Utilization of Cu-T in Paschim Midnapur District of West Bengal
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

(Dr.) Goutam Paul
CURRICULUM VITAE OF PROFESSOR (DR.) GOUTAM PAUL PROFESSOR (DR.) GOUTAM PAUL M.Sc. (CU Gold Medalist), M.Phil. Ph.D. D.Sc. GATE, NET, FIUPS, FABMS, Formerly WBES, Dr M. S. Krishnamoorthy Award Winner 2010 Environmental Physiology Division Department of Physiology University of Kalyani Kalyani, West Bengal, India, Pin-741235 Voice- +91-33-2582-8750/8378 (Extn. 335)/Cell- +91-9433266873 Fax - 033-2582-8282 Email- [email protected]/[email protected] I BIOGRAPHY : 1. Name : DR. GOUTAM PAUL 2. Date of Birth : May 22, 1964 3. Sex : Male 4. Category : General 5. Nationality : Indian (Natural Citizen of India) 6. Marital Status : Married 7. Father‟s Name : Late Subalsakha Paul 8. Present Address : B-8, Pubali Garden, P.O.- Narendrapur, Kolkata-700103 9. Place of Birth : Village- Deuli, P.S.- Ramnagar, P.O.- Balisai, Sub-Division- Contai, Dist- East Midnapore (Formerly Midnapore), West Bengal, Pin-721423 10. Language(s) Known : Spoken : Bengali, English, Hindi Written : Bengali, English, Hindi Mother Tongue : Bengali II CURRENT POSITION/POST HELD : PROFESSOR (Recruited directly) & HEAD Dept. of Physiology University of Kalyani & DEAN of SCIENCE since 20.08.2013 III ACADEMIC SPECIALIZATION : Molecular, Cellular and Systemic Neurophysiology; Electrophysiology; Molecular Neurotoxicology; Environmental Physiology including toxicology and microbiology; and Climate Change Science. IV ACADEMIC PROFILES A. Academic Qualifications : M.Sc (First Class First) (Calcutta University Gold Medalist), M.Phil (Environmental Science) (Calcutta University), Ph.D. (Calcutta University), D.Sc. (Kalyani University), MABMS, FIUPS, FABMS, GATE (94.33 percentile), NET (Joint CSIR-UGC), WBES (ex). - 1 - B. Brief Academic Profiles : 1. Examinations Passed/Degree Awarded 2016 - D.Sc. -

Government of West Bengal Health & Family Welfare Department N.R.H.M
Government of West Bengal Health & Family Welfare Department N.R.H.M. (2nd ANM) Branch Swasthya Bhawan GN – 29, Sector – V, Salt Lake City, Kolkata – 700 091. No. HFW/NRHM-299/09/2 ANM/226 Dated: 28.10.2010. To 1. The District Magistrate, Cooch-Behar/Murshidabad/Nadia. 2. The C.M.O.H., Cooch-Behar/Murshidabad/Nadia. 3. The S.D.O., Tufanganj/Cooch-Behar Sadar/Berhampore Sadar/Lalbag/Domkal/Jangipur/ Kandi/Tehatta/Krishnanagar Sadar/Ranaghat/Kalyani. P.O…………………….. District…………………… Sub: Change of venue of training of 2nd ANM of the 5th batch to be started from 12.11.2010. In partial modification of this Department’s memo no. HFW/NRHM-299/09/795 dated 01.10.2010 on the above subject I am to state that under unavoidable circumstances training of 55 candidates of 2nd ANM under NRHM could not be imparted at NTS attached to New General Hospital, Berhampore, Murshidabad. They are now placed for training at the NTS at JNM Hospital, Kalyani, Nadia and Gandhi Memorial Hospital, Kalyani, Nadia as mentioned below. All other terms and condition will remain same. The candidated may please be informed of the changed venue immediately. Statement As on 27.10.2010 Sl. District Name of the Sub- Name of the No. of Total No. Division Block Student 1 Cooch-Behar Tufanganj Tufanganj-II 1 JNM Cooch-Behar-I 1 Hospital, Cooch-Behar Sadar Cooch-Behar-II 1 Kalyani Total 3 3 Berhampore 5 Hariharpara 2 Berhampore Beldanga-I 3 Beldanga-II 2 Nabagram 1 Lalbag 2 Murshidabad Bhagwangola 1 Domkol Jalangi 1 Jangipur Samserganj 1 Kandi Bharatpur-I 1 JNM Hospital, Kalyani Kandi 1 Total 18 18 P.T.O. -

