Oral Pigmented Lesions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Oral Diagnosis: the Clinician's Guide
Wright An imprint of Elsevier Science Limited Robert Stevenson House, 1-3 Baxter's Place, Leith Walk, Edinburgh EH I 3AF First published :WOO Reprinted 2002. 238 7X69. fax: (+ 1) 215 238 2239, e-mail: [email protected]. You may also complete your request on-line via the Elsevier Science homepage (http://www.elsevier.com). by selecting'Customer Support' and then 'Obtaining Permissions·. British Library Cataloguing in Publication Data A catalogue record for this book is available from the British Library Library of Congress Cataloging in Publication Data A catalog record for this book is available from the Library of Congress ISBN 0 7236 1040 I _ your source for books. journals and multimedia in the health sciences www.elsevierhealth.com Composition by Scribe Design, Gillingham, Kent Printed and bound in China Contents Preface vii Acknowledgements ix 1 The challenge of diagnosis 1 2 The history 4 3 Examination 11 4 Diagnostic tests 33 5 Pain of dental origin 71 6 Pain of non-dental origin 99 7 Trauma 124 8 Infection 140 9 Cysts 160 10 Ulcers 185 11 White patches 210 12 Bumps, lumps and swellings 226 13 Oral changes in systemic disease 263 14 Oral consequences of medication 290 Index 299 Preface The foundation of any form of successful treatment is accurate diagnosis. Though scientifically based, dentistry is also an art. This is evident in the provision of operative dental care and also in the diagnosis of oral and dental diseases. While diagnostic skills will be developed and enhanced by experience, it is essential that every prospective dentist is taught how to develop a structured and comprehensive approach to oral diagnosis. -

Two Cases of Nevoid Basal Cell Carcinoma Syndrome in One Family
221 Two Cases of Nevoid Basal Cell Carcinoma Syndrome in One Family Dong Jin Ryu, M.D., Yeon Sook Kwon, M.D., Mi Ryung Roh, M.D., Min-Geol Lee, M.D., Ph.D. Department of Dermatology and Cutaneous Biology Research Institute, Yonsei University College of Medicine, Seoul, Korea The nevoid basal cell carcinoma syndrome, or Gorlin-Goltz syndrome, is an autosomal dominant multiple system disorder with high penetrance and variable expressions, although it can also arise spontaneously. The diagnostic criteria for nevoid basal cell carcinoma syndrome include multiple basal cell carcinomas, palmoplantar pits, multiple odontogenic keratocysts, skeletal anomalies, positive family history, ectopic calcification and neurological anomalies. We report a brother and sister who were both diagnosed with nevoid basal cell carcinoma syndrome. (Ann Dermatol (Seoul) 20(4) 221∼225, 2008) Key Words: Basal cell carcinoma, Nevoid basal cell carcinoma syndrome, Odontogenic keratocyst INTRODUCTION cell carcinoma syndrome. The nevoid basal cell carcinoma syndrome (NBCCS), or Gorlin-Goltz syndrome, is an auto- CASE REPORT somal dominant multiple system disorder with high 1 penetrance and variable expressions . However, Case 1 60% of patients with NBCCS are sporadic cases. It An 11-year-old male was referred to our depart- has an estimated prevalence of 1 in 60,000 with ment for the evaluation of multiple miliary sized 2 equal distributions among males and females . The pigmented macules on the palm and sole that had well-defined diagnostic criteria include cutaneous increased in number over several years. He had an anomalies, dento-facial anomalies, skeletal ano- operation for inguinal hernia at 3 years of age, but malies, positive family history, neurological ano- no other medical problems. -

