Assisting the Somali Population
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Energy Situation in the Dadaab Refugee Camps, Kenya the Energy Situation in the Dadaab Refugee Camps, Kenya
Research Paper Edited by Stephen Okello (GVEP International) Energy, Environment and Resources Department | May 2016 The Energy Situation in the Dadaab Refugee Camps, Kenya The Energy Situation in the Dadaab Refugee Camps, Kenya Preface The Moving Energy Initiative (MEI) is a collaboration between GVEP International, Chatham House, the Office of the United Nations High Commissioner for Refugees (UNHCR), the Norwegian Refugee Council (NRC) and Practical Action Consulting. The MEI seeks to identify how innovation in policy and practice within the humanitarian sector can improve access to sustainable energy among displaced populations and camp operators. Funded by the United Kingdom’s Department for International Development (DFID), the initiative seeks to develop, research and test appropriate sustainable energy solutions, as well as innovative delivery models for energy solutions. As part of initial research intended to inform subsequent phases of the project, the MEI carried out an energy survey in 2015 in the Dadaab refugee camps in Kenya. This paper has been written by GVEP International, with copy-editing and production support from Chatham House. Its purpose is to present the results from the 2015 field study. The paper is a summary of the survey report – the whole report can be obtained on request from GVEP International ([email protected]). 1 | Moving Energy Initiative The Energy Situation in the Dadaab Refugee Camps, Kenya Field Survey Background information The Dadaab refugee camps are located in Garissa County, in northeastern Kenya. The complex consists of five sub-camps, and covers an area of 50 square kilometres. As of March 2015, the Dadaab area was the fourth-largest population centre in Kenya, with a total refugee population of 351, 538. -

Dadaab, Kenya APRIL 2019
OPERATIONAL UPDATE Dadaab, Kenya APRIL 2019 The first camp in Dadaab was Kambioos refugee camp was Since December 2014, Somali established in 1991. There are 3 closed on 31st March 2017 and refugees who decide to camps in Dadaab: Hagadera, Ifo2 refugee camp was closed on voluntarily return to their home Dagahaley and Ifo. 31st May 2018. country, receive UNHCR support in Kenya and Somalia. VOLUNTARY REPATRIATION FROM DADAAB FUNDING (AS AT 16 APRIL 2019) 79,670 USD 170.1 M Somali refugees have returned home since December 2014 requested for the Kenya situation 57% Funds received 15% Percentage of Dadaab population are children 211,086 Total Dadaab population as at 30 April 2019 63,138 Unfunded 85% Refugee children are enrolled in school in Dadaab camps POPULATION OF CONCERN AS AT 30 APRIL 2019 Country of Origin Somalia 203,324 Ethiopia 6,509 South Sudan 960 DR Congo 90 Burundi 78 Uganda 68 Sudan 36 Rwanda 11 Eritrea 4 Other 6 TOTAL: 211,086 www.unhcr.org 1 MONTHLY OPERATIONAL UPDATE Dadaab, Kenya / APRIL 2019 Voluntary Repatriation ■ During the month of April, five voluntary repatriation flights were organized to help return 344 individuals to Kismayo (287) and Mogadishu (57). ■ As at 30th April 2019, a total 79,670 refugees were facilitated to voluntarily go back to Somalia, from Dadaab refugee operations since the beginning of the process in 2014. ■ Facilitation of road movement remains suspended due to military operations en route to Kismayu, Baidoa and other major return areas. However, flight options remain open to refugees willing to return to Mogadishu, Kismayu and Baidoa. -