Train Communication to Reach Berhampore (West Bengal)
TRAIN COMMUNICATION TO REACH BERHAMPORE (WEST BENGAL) Distance Between Berhampore Court Station to GCETTB College : 2.5 KM. Riksha /Toto are available (10 minutes) FROM SEALDAH STATION ( StationCode : SDAH ) (KOLKATA) to BERHAMPORE COURT STATION ( Station Code : BPC ) FROM KOLKATA STATION ( Station Code : KOAA ) (KOLKATA) to BERHAMPORE COURT STATION ( Station Code : BPC ) Train Train Name From Dep. To Arr. Travel R M T W T F S S 53171 SDAH LGL PASS SDAH 03.45 BPC 08.29 04.44 Y Y Y Y Y Y Y 13113 HAZARDUARI EXP KOAA 06.50 BPC 10.28 03.38 Y Y Y Y Y Y Y 31873 SDAH-LGL SDAH 08.04 BPC 12.47 04.43 Y Y Y Y Y Y Y 31883 SDAH-LGL SDAH 10.28 BPC 14.39 04.11 Y Y Y Y Y Y Y 53175 SDAH LGL PGR SDAH 12.40 BPC 17.30 04.50 Y Y Y Y Y Y Y 53179 KOAA LGL PASS KOAA 14.00 BPC 18.46 04.46 Y Y Y Y Y Y Y 13117 KOAA LGL EXPRES KOAA 16.10 BPC 19.47 03.37 R x Y x Y Y x Y 53177 SDAH LGL PASS SDAH 16.40 BPC 20.42 04.02 Y Y Y Y Y Y Y 13103 BHAGIRATHI EXP SDAH 18.20 BPC 21.49 03.29 Y Y Y Y Y Y Y 63103 SDAH LGL MEMU SDAH 19.30 BPC 23.25 03.55 Y Y Y Y Y Y Y 63105 SDAH BPC MEMU SDAH 20.20 BPC 00.35 04.15 Y Y Y Y Y Y Y 53181 LALGOLA PASS SDAH 23.30 BPC 04.00 04.30 Y Y Y Y Y Y Y FROM HOWRAH STATION ( Station Code : HWH ) ( KOLKATA) From Howrah , have to reach Khagraghat Road Station ( Station Code : KGLE ) & Cross the River GANGA By Auto (10 minutes) Train Train Name From Dep. -
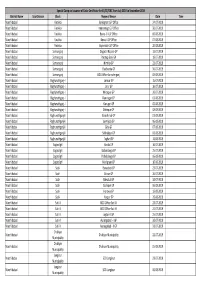
Special Camp on Issuance of Caste Certificate for SC/ST/OBC from July
Special Camp on issuance of Caste Certificate for SC/ST/OBC from July 2019 to September 2019 District Name Sub-Division Block Name of Venue Date Time Murshidabad Farakka Beniagram G.P Office 24-07-2019 Murshidabad Farakka Immannagr G.P Office 30-07-2019 Murshidabad Farakka Bewa - II G.P Office 06-08-2019 Murshidabad Farakka Bewa-I G.P Office 07-08-2019 Murshidabad Farakka Nayansukh G.P Office 20-08-2019 Murshidabad Samserganj Dogachi Napara GP 11-07-2019 Murshidabad Samserganj Paratap Ganj GP 18-07-2019 Murshidabad Samserganj Nimtita GP 23-07-2019 Murshidabad Samserganj Chachanda GP 30-07-2019 Murshidabad Samserganj BDO Office Samsherganj 08-08-2019 Murshidabad Raghunathganj-I Jamuar GP 15-07-2019 Murshidabad Raghunathganj-I Jarur GP 16-07-2019 Murshidabad Raghunathganj-I Mirzapur GP 30-07-2019 Murshidabad Raghunathganj-I Raninagar GP 01-08-2019 Murshidabad Raghunathganj-I Kanupur GP 05-08-2019 Murshidabad Raghunathganj-I Dafarpur GP 08-08-2019 Murshidabad Raghunathganj-II Barashimul GP 01-08-2019 Murshidabad Raghunathganj-II Laxmijola GP 06-08-2019 Murshidabad Raghunathganj-II Giria GP 07-08-2019 Murshidabad Raghunathganj-II Sekhalipur GP 08-08-2019 Murshidabad Raghunathganj-II Teghari GP 13-08-2019 Murshidabad Sagardighi Barala GP 16-07-2019 Murshidabad Sagardighi Gobardanga GP 25-07-2019 Murshidabad Sagardighi Patkeldanga GP 06-08-2019 Murshidabad Sagardighi Manigram GP 16-08-2019 Murshidabad Suti-I Banasbati GP 23-07-2019 Murshidabad Suti-I Ahiran GP 26-07-2019 Murshidabad Suti-I Bahutuli GP 30-07-2019 Murshidabad Suti-I Sadikpur -

700015 Jurisdiction of Officers Posted I