Research Article
z Available online at http://www.journalcra.com INTERNATIONAL JOURNAL OF CURRENT RESEARCH International Journal of Current Research Vol. 10, Issue, 07, pp.71222-71228, July, 2018 ISSN: 0975-833X RESEARCH ARTICLE THE TONGUE SPEAKS A LOT OF HEALTH. 1,*Dr. Firdous Shaikh, 2Dr. Sonia Sodhi, 3Dr Zeenat Fatema Farooqui and 4Dr. Lata Kale 1PG Student, Department of Oral Medicine and Radiology, CSMSS Dental College and Hospital, Aurangabad 2Professor, Department of Oral Medicine and Radiology, CSMSS Dental College and Hospital, Aurangabad 3Fatema Farooqui, Chief Medical Officer, Sri Ram Homeopathic Clinic and Research Center, Solapur 4Professor and Head, Department of Oral Medicine and Radiology, CSMSS Dental College and Hospital, Aurangabad ARTICLE INFO ABSTRACT Article History: Multifunctional organ of the human body without a bone yet strong is the tongue. It mainly consists Received 26th April, 2018 of the functional portion of muscle mass, mucosa, fat and the specialized tissue of taste i.e. the Received in revised form papillae. Diseases may either result from internal/ systemic causes of extrinsic causes like trauma, 14th May, 2018 infection, etc. A new method for classification has been proposed in this review for diseases of Accepted 09th June, 2018 tongue. This review mainly focuses on encompassing almost each aspect that the body reflects via its th Published online 30 July, 2018 mirror in mouth, the tongue. Key Words: Tongue, Diseases of Tongue, Discoloration of Tongue, Oral health, Hairy Tongue. Copyright © 2018, Firdous Shaikh et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. -

Acquired Bilateral Nevus of Ota–Like Macules (Hori's Nevus): a Case
Acquired Bilateral Nevus of Ota–like Macules (Hori’s Nevus): A Case Report and Treatment Update Jamie Hale, DO,* David Dorton, DO,** Kaisa van der Kooi, MD*** *Dermatology Resident, 2nd year, Largo Medical Center/NSUCOM, Largo, FL **Dermatologist, Teaching Faculty, Largo Medical Center/NSUCOM, Largo, FL ***Dermatopathologist, Teaching Faculty, Largo Medical Center/NSUCOM, Largo, FL Abstract This is a case of a 71-year-old African American female who presented with bilateral periorbital hyperpigmentation. After failing treatment with a topical retinoid and hydroquinone, a biopsy was performed and was consistent with acquired bilateral nevus of Ota-like macules, or Hori’s nevus. A review of histopathology, etiology, and treatment is discussed below. cream and tretinoin 0.05% gel. At this visit, a Introduction Figure 2 Acquired nevus of Ota-like macules (ABNOM), punch biopsy of her left zygoma was performed. or Hori’s nevus, clinically presents as bilateral, Histopathology reported sparse proliferation blue-gray to gray-brown macules of the zygomatic of irregularly shaped, haphazardly arranged melanocytes extending from the superficial area. It less often presents on the forehead, upper reticular dermis to mid-deep reticular dermis outer eyelids, and nose.1 It is most common in women of Asian descent and has been reported Figure 4 in ages 20 to 70. Classically, the eye and oral mucosa are uninvolved. This condition is commonly misdiagnosed as melasma.1 The etiology of this condition is not fully understood, and therefore no standardized treatment has been Figure 3 established. Case Report A 71-year-old African American female initially presented with a two week history of a pruritic, flaky rash with discoloration of her face. -

Co-Occurrence of Vitiligo and Becker's Nevus: a Case Report
Case Report Olgu Sunumu DOI: 10.4274/turkderm.71354 Turkderm - Arch Turk Dermatol Venerology 2016;50 Co-occurrence of vitiligo and Becker's nevus: A case report Vitiligo ve Becker nevüs birlikteliği: Olgu sunumu Ayşegül Yalçınkaya İyidal, Özge Çokbankir*, Arzu Kılıç** Ağrı State Hospital, Clinic of Dermatology, *Clinic of Pathology, Ağrı, Turkey **Balıkesir University Faculty of Medicine, Department of Dermatology, Balıkesir, Turkey Abstract Vitiligo is an acquired disorder with an unknown etiology in which genetic and non-genetic factors coexist. Melanocytes are destructed in the affected skin areas and clinically depigmented macules and patches appear on the skin. Becker's nevus (BN) appears as hyperpigmented macule, patch or verrucous plaques with sharp and irregular margins and often unilateral occurrence and with associated hypertrichosis in various degrees. Although its pathogenesis is unknown, it is suggested to represent a hamartomatous lesion harboring androgen receptors on the lesion. In this report, we present a 19-year-old male patient who developed vitiligo lesions and then BN adjacent to the vitiligo lesion in the right upper back portion of the body ten years after the initial vitiligo lesion. Keywords: Becker's nevus, vitiligo, co-occurrence Öz Vitiligo nedeni tam olarak bilinmeyen, genetik ve genetik olmayan faktörlerin birlikte rol oynadığı edinsel bir bozukluktur. Bu hastalıkta tutulan deride melanositler ortadan kalkar, klinik olarak depigmente makül ve yamalar belirir. Becker nevüs (BN) sıklıkla unilateral dağılım gösteren, keskin ama düzensiz sınırlı hiperpigmente makül, yama veya verrüköz plakların izlendiği, üzerinde değişik derecelerde hipertrikozun bulunduğu bir hastalıktır. Patogenezi belli olmamakla birlikte hamartamatöz bir lezyon olduğu ve üzerinde androjen reseptörlerinin arttığı ileri sürülmektedir. -

