACT, 2005
LIST OF THE DESIGNATED APIOs, PIOs AND APPELLATE AUTHORITIES OF ASSAM POLICE UNDER RIGHT TO INFORMATION ACT, 2005 Name of the Public APIOs PIOs Appellate Authorities Authority Assam Police Asstt. Inspector General Inspector General of Police(A), Director General of Police, Assam Headquarters, Ulubari, of Police(A), Assam, Assam, Guwahati Phone- 0361-2450555/ 2455126 Guwahati. Guwahati Phone- 0361-2526189 E-mail: [email protected] Phone-0361-2521703 Deputy Inspector General of Police(Western Range) Dhubri District 1.Dy.SP(HQ), Dhubri SP, Dhubri DIGP(WR), Assam, Bongaigaon 2. SDPO, South Salmara Phone- 03662-230014 Phone- 03664- 237888 3.SDPO, Bilasipara e-mail- [email protected] Kokrajhar District 1.Dy.SP(HQ), Kokrajhar SP, Kokrajhar -do- 2.SDPO, Gossaigaon Phone- 03661-270725 3.SDPO, Parbhatjora Chirang District 1.Dy.SP(HQ), Chirang SP, Chirang -do- 2.SDPO, Bijni Phone- 03664-243189 Bongaigaon District Dy.SP(HQ), Bongaigaon SP, Bongaigaon -do- Phone- 03664-230898 Goalpara District Dy.SP(HQ), Goalpara SP, Goalpara -do- Phone-03663- 240161 Barpeta District 1.Dy.SP(HQ), Barpeta SP, Barpeta -do- 2.SDPO, Bajali Phone- 03665-236254 7th A.P.Bn., Kokrajhar Adjt 7th APBn CO 7th APBn, Charaikhola, DIGP(AP), Assam, Guwahati Kokrajhar. Phone-03661-270213 Phone- 0361-2452891 e-mail- [email protected] 8th APBn, Bongaigaon Adjt 8th APBn CO 8th APBn, Abhayapuri, -do- Bongaigaon. Phone- 03664- 281446 20th A.P.(I.R.) Bn, Dhubri Adjt 20th AP(IR) Bn. CO 20th AP (IR) Bn, Panbari, -do- Dhubri. Phone- 03662-239187 24th AP(IR) Bn, Chirang Adjt 24th AP(IR) Bn CO 24th AP(IR) Bn., Chirang -do- 1st APTF Bn., Goalpara Adjt. -

Assessing the Tropical Forest Cover Change in Northern Parts of Sonitpur
www.nature.com/scientificreports OPEN Assessing the tropical forest cover change in northern parts of Sonitpur and Udalguri District of Assam, India Ranjit Mahato1, Gibji Nimasow1*, Oyi Dai Nimasow2 & Dhoni Bushi1 Sonitpur and Udalguri district of Assam possess rich tropical forests with equally important faunal species. The Nameri National Park, Sonai-Rupai Wildlife Sanctuary, and other Reserved Forests are areas of attraction for tourists and wildlife lovers. However, these protected areas are reportedly facing the problem of encroachment and large-scale deforestation. Therefore, this study attempts to estimate the forest cover change in the area through integrating the remotely sensed data of 1990, 2000, 2010, and 2020 with the Geographic Information System. The Maximum Likelihood algorithm- based supervised classifcation shows acceptable agreement between the classifed image and the ground truth data with an overall accuracy of about 96% and a Kappa coefcient of 0.95. The results reveal a forest cover loss of 7.47% from 1990 to 2000 and 7.11% from 2000 to 2010. However, there was a slight gain of 2.34% in forest cover from 2010 to 2020. The net change of forest to non-forest was 195.17 km2 in the last forty years. The forest transition map shows a declining trend of forest remained forest till 2010 and a slight increase after that. There was a considerable decline in the forest to non-forest (11.94% to 3.50%) from 2000–2010 to 2010–2020. Further, a perceptible gain was also observed in the non-forest to the forest during the last four decades. -
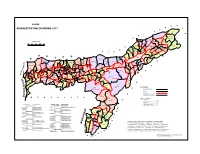
ADMINISTRATIVE DIVISIONS 2011 a R Sadiya