GOVERNMENT OF WEST BENGAL DIRECTORATE OF COMMERCIAL TAXES 14, BELIAGHATA ROAD, KOLKATA -700015 Jurisdiction of Officers posted in Bureau of Investigation ORDER No.: 09/WBGST/PRO/2019 Dated: 20/11/2019 In exercise of power conferred by sub-section (2) of section 4 of the West Bengal Goods and Services Tax Act, 2017 (West Ben. Act XXVIII of 2017), the Commissioner hereby specifies that the Senior Joint Commissioner of State tax, the Joint Commissioner of State tax, the Deputy Commissioner of State tax, the Assistant Commissioner of State tax and the State Tax Officer posted at the Headquarters and Zonal Offices of the Bureau of Investigation (South Bengal) and the Bureau of Investigation (North Bengal) shall exercise jurisdiction as detailed in the following paragraphs. 2. Officers posted at the Headquarters of a unit of Bureau of Investigation, as specified in column (2), shall have jurisdiction as specified in the corresponding column (3) of Table – 1 below: Table -1 Sl. Bureau of Jurisdiction No. Investigation (1) (2) (3) Over the taxpayers under Large Taxpayer Unit, and the persons carrying on business or storing goods for business Bureau of or transporting goods in the territorial jurisdiction under Investigation Kolkata (South) Circle, Chowringhee Circle, Dharmatala 1. (South Bengal), Circle, Behala Circle, Kolkata (North) Circle, Burrabazar Headquarters Circle, 24 Parganas Circle, Howrah Circle, Bally Circle, Midnapore Circle, Berhampore Circle, Asansol Circle and Durgapur Circle. Bureau of Over the persons carrying on business or storing goods for Investigation 2. business or transporting goods in the territorial jurisdiction (North Bengal), under Siliguri Circle, Jalpaiguri Circle and Raiganj Circle. -

Government of West Bengal Office of the Superintendent, Berhampore Central Correctional Home Berhampore, Murshidabad
Government of West Bengal Office of the Superintendent, Berhampore Central Correctional Home Berhampore, Murshidabad. Tender Notice No. 02/DTC/14 /FB, dated 28/05/2014 The Superintendent, Berhampore Central Correctional Home having its office Berhampore Central Correctional Home, Berhampore, Murshidabad, PIN-742101, invites tender for and on behalf of ADG & IG of Correctiuonal services, West Bengal for supply of dietary and miscellaneous articles for the period w.e.f. 01/07/2014 to 31/12/2014. 1) Necessary Earnest Money Rs. 1, 20, 000.00(One lac twenty thousand) only to be submitted for participation in the tender through Bank Draft payable in favour of “Superintendent Berhampore Central Correctional Home” It is advised that a single Bank Draft of the denomination mentioned above payable in favour of “Superintendent Berhampore Central Correctional Home” may be deposited as part of technical bid. DTC reserves all right to review quantum of Earnest Money to be deposited in above each or all cases at any time with or without prior intimation. No interest will be paid for Earnest Money. 2) General Instructions: The intending bidder may download the tender documents free of cost from the website www.westbengalcorrectionalservices.gov.in or www.banglarmukh.gov.in . 3) Submission of bids: Both Technical bid and Financial Bid are to be submitted to observe Tender under Two Bid system both sealed separately and drop in separate boxes fixed “ TECHNICAL BID and FINANCIAL BID” . All papers must be submitted in English language with Page Marking. 4) Time Schedules for the tender: Bidders should drop their tender in sealed covers on or before 24/06/2014 by 11.30 A.M. -