Dermoscopy on Nevus Comedonicus: a Case Report and Review of the Literature
Case report Dermoscopy on nevus comedonicus: a case report and review of the literature Grażyna Kamińska-Winciorek 1, Radosław Śpiewak 2 1The Center for Cancer Prevention and Treatment, Katowice, Poland Head: Beata Wydmańska 2Department of Experimental Dermatology and Cosmetology, Faculty of Pharmacy, Jagiellonian University Medical College, Krakow, Poland Head: Prof. Radosław Śpiewak MD. PhD Postep Derm Alergol 2013; XXX, 4: 252 –254 DOI: 10.5114/pdia.2013.37036 Abstract Nevus comedonicus (NC) is a very rare, benign hamartoma characterised by the occurrence of dilated, comedo-like openings, typically on the face, neck, upper arms, chest or abdomen. In uncertain cases, histopathological exami - nation confirms the diagnosis. The authors suggest dermoscopy as a rapid and useful method of initial diagnosis of nevus comedonicus based upon its distinctive dermoscopic features. The dermoscopy reveals numerous light- and dark-brown, circular or barrel-shaped, homogenous areas with prominent keratin plugs. Key words: dermoscopy, dermatoscopy, nevus comedonicus, epidermal nevus, acne vulgaris. Introduction a hypopigmented, slightly hypotrophic, linear spot of Nevus comedonicus (NC) is a benign hamartoma cha - 2 cm × 8 cm (Figure 1). The plugs could not be extracted racterised by the occurrence of dilated comedo-like open - mechanically. The dermoscopic examination revealed ings, with black or brown keratin plugs, typically localised the distinctive pattern consisting of dark, sharply demar - on the face, neck, upper arms, chest or abdomen. The diag - cated keratin plugs of 1–3 mm diameter, numerous struc - nosis of nevus comedonicus is relatively easy. In uncertain tureless, circular- and barrel-shaped, homogenous areas cases, a typical histopathological picture confirms the diag - with hyperkeratotic plugs of various shades of brown nosis. -
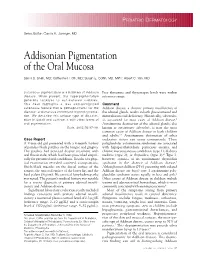
Addisonian Pigmentation of the Oral Mucosa
PEDIATRIC DERMATOLOGY Series Editor: Camila K. Janniger, MD Addisonian Pigmentation of the Oral Mucosa Samir S. Shah, MD; Catherine H. Oh, MD; Susan E. Coffin, MD, MPH; Albert C. Yan, MD Cutaneous pigmentation is a hallmark of Addison Free thyroxine and thyrotropin levels were within disease. When present, the hyperpigmentation reference range. generally localizes to sun-exposed surfaces. This case highlights a less well-recognized Comment cutaneous feature that is pathognomonic for the Addison disease, a chronic primary insufficiency of disease: oral mucous membrane hyperpigmenta- the adrenal glands, results in both glucocorticoid and tion. We describe this unique type of discolor- mineralocorticoid deficiency. Historically, tuberculo- ation in detail and contrast it with other forms of sis accounted for most cases of Addison disease.1 oral pigmentation. Autoimmune destruction of the adrenal glands, also Cutis. 2005;76:97-99. known as autoimmune adrenalitis, is now the most common cause of Addison disease in both children and adults.2,3 Autoimmune destruction of other Case Report endocrine tissues can occur concurrently. These A 9-year-old girl presented with a 4-month history polyglandular autoimmune syndromes are associated of painless black patches on the tongue and gingiva. with hypoparathyroidism, pernicious anemia, and The patches had persisted despite treatment with chronic mucocutaneous candidiasis (type 1); diabetes oral fluconazole, which had been prescribed empiri- mellitus (type 2); or thyroiditis (type 3).4 Type 3, cally for presumed oral candidiasis. Results of a phys- however, consists of an autoimmune thyroiditis ical examination revealed scattered, asymptomatic, syndrome in the absence of Addison disease.5 bluish-black macules on the dorsal surface of the Although most children (75%) presenting with isolated tongue, the mucosal surface of the lower lip, and the Addison disease are boys,6 type 1 autoimmune poly- hard palate (Figure). -