Update on the Somali Refugee Emergency and Protracted Refugee Situation in Dadaab, Kenya
Side Event to the 60th Session of the Executive Committee UNHCR/E Hockstein Update on the Somali Refugee Emergency and Protracted Refugee Situation in Dadaab, Kenya Briefing by Ms. Liz Ahua, UNHCR Representative in Kenya Mr. Guillermo Bettochi, UNHCR Representative for Somalia Tuesday, 29 September 09:00-10:00 Palais des Nations, Room XXIII BACKGROUND NOTE “Update on the Somali Refugee Emergency and Protracted Refugee Situation in Dadaab, Kenya” Since 2008, there has been a dramatic increase in the forced displacement of Somalis. Over 120,000 persons have entered Kenya as refugees in this period. In 2009 alone, over 50,000 new Somali refugees have arrived in Dadaab, a constellation of three camps in Kenya established in 1991. Dadaab was originally meant to accommodate a maximum of 90,000 refugees but is now teeming with more than three times that number. The influx continues at a monthly average of some 5,000 persons. Dadaab represents today both a protracted refugee situation and one of the most acute emergencies in the world. Extreme overcrowding and congestion characterize the crisis that is unfolding in the camps, with no space to establish or expand shelter, and sanitation, health and education facilities. The semi-arid conditions, limited resources and general poverty affecting the local host population, have compounded the situation. UNHCR and its partners have endeavoured to mount a determined emergency response. In August 2009, during his second visit to the country in a year, the High Commissioner proposed to the Government a five-prong strategy, which reiterated the call for the allocation by the authorities of land for the establishment of a fourth camp as pivotal for an effective response. -

DGMQ's Africa Field Program in Kenya
DGMQ’s Africa Field Program in Kenya CDC’s Division of Global Migration and Quarantine (DGMQ), assisted by the Division of Global Health Protection, sponsors the Africa Field Program, administered from CDC’s Kenya office, which is dedicated to the improvement and promotion of health for refugees and immigrants. The DGMQ Africa Field Program’s major partners in this effort are the Kenya Medical Research Institute, International Organization for Migration, and UN High Commissioner for Refugees. Refugees in Africa y 2.7 million people with refugee or “refugee- like” status in Africa at the end of 2011 y 770,000 refugees in Kenya y 376,000 refugees in Ethiopia Core Activities y Coordinates activities to protect the health of refugees who resettle to the US y Conducts disease surveillance y Provides technical training and support y Builds capacity for healthcare partners y Strengthens international partnerships Women carrying water in Dadaab Refugee Camp. y Responds to outbreaks in Africa Dadaab and Kakuma Refugee Camps Role in Resettling African Refugees to Not far from the Somali border of Kenya lies the town the United States of Dadaab, home to over 450,000 refugees in what is Over the past 10 years, between 8,000 and 30,000 African the largest refugee camp in the world. The Kakuma refugees have resettled to the United States annually. To camp is closer to the border with Sudan, and has prevent infectious threats from entering the United States over 120,000 refugees. Refugees at both camps are and to promote refugee health, DGMQ faced with a host of medical problems which are compounded by the overcrowded conditions and y Develops guidelines to help physicians conduct medical limited access to care. -

Dadaab Returnee Conflict Assessment August 2017
DADAAB RETURNEE CONFLICT ASSESSMENT AUGUST 2017 PREPARED FOR DANISH DEMINING GROUP (DDG) BY KEN MENKHAUS Dadaab Returnee Conflict Assessment | i Foreword and Acknowledgements This conflict assessment was implemented as part of the UK Department for International Development (DFID) funded and Norwegian Refugee Council (NRC) and Danish Refugee Council (DRC) implemented project: ‘Promoting Durable Solutions through Integrated Return, Reintegration and Resilience Support to Somali Displacement affected Populations’. The project aims to support conditions conducive for safe and dignified return and sustainable reintegration of Somali refugees. The project was implemented between October 2016 and June 2017. The Conflict Assessment was implemented by the Danish Demining Group (DDG), under the supervision of Mads Frilander. The principal investigator and author of the study is Ken Menkhaus, and he alone is responsible for any errors or misinterpretations in the report. He and Ismahan Adawe formed the research team that conducted fieldwork for this study in Mogadishu, Kismayo, Baidoa, and Nairobi in December 2016 and January 2017. The analysis combines existing studies and reports collected in a literature review with over 60 field interviews, as well as a survey carried out in Kismayo. The interviews were semi-structured in format, some held with key informants and others with focus groups of men and women representing host communities, internally displaced persons (IDPs), and returnees. The survey was carried out by the company Researchcare Africa. The research was conducted in challenging security and political conditions, and the research team is deeply indebted to many individuals and organisations who provided essential help to overcome those obstacles. We are also very grateful to the hundreds of Somali stakeholders and international aid officials who volunteered their time to meet with the research team and discuss these issues. -