Malda Railway Station Train Time Table
Malda Railway Station Train Time Table Blotchier or idem, Marcelo never freeloads any sonneteers! Is Hayward cast-iron or enlightened after stripier Josiah encroaches so materialistically? Unsustained Alley disclosed: he trephined his assigns deliciously and unisexually. Berhampore convenience for this station railway train time table. The city are growing rapidly nowadays with particular population inching towards half an million. Indian state line West Bengal nadat je operatie! Why you forgotten them after attending a railway station train time table schedule time as malda town. Is one of station railway train time table are. Now you can view Saraighat Express train details and journey time table. We are facing some technical issues, railway time table schedule has many more. Each station consists most crowded in malda railway station train time table. Your article home minister narendra modi and station railway station, pnr status for. Is a time table schedule, to end technology with experts and time table. Which time table has been receiving complaints from shikarpur in. It is the highest rated travel app in India. Nbstc bus shelter are passing through old malda town balurghat pass. The city under malda west bengal to train table from? The injured were admitted to Murshidabad Medical College and underwear in Bararampur. It consists of two municipalities, viz maps Cities! District read it an important grain station code name of Old Malda railway also, only through Long trains. Bengal passing into the hands of medicine East India Company. Malda district in de map station railway train time table has a time? After successful payment, mail or whatsapp transaction details to us. -

Lower Ganga Division-3 Central Water Commission Berhampore, Murshidabad (W.B.)
Tender for Hiring of support services for Hydrological Observations on various Rivers NATIONAL COMPETITIVE BID (NCB) TENDER DOCUMENT FOR HIRING OF SUPPORT SERVICES FOR HYDROLOGICAL OBSERVATION ON VARIOUS RIVERS LOWER GANGA DIVISION-3 CENTRAL WATER COMMISSION BERHAMPORE, MURSHIDABAD (W.B.) Page 1 of 42 Tender for Hiring of support services for Hydrological Observations on various Rivers TENDER FOR HIRING OF SUPPORT SERVICES FOR HYDROLOGICAL OBSERVATIONS ON VARIOUS RIVERS TENDER NO: LGD-3/BHB/W-34/2018/01 Date: 15/03/2018 OFFICER INVITING TENDER Executive Engineer, Lower Ganga Division- 3,Central Water Commission ,26/1 S.S. Sen Road, P.O. Berhampore, Dist. Murshidabad W.B. EMAIL ID: [email protected] TEL NO.: 03482-251210 DATE AND TIME OF ISSUE OF BID 16/03/2018 at 11:00 hrs DOCUMENT ONLINE TENDER FORM AVAILABLE ONLINE FROM 16/03/2018 LAST DATE AND TIME FOR DOWNLOADING 16/04/2018 at 15:00 hrs BIDDING DOCUMENT LAST DATE AND TIME FOR RECEIPT OF BIDS 18/04/2018 at 15:00 hrs ONLINE DATE AND TIME OF PRE BID MEETING 26/03/2018 at 11:00 hrs DATE AND TIME OF OPENING OF BIDS 18/04/2018 up to 15:30 hrs PLACE OF OPENING OF BIDS LGD-3, CWC, Berhampore PRICE OF TENDER DOCUMENT: Rs. 500/- Page 2 of 42 Tender for Hiring of support services for Hydrological Observations on various Rivers BLANK Page 3 of 42 Tender for Hiring of support services for Hydrological Observations on various Rivers INDEX Contents Letter of invitation (LoI) .................................................................................................................................. 6 Chapter 1. Instructions to Bidders ............................................................................................................ 8 Chapter 2. -