The Role of Androgen Receptors in the Clinical Course of Nevus Sebaceus of Jadassohn Katherine S
The Role of Androgen Receptors in the Clinical Course of Nevus Sebaceus of Jadassohn Katherine S. Hamilton, M.D., Sandra Johnson, M.D., Bruce R. Smoller, M.D. Department of Pathology, Vanderbilt University Medical Center, Nashville, Tennessee (KSH); and Departments of Dermatology (SJ, BRS) and Pathology (SJ), University of Arkansas for Medical Services, Little Rock, Arkansas During puberty, they usually enlarge and become Nevus sebaceus of Jadassohn (NSJ) is a benign, con- elevated, verrucous, or nodular and may appear genital hamartoma that often presents at birth, ap- brown (1, 2). In late childhood and adulthood, there pears to regress in childhood, and grows during is a significant risk of developing a secondary tu- puberty, suggesting possible hormonal control. We mor, the most common of which are syringocysta- studied 18 cases of NSJ from children and adults for denoma papilliferum and basal cell carcinoma (1, immunohistochemical evidence of androgen recep- 3). Myriad other cutaneous appendageal neoplasms tor expression. The lesions were evaluated for loca- have also been reported to arise within NSJ. tion and pattern of immunostaining, and these Androgen receptors (AR) are nuclear ligand–de- findings were compared between age groups, sexes, pendent transcription factors of the steroid super- and to androgen receptor expression in normal family that bind testosterone and dihydroxytestos- skin. Androgen receptor positivity was seen in the terone (4). AR have been identified in normal sebaceous glands, in eccrine glands with and with- cutaneous structures and in some epithelial tu- out apocrine change, and rarely in keratinocytes in mors. In normal skin, AR have been localized to the sebaceous nevi. -

Choroidal Nevus Transformation Into Melanoma: Analysis of 2514 Consecutive Cases
CLINICAL SCIENCES Choroidal Nevus Transformation Into Melanoma Analysis of 2514 Consecutive Cases Carol L. Shields, MD; Minoru Furuta, MD; Edwina L. Berman, BS; Jonathan D. Zahler, MD; Daniel M. Hoberman, BS; Diep H. Dinh, BS; Arman Mashayekhi, MD; Jerry A. Shields, MD Objective: To determine features that are predictive of halo absence (P=.009). A mnemonic device to recall risk growth of choroidal nevi into melanoma. factors of ocular melanoma is “To find small ocular mela- noma using helpful hints,” representing thickness, fluid, Methods: This was a retrospective medical record re- symptoms, orange pigment, margin, ultrasonographic hol- view of 2514 consecutive eyes; Kaplan-Meier estimates lowness, and halo absence. The median hazard ratio for and Cox regression analyses were used. those with 1 to 2 risk factors was 3; for 3 or 4 factors, 5; for 5 to 6 factors, 9; and for all 7 factors, 21. Results: The median tumor basal diameter was 5.0 mm and thickness was 1.5 mm. Nevus growth into mela- Conclusions: In an analysis of 2514 choroidal nevi, fac- noma occurred in 2%, 9%, and 13% of eyes at 1, 5, and tors predictive of growth into melanoma included greater 10 years, respectively. Factors predictive of growth into thickness, subretinal fluid, symptoms, orange pigment, melanoma by multivariable analysis included tumor thick- margin near disc, and 2 new features: ultrasonographic ness greater than 2 mm (PϽ.001), subretinal fluid hollowness and absence of halo. (P =.002), symptoms (P =.002), orange pigment (PϽ.001), tumor margin within 3 mm of the optic disc (P=.001), ultrasonographic hollowness (PϽ.001), and Arch Ophthalmol. -