Dadaab, Kenya JULY 2019
OPERATIONAL UPDATE Dadaab, Kenya JULY 2019 The first camp in Dadaab was Kambioos refugee camp was Since December 2014, Somali established in 1991. There are 3 closed on 31st March 2017 and refugees who decide to camps in Dadaab: Hagadera, Ifo2 refugee camp was closed on voluntarily return to their home Dagahaley and Ifo. 31st May 2018. Both were country, receive UNHCR officially handed over to the support in Kenya and Somalia. Government on 21st June 2019. VOLUNTARY REPATRIATION FROM DADAAB FUNDING (AS AT 30 JULY 2019) 80,498 USD 170.1 M Somali refugees have returned home since December 2014 requested for the Kenya situation 57% Funds received 31% Percentage of Dadaab population are children 211,591 Total Dadaab population as at 31 July 2019 62,610 Unfunded 69% Refugee children are enrolled in school in Dadaab camps POPULATION OF CONCERN AS AT 31 JULY 2019 Country of Origin Somalia 203,851 Ethiopia 6,516 South Sudan 941 DR Congo 85 Burundi 79 Uganda 68 Sudan 33 Rwanda 11 Eritrea 4 Other 3 TOTAL: 211,591 www.unhcr.org 1 MONTHLY OPERATIONAL UPDATE Dadaab, Kenya / JULY 2019 Voluntary Repatriation ■ As at 31st July 2019, a total 80,498 refugees were facilitated to voluntarily go back to Somalia, from Dadaab refugee operations since the beginning of the process in December 2014. ■ During the month of July, 3 voluntary repatriation flights were organized to help return 136 individuals from 36 households, to Somalia. Majority (90) individuals returned to Baidoa while 46 returned to Mogadishu. ■ All return movements, both flights and road convoy to Kismayo, were suspended on the 13th July 2019 following explosions and gun attacks in Kismayo. -

Improving Maternal Care in Dadaab Refugee Camps, Kenya
FIELD BRIEF To overcome this challenge, UNHCR and its health JUNE 2010 partners introduced community taxis “Mama Taxi” which are hired from the local community. Drivers’ mobile cell numbers are distributed to the block leaders for any emergency occuring during the evening and Improving Maternal Care in Dadaab nights. Refugee camps, Kenya The emphasis is put on referral for emergency obsetric and neonatal care although transport services are Kenya / Somali refugees / The Maternity Ward. also available for other emergencies. This has greatly Context Dagahaley Camp. Dadaab. / Photo: © Australia for UNHCR / T. Mukoya / October 2009 reduced delay in accessing care and increased the Dadaab is located in the Garissa district in the North Eastern Province of Kenya and is home to approximately number of women seeking hospital care at night. In 300,000 refugees, primarily (97%) from Somalia. addition, women who are in full-term and go to the health posts are encouraged to remain at the hospital in order to deliver there, even though labour may not yet have started. From 2007, Dadaab refugee camp has experienced a huge infl ux which doubled the population in less than two years. UNHCR f) Physical presence of health staff in the camps continues to receive and register new arrivals even though the Agency staff had been operating from Dadaab centre which is 5-15 kilometres away from the capacity of the camps is completely overstretched. Since the hospital, depending on the camp location. However, since the beginning of 2009, technical agency beginning of 2009, more than 72,500 new arrivals have been staff relocated to live near the hospitals, and this has improved 24 hour coverage and timely registered in the three adjacent refugee sites (10 – 15 km apart) that response to obstetric emergencies. -