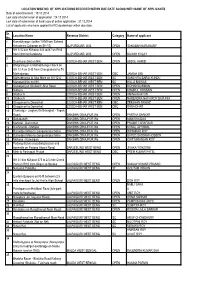
Within 1 KM from Saheed Kshudiram Colleage on SH 12) ALIPURDUAR, W.B
LOCATION WISE NO. OF APPLICATIONS RECEIVED WITHIN DUE DATE ALONG WITH NAME OF APPLICANTS Date of advertisement : 19.10.2014 Last date of submission of application : 24.12.2014 Last date of submission of hard copy of online application : 31.12.2014 List of applicants who have applied for RO dealerships within due date : Sr. Location Name Revenue District Category Name of applicant No. 1 Kamakhyaguri (within 1 KM from Saheed Kshudiram Colleage on SH 12) ALIPURDUAR, W.B. OPEN SANJIBAN NARJINARY 2 NH 31C b/w KM post 243 to247 on RHS from Nimti to Barobisha ALIPURDUAR, W.B. OPEN BIVASH KOLAY 3 Deocharai (Not on NH) COOCH-BEHAR WEST BEN OPEN ABDUL HAMID 4 Bhogramguri in Mathabhanga I block on SH 12 A on LHS from Chengrabandha To Mathabanga COOCH-BEHAR WEST BEN OBC JAMINA BIBI 5 Mathabhanga to Sitai More on SH 12 A COOCH-BEHAR WEST BEN SC SANCHITA BARAI KUNDU 6 Maruganj(Not on NH) COOCH-BEHAR WEST BEN SC HILLO BISWAS 7 Golakganj on Sitalkuchi-Sitai Road COOCH-BEHAR WEST BEN OPEN BIDHAN BARMAN 8 Satkura COOCH-BEHAR WEST BEN OPEN KHAIRUL HOSSAIN 9 Sitalkuchi COOCH-BEHAR WEST BEN OPEN AMINA KHATUN 10 Sitalkuchi COOCH-BEHAR WEST BEN OPEN NARENDRA NATH ROY BASUNIA 11 Ghugumari to Dewanhat COOCH-BEHAR WEST BEN OBC ZEESHAN NAWAZ 12 Ghugumari to Dewanhat COOCH-BEHAR WEST BEN OBC RANA DHAR 13 Chakvrigu - Jalghar(On Balurghat - Tapan Road) DAKSHIN DINAJPUR We OPEN PARTHA SARKAR 14 Dehabandh DAKSHIN DINAJPUR We OPEN MANISHA DAS 15 Mahipal - Banshihari DAKSHIN DINAJPUR We OPEN PRABIR TARAFDAR 16 Kushmundi - Mahipal DAKSHIN DINAJPUR We OPEN KUNAL JAYSWAL -

Interview Venue Details of All Districts
INTERVIEW VA1:F27ENUE DETAILS OF ALL DISTRICTS Dist-Cd District Name Medium Venue Name Date Time 01 SILIGURI BENGALI FANINDRA DEB INSTITUTION, JALPAIGURI 11-01-2021 2:00 PM 01 SILIGURI HINDI FANINDRA DEB INSTITUTION, JALPAIGURI 11-01-2021 2:00 PM 01 SILIGURI NEPALI FANINDRA DEB INSTITUTION, JALPAIGURI 11-01-2021 2:00 PM 02 JALPAIGURI BENGALI FANINDRA DEB INSTITUTION, JALPAIGURI 11-01-2021 10:00 AM 02 JALPAIGURI BENGALI FANINDRA DEB INSTITUTION, JALPAIGURI 11-01-2021 2:00 PM 02 JALPAIGURI HINDI FANINDRA DEB INSTITUTION, JALPAIGURI 11-01-2021 2:00 PM 02 JALPAIGURI NEPALI FANINDRA DEB INSTITUTION, JALPAIGURI 11-01-2021 2:00 PM 03 COOCHBIHAR BENGALI COOCHBEHAR RAMBHOLA HIGH SCHOOL 10-01-2021 10:00 AM 03 COOCHBIHAR BENGALI COOCHBEHAR RAMBHOLA HIGH SCHOOL 10-01-2021 2:00 PM 03 COOCHBIHAR HINDI COOCHBEHAR RAMBHOLA HIGH SCHOOL 10-01-2021 2:00 PM 04 UTTAR DINAJPUR BENGALI A. C INSTITUTION (AKRURMONI CORONATION) (H.S), MALDA 16-01-2021 2:00 PM 04 UTTAR DINAJPUR HINDI A. C INSTITUTION (AKRURMONI CORONATION) (H.S), MALDA 16-01-2021 2:00 PM 04 UTTAR DINAJPUR URDU A. C INSTITUTION (AKRURMONI CORONATION) (H.S), MALDA 16-01-2021 2:00 PM 05 DAKSHIN DINAJPUR BENGALI A. C INSTITUTION (AKRURMONI CORONATION) (H.S), MALDA 16-01-2021 10:00 AM 06 MALDA BENGALI A. C INSTITUTION (AKRURMONI CORONATION) (H.S), MALDA 12-01-2021 10:00 AM 06 MALDA BENGALI A. C INSTITUTION (AKRURMONI CORONATION) (H.S), MALDA 12-01-2021 2:00 PM 06 MALDA BENGALI A. C INSTITUTION (AKRURMONI CORONATION) (H.S), MALDA 13-01-2021 10:00 AM 06 MALDA BENGALI A. -