Differentiating Malignant Melanoma from Other Lesions Using Dermoscopy
PRAXIS Differentiating malignant melanoma from other lesions using dermoscopy Ahmed Mourad Robert Gniadecki MD PhD DMSci ermoscopy (also called dermatoscopy, epilumi- nescent microscopy, or episcopy) is a noninvasive Figure 1. Image depicting proper dermoscopic technique: method of examining skin lesions using a hand- This is a polarized light dermoscope and does not require Dheld magnifying device (a dermoscope) equipped with a direct contact with the skin or application of oil. light source.1 Dermoscopy allows adequate visualization of the structures in the skin not only by magnifying them but also by eliminating the surface light reflection and scatter that obscures the deeper features.2,3 This arti- cle provides information on the dermoscopic features specific to malignant melanoma and other pigmented lesions that often resemble malignant melanoma via naked-eye examination (ie, benign melanocytic nevus [BMN], seborrheic keratosis, and dermatofibroma). Technique Before evaluating the lesion of interest using dermoscopy, the clinician should take an adequate history and evalu- ate the morphology and distribution of the lesion with the naked eye.1 Dermoscopy is then performed by apply- ing the dermoscope on the lesion of interest and looking through the lens to visualize the morphologic features of The presence of 2 or more of the above features sug- the skin lesion (Figure 1). Dermoscopy should never be gests a suspicious lesion that should be biopsied or that used alone, and the dermoscopic result should be corre- the patient should be referred for further assessment.4 lated with that of the naked-eye examination. The cost of a dermoscope ranges from a few hundred Conditions to a few thousand dollars. -

Lumps & Bumps: Approach to Common Dermatologic Neoplasms
Case-Based Approach to Common Dermatologic Neoplasms Patrick Retterbush, MD, FAAD Mohs Surgery & Dermatologic Oncology Associate Member of the American College of Mohs Surgery Private Practice: Lockman Dermatology January 27th 2018 Disclosure of Relevant Financial Relationships • I do not have any relevant financial relationships, commercial interests, and/or conflicts of interest regarding the content of this presentation. Goals/Objectives • Recognize common benign growths • Recognize common malignant growths • Useful clues & examination for evaluating melanocytic nevi and when to be concerned for melanoma/atypical moles • How to perform a basic skin biopsy and which method/type to choose • Basic treatment/when to refer Key Questions & Physical Examination Findings for a Growth History Physical Examination • How long has the lesion been • Describing a growth present? – flat or raised? • flat – macule (<1cm) or patch (>1cm) – years, months, weeks • raised – papule (<1cm) or plaque (>1cm) – nodule if deep (majority of lesion in • Has it changed? dermis/SQ) – Size – secondary descriptive features • scaly (hyperkeratosis, retention of strateum – Shape corneum) – Color • crusty (dried serum, blood, or pus on surface) • eroded or ulcerated (partial vs. full thickness – Symptoms – pain, bleeding, itch? epidermal loss) – Over what time frame? • color (skin colored, red, pigmented, pearly) • feel (hard or soft, mobile or fixed) • PMH: • size: i.e. 6 x 4mm – prior skin cancers • Look at the rest of the skin/region of skin • SCC/BCCs vs. melanoma -

Oral and Maxillo-Facial Manifestations of Systemic Diseases: an Overview
medicina Review Oral and Maxillo-Facial Manifestations of Systemic Diseases: An Overview Saverio Capodiferro *,† , Luisa Limongelli *,† and Gianfranco Favia Department of Interdisciplinary Medicine, University of Bari Aldo Moro, Piazza G. Cesare, 11, 70124 Bari, Italy; [email protected] * Correspondence: [email protected] (S.C.); [email protected] (L.L.) † These authors contributed equally to the paper. Abstract: Many systemic (infective, genetic, autoimmune, neoplastic) diseases may involve the oral cavity and, more generally, the soft and hard tissues of the head and neck as primary or secondary localization. Primary onset in the oral cavity of both pediatric and adult diseases usually represents a true challenge for clinicians; their precocious detection is often difficult and requires a wide knowledge but surely results in the early diagnosis and therapy onset with an overall better prognosis and clinical outcomes. In the current paper, as for the topic of the current Special Issue, the authors present an overview on the most frequent clinical manifestations at the oral and maxillo-facial district of systemic disease. Keywords: oral cavity; head and neck; systemic disease; oral signs of systemic diseases; early diagnosis; differential diagnosis Citation: Capodiferro, S.; Limongelli, 1. Introduction L.; Favia, G. Oral and Maxillo-Facial Oral and maxillo-facial manifestations of systemic diseases represent an extensive and Manifestations of Systemic Diseases: fascinating study, which is mainly based on the knowledge that many signs and symptoms An Overview. Medicina 2021, 57, 271. as numerous systemic disorders may first present as or may be identified by head and https://doi.org/10.3390/ neck tissue changes.