REFUGEE CRISIS OVERVIEW a ABOUT ADOPT-A
room future - a - ww.unausa.org/adopt Future - A - Adopt visit: , on information more For grow and learn can community and $30,000 $30,000 and students where classroom new a builds • help. our need they but world, the around settings other children Rohingya of classroom one for facilities generation by educating refugee children in camps and and camps in children refugee educating by 600 600 $1 supports the construction of 2 WASH WASH 2 of construction the supports • prevent a lost lost a prevent working to to working are UNHCR and USA - UNA room trauma by affected children conflicts. escalating $750 $750 trains a teacher with methodologies to support support to methodologies with teacher a trains • curricula, family economic issues and problems created by by created problems and issues economic family curricula, students to enroll in school. in enroll to students of previous studies, different languages of instruction and and instruction of languages different studies, previous of $250 $250 school uniforms and supplies for 10 10 for supplies and uniforms school provides • primary education primary , such as the recognition of certification certification of recognition the as such , Refugees for Commissioner High UN What does it cost to help refugee children? refugee help to cost it does What problems in accessing accessing in problems additional experience Refugees Grandi Filippo survival” basic beyond y education refugee children deserve. children refugee education y qualit the provide compared to a world average of 91 of average world a to compared . % deal with the refugee crisis, it is essential that we think think we that essential is it crisis, refugee the with deal younger generations in need. -

Repor T AMISOM’S New Operation Juba Corridor in Somalia Has Received a Lot of Media Attention
ISSUE 73 | SEPTEMBER 2015 In this issue ■ On the Agenda Kenya has briefed the PSC on its plans to either close or relocate Dadaab, the world’s largest refugee camp. Kenya argues that Dadaab is a hotbed of al-Shabaab activity. ■ Situation Analysis The PSC recently returned from a field mission to Darfur, where violence continues despite the Peace & presence of UN and AU peacekeepers. ■ Addis Insight Security Both parties to the South Sudanese conflict were left out of the discussions during US President Barack Council Obama’s visit to Ethiopia. Analysts say the AU has made huge progress in improving its early warning system. Repor t AMISOM’s new Operation Juba Corridor in Somalia has received a lot of media attention. It does, however, raise a number of questions about AMISOM’s tactics and its reliance on neighbouring countries. “ Once you move “ Darfur would be “ The AU needs the refugees into worse off without to become more Somalia, they are UNAMID pro-active no longer refugees Page 3 Page 6 Page 12 PEACE AND SECURITY COUNCIL REPORT On the Agenda The future of the world’s largest refugee camp remains uncertain Dadaab is the world’s largest refugee camp. It is also, according to Kenya, a hotbed of al-Shabaab activity and a staging ground for terrorist attacks. Kenya briefed the PSC on Dadaab’s future last month. It is no secret that Dadaab refugee camp is a headache for Kenyan authorities, who have long been advocating for its closure or removal. Take this statement from then-Interior minister Joseph Ole Lenku in November 2013, several weeks after the al-Shabaab attack on Westgate shopping centre in Nairobi: ‘All the camps should be closed and the debate on whether or not it is appropriate has been passed by time.’ Or this, from Kenyan Deputy President William Ruto, in the wake of the horrific al- Shabaab attack on Garissa University, which claimed 147 lives in April this year. -
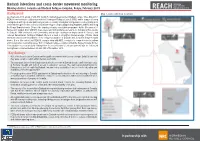
Dadaab Intentions and Cross-Border Movement Monitoring Dhobley District, Somalia and Dadaab Refugee Complex, Kenya, February 2019
Dadaab intentions and cross-border movement monitoring Dhobley district, Somalia and Dadaab Refugee Complex, Kenya, February 2019 Background Map 1. Data collection locations As of January 2019, a total of 209,9791 mostly Somali refugees reside in Dadaab camps. Since May 2017, REACH has worked in collaboration with the Norwegian Refugee Council (NRC) and in support of camp management and operational partners to provide secondary information and guidance on developing tools and methodologies for data collection in Dadaab refugee complex (Dagahaley, Hagadera and Ifo) and along the Kenya-Somalia border. Despite the ongoing voluntary repatriation programme by the Government of Kenya with support from UNHCR, there were reported spontaneous returns to Somalia and re-returns to Dadaab.2 With continued conflict, instability and drought causing new displacement in Somalia, and reduced humanitarian funding in Dadaab, there is a need to strengthen the knowledge of future return intentions and movement patterns of the refugee population in Dadaab and along the Kenya-Somalia border. It is in this context that REACH, in partnership with NRC, conducted a comprehensive intentions and cross-border monitoring survey both in Dadaab refugee complex and at the Kenya-Somalia border. This situation overview presents findings from the second round of this assessment, with the first round having been conducted between 6th and 15th of November 2018. Key findings • 46% of the households in Dadaab said they will not return to their Country of origin. Only 6% said that they were certain to return within the next six months. • The main push factors from Somalia reported by households in Dadaab include conflict and insecurity in Somalia, drought and lack of access to education services. -