ASSAM D E S ADMINISTRATIVE DIVISIONS 2011 A R Sadiya P H ! ! L A Jonai TINSUKIA H Doom Dooma Sissibargaon ! Subansiri (Pt - II) KILOMETRES ! Dibrugarh Chabua P Gogamukh P East ! C Dhemaji P Tinsukia 10 0 10 20 30 ! DHEMAJI DIBRUGARH ! ! ! Tengakhat Margherita Kadam Dhakuakhana Dibrugarh A (Pt -II) W e s t ! ! Subansiri (Pt - I) ! ! P ! Moran Naharkatiya Naobaicha N North Dhakuakhana Tingkhong Lakhimpur !(Pt-I) ! A U ! ! R Dimow ! LAKHIMPUR Mahmora ! Sonari Bihpuria Sivasagar ! ! H P SIVASAGAR U Narayanpur Majuli A N Gohpur T Chariduar ! Amguri ! ! ! B ! ! ! Udalguri Helem Jorhat East Nazira Bengtal Jalah Dhekiajuli (Pt) SONITPUR Biswanath ! Baksa ! Harisinga ! P D L Barnagar (Pt) (Pt) P Tamulpur P Mazbat ! ! Jorhat West Teok ! UDALGURI A Sarupeta ! BAKSA ! Na-Duar ! CHIRANG JORHAT Kokrajhar 2 (Pt) Baganpara Kalaigaon (Pt) Dergaon G Gossaigaon (Pt) (Pt) (Pt) 3 4 Bokakhat (Sidli (Pt)) Khoirabari (Pt) (Tezpur) ! ! ! N N Barama 2 Goreswar (Pt) Bijni (Pt) ! Jalah ! Khumtai ! 3 ! (Pt) ! ! ! Titabor Mariani E ! 3 2 ! ! P ! ! Dotoma P Barnagar (Pt) Bajali Ghograpar (Pt) 1 Khoirabari (Pt) Tihu(Pt)Banekuchi 4 ! Dalgaon (Pt) Kaliabor B P Bijni (Pt) ! S a r u peta (Pt) ! 1 ! 1 1 2 ! KOKRAJHAR P 1 (Pt) ! Pathorighat (Pt) GOLAGHAT ! Bongaigaon ! Tihu P Rupahi (Pt) ! Nalbari Rangia 1 (Mangaldoi (Pt)) ! Silonijan T (Pt) BARPETA ! Dhing ! Morangi A Bhowraguri Chapar 1 NALBARI ! (Pt) Laharighat ! S Gossaigaon (Pt) ! Barpeta Sarthebari ! ! ! Golaghat (Pt) BONGAIGAON ! Pachim Koya P Samaguri E ! Nalbari Barbhag ! P P I ! Bilasipara Chapar N DARRDANG Bhuragaon -

Executive Summary
PLP 2016-17 Baksa District EXECUTIVE SUMMARY 1.i. Theme of PLP 2015-16 and Sectoral Projections for the year 2016-17 The criticality of capital formation ‘in’ and ‘for’ agriculture need not be overemphasized. However, the recent declining trend in investment credit vis-à-vis crop loan has serious implications for sustaining capital formation. The theme for the PLP 2016-17 is ‘Accelerating the pace of capital formation in agriculture and allied sector’. The PLP maps the potential in priority sectors which could be exploited with institutional credit within a specified time frame. PLPs are intended to provide a meaningful direction to the flow of credit to different sectors at the ground level taking into account all relevant factors. The various linkages and other support services required to be provided by line departments to facilitate credit flow as planned are also listed in the PLP. Baksa District is a newly re-organised district under Bodoland Territorial Council of Assam carved out from three districts viz Nalbari, Barpeta and Kamrup. It is located between 90º.8´ E to 91º.8´ E longitude and 26º.35´N to 26º.83´N latitude on North-West side of Assam. The district is surrounded by Chirang district in the West, Barpeta, Nalbari & Kamrup districts in the South, Udalguri district in the East and Bhutan on the North. The District head quarter is located at Mushalpur. The district is divided into 3 sub-divisions viz. Mushalpur, Tamulpur & Salbari. There are 8 development Blocks in the district with 690 inhabited villages. The total geographical area of the district is spread over 2346 Sq. -

Ethno-Medicinal Use of Weed Flora in Dibrugarh, Assam, Ne India. Suman Gogoi Department of Botany, DHSK College, Dibrugarh, Assam
International Journal of Disaster Recovery and Business Continuity Vol.11, No. 3, (2020), pp. 2702–2706 Ethno-Medicinal Use Of Weed Flora In Dibrugarh, Assam, Ne India. Suman Gogoi Department of botany, DHSK College, Dibrugarh, Assam. Abstract The present study was conducted in the city Dibrugarh, Assam in order to document the ethno-medicinal use of weed flora in different regions of the city. Data was collected through observation and interview with the local people during the year 2020. In this investigation 48 species of weed flora belonging to 28 families were found to be utilized in the treatment of certain diseases and health conditions. Keywords Ethno-medicinal, Weed, Diseases. Introduction Weeds are the plants that grow in an uncontrolled manner and at places where they are unwanted. These plant species have no economic value and are rarely utilized. They cause inconvenience by growing in different surfaces like agricultural land, flower gardens, house hold gardens and road sides etc. These weeds however are seen to find a place in the traditional medicine systems where they are used as cure for different diseases. Ethno-medicine or the traditional practice of medicine among the different ethnic groups in a region utilizes plant and animal compounds for the treatment of a particular disease. Since time immemorial, mankind has utilized plants for the treatment of various diseases. Today, with the easy availability of modern therapeutic medicine such plant based medicine are rarely used. However in the elderly people in villages and rural areas people are still found to utilize these plant based medicine for treatment of diseases. -