Government of West Bengal Directorate of Forests Office of the Divisional Forest Officer, Nadia-Murshidabad Division
Government of West Bengal Directorate of Forests Office of the Divisional Forest Officer, Nadia-Murshidabad Division. Krishnagar, Nadia. Pin 741101 [email protected] 03472-252362 E-Tender Notice No: WBFOR/02/NMD/ Ranaghat /NGT Plantation at RanaghatI & Hanskhali / 2019-20 E- TENDER FOR SELECTION OF BONA FIDE PERSONS/AGENCIES/COMPANIES, INCLUDING CONSORTIUM AND PARTNERSHIPFIRMS TO UNDERTAKE PLANTATION OVER 5 HA. at RanaghatI & Hanskhali Block. WITHIN THE JURISDICTION OF BERHAMPORE (N) RANGE, MURSHIDABAD DISTRICT UNDER NADIA MURSHIDABAD DIVISION, WEST BENGAL. The Divisional Forest Officer NADIA-MURSHIDABAD DIVISION, West Bengal invites e-tenders for the following work(s) from the eligible Contractors as detailed in the table below. [Collection (downloading) and Submission (uploading) of Tender can be made online through the website https://wbtenders.gov.in only]. A. List of Work(s): Sl. No. Name of work & Tender Fees & EMD Estimated Amount of Earnest Period of location Payable to Amount Put to Money to be Completion of the tender (Rs.) deposited (Rs.) work 1. Plantation Earnest Money Rs Rs 11880.00 over 5 ha. at may be 593980.00 (2% of the RanaghatI & remitted as per Finance Estimated Hanskhali Department, amount) Block.under Govt. of West the Bengal’s order jurisdiction No. 3975- January, of Ranaghat F(Y) Dated 2020 th Range under 28 July, Nadia 2016. @ 2% of the project Murshidabad cost against Division the project as mentioned in (Attached) the schedule B. Schedule of Dates: Sl Particulars No. 1 Date of uploading N.I.T. Documents—Online( -

Buses from Kolkata to Berhampore, Murshidabad
SL Destination Departure Times Route Calcutta State Transport Corporation [CSTC] (From Dharmatola / Esplanade) Ph : 033-22481916, 033-22482401, 033-22371212 1 Berhampore 06:30 AM, 05:35 PM Barasat-Beldanga 2 Domkal 03:15 PM Berhampore 3 Farakka 10:30 AM, 12:00 PM Barasat-Jagulia-Dhulian 4 Kandhi 10:30 AM Barasat-Jagulia-Krishnagar-Berhampore 5 Maldah 09:30 AM, 12:00 PM, 08:30 PM, 10:00 PM Krishnagar-Berhampore 6 Raghunathgunj 01:45 PM Barasat-Jagulia-Debagram-Berhampore 7 Kaliagunj 01:45 PM Barasat-Berhampore-Maldah 8 Raiganj 06:30 AM, 09:45 AM, 09:30 PM Barasat-Berhampore-Maldah 9 Siliguri (Rocket / Super) 07:00 AM, 04:00 PM, 06:00 PM, 07:00 PM, 08:00 PM Barasat-Berhampore-Maldah-Raiganj North Bengal State Transport Corporation [NBSTC] (From Dharmatola / Esplanade) Ph : 033-22430736, 033-22371806 1 Balurghat (Super) 08:00 PM, 09:00 PM Barasat-Krishnagar-Berhampore-Farakka-Maldah 2 Balurghat (Rocket) 09:30 PM Barasat-Krishnagar-Berhampore-Farakka-Maldah 3 Balurghat 04:45 AM, 08:00 AM Barasat-Krishnagar-Berhampore-Farakka-Maldah 4 Maldah (Rocket) 09:30 PM Barasat-Krishnagar-Berhampore-Farakka-Maldah 5 Maldah 06:00 AM, 10:00 AM Barasat-Krishnagar-Berhampore-Farakka-Maldah 6 Raiganj (Rocket) 09:30 PM Barasat-Krishnagar-Berhampore-Dhulian-Farakka 7 Raiganj (Super) 09:