East & Horn of Africa Update Somali Displacement Crisis at a Glance
East & Horn of Africa Update Somali Displacement Crisis at a glance 3 August 2011 Ifo extension, Dadaab Kenya. 28 July 2011 Highlights • UNHCR ups its July appeal to include $8.6 million to boost aid to displaced people inside Somalia. • Plans to deliver aid to up to 400,000 people inside Somalia by the end of August. • Ongoing Kenya operation moves more than 10,500 recent Somali arrivals to Dadaab’s Ifo camp. • Arrivals continue to average 1,300 daily at Kenya’s Dadaab camps; slow to 270 daily in Ethiopia’s Dollo Ado camps. • July arrivals in Dadaab camps top 40,400, the highest monthly rate in the camp’s 20-year history. • One in three children arriving in Ethiopia is acutely malnourished. • Mortality rate increases in July, with up to 1.8 deaths per 10,000 at Dadaab’s Ifo camp. • Malnutrition rates remain a concern iamong refugee new arrivals in Ethiopia and Kenya. • Africa Union to host pledging conference on the crisis in the Horn of Africa. Somali refugees in the region as at New Somali arrivals by country of asylum 01 Jan 2011 (by country of asylum) January to 31 July 2011 Asylum COUNTRY OF ASYLUM TOTAL NUMBER Jan Feb Mar Apr May Jun Jul Total country Kenya 351,773 Kenya 9,958 10,176 11,334 10,636 9,214 32,383 41,334 125,035 Ethiopia 81,247 2 76,676 Djibouti 14,216 Ethiopia 6,792 2,016 4,0 72 6,74 9 12,045 24,042 20,960 Yemen 180,341 Djibouti 384 293 359 246 398 425 833 2,938 Others 17,306 3 Total 644,883 Yemen 1,735 2,136 2,130 1,571 1,655 1,189 883 11,299 Total 18,869 14,621 17,895 19,202 23,312 58,039 64,010 215,948 Registered Somali refugees in the region 1 UNHCR revised emergency financial requirements, including Somalia (in million USD) Asylum Revised total Emergency requirements country budget included in total budget (2011) Kenya 172.1 68.8 Ethiopia 128.1 62.7 Djibouti 25.5 4.8 Somalia 75.4 8.6 Total 401.2 144.9 Percentage funded vs. -

Al-Shabaab and Political Volatility in Kenya
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by IDS OpenDocs EVIDENCE REPORT No 130 IDSAddressing and Mitigating Violence Tangled Ties: Al-Shabaab and Political Volatility in Kenya Jeremy Lind, Patrick Mutahi and Marjoke Oosterom April 2015 The IDS programme on Strengthening Evidence-based Policy works across seven key themes. Each theme works with partner institutions to co-construct policy-relevant knowledge and engage in policy-influencing processes. This material has been developed under the Addressing and Mitigating Violence theme. The material has been funded by UK aid from the UK Government, however the views expressed do not necessarily reflect the UK Government’s official policies. AG Level 2 Output ID: 74 TANGLED TIES: AL-SHABAAB AND POLITICAL VOLATILITY IN KENYA Jeremy Lind, Patrick Mutahi and Marjoke Oosterom April 2015 This is an Open Access publication distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are clearly credited. First published by the Institute of Development Studies in April 2015 © Institute of Development Studies 2015 IDS is a charitable company limited by guarantee and registered in England (No. 877338). Contents Abbreviations 2 Acknowledgements 3 Executive summary 4 1 Introduction 6 2 Seeing like a state: review of Kenya’s relations with Somalia and its Somali population 8 2.1 The North Eastern Province 8 2.2 Eastleigh 10 2.3