A Study of Human Development in Bodoland Territorial Area Districts (BTAD), Assam
INTERNATIONAL JOURNAL OF SCIENTIFIC & TECHNOLOGY RESEARCH VOLUME 9, ISSUE 04, APRIL 2020 ISSN 2277-8616 A Study Of Human Development In Bodoland Territorial Area Districts (BTAD), Assam Priyambee Swargiary Abstract: In the year 1990, United Nations Development Programme [UNDP] introduced a more comprehensive way of measuring human development, i.e. Human Development Index. HDI is a statistical tool used to measure a country’s overall achievement in its s ocial and economic dimensions. Both social and economic dimensions are based on education, health and standard of living. This index has become an alternative to the traditional unidimensional measure of development. HDI plays an important role to broaden the prospect of progress. HDI is an attempt to reflect the certain characteristics such as people’s choices, capabilities, and well being etc. The main objective of the paper is to analyse the key dimension of human development i.e. education, health and standard of living of the pe ople of BTAD. Its empirical evidence has proved to be very meaningful to the Governments all over the world as well as the UN agencies. Index Terms: Development, Human Development Index, Capabilities, Well Being, Standard of Living, Health, Education etc. ———————————————————— 1 INTRODUCTION Bodoland Territorial Council is one of the largest autonomous Area, Population, Town, Block and Villages of BTAD: council in Assam comprising of four districts viz. Kokrajhar, District Area in Population Town Block No. of Chirang, Baksa, and Udalguri. Under the sixth schedule of the sq.km Villages Indian Constitution BTC was formed on 10th February 2003. Kokrajhar 3296 887142 4 11 1068 The autonomous council was carved out of the seven existing Chirang 1923 482162 3 5 508 Baksa 2457 950075 2 10 690 districts viz. -
No. BTC-LR-220-2014-16 (9 January)
Û?œˆ¬≈Mê√ Ú•§1 - 768 ˚97 Registered No.-768/97 ’¸˜ 1±Ê√¬ÛS THE ASSAM GAZETTE ’¸±Ò±1Ì EXTRAORDINARY õ∂±5 fl¡M‘√√«Q1 ¡Z±1± õ∂fl¡±ø˙Ó¬ PUBLISHED BY THE AUTHORITY Ú— 603 ø√˙¬Û≈¬1, qSê¬ı±1, 27 ’À"√√±¬ı1, 2017, 5 fl¡±øÓ¬, 1939 (˙fl¡) No. 603 Dispur, Friday, 27th October, 2017, 5th Kartika, 1939 (S.E.) GOVERNMENT OF ASSAM ORDERS BY THE GOVERNOR BODOLAND TERRITORIAL COUNCIL SECRETARIAT ::: BODOFA NWGUR, KOKRAJHAR LAND REVENUE AND DIASTER MANAGEMENT DEPARTMENT NOTIFICATIONS The 9th January, 2017 No. BTC/LR-220/2014/16.- The Bodoland Territorial Council, Kokrajhar is pleased to Re-organize the existing Orang & Udalguri mouza of Mazbat & Udalguri Revenue Circle in the district of Udalguri and create one new mouza from existing Orang & Udalguri mouza known as Mazbat mouza in the interest of public service and administrative convenience from the date of its functioning. The Jurisdiction of Mazbat mouza is comprising with the following 85 Nos. of Revenue villages of existing Orang mouza of Mazbat Revenue Circle and 22 Nos. Revenue villages of existing Udalguri mouza of Udalguri Revenue Circle of Udalguri District which has been transferred to Mazbat Revenue Circle due to Re-organization of Revenue Circles as a consequence of creation of BTAD. The Re-organize Mazbat mouza comprising the following Revenue villages :- 1 No.2 Bahipukhuri TE 22 Bagulamari 43 No.1 Garogaon 64 pub-Kuruabahi 2 Lamabari TE 23 Bamuniagaon 44 No.1 Mazbat TE 65 Rowtamukh 3 No.1 Pathakpur 24 Pachnaikhuti 45 No.3 Naharbari 66 No.1 Merabil 4 No.2 Pathakpur 25 Dewalkhanda 46 Chutia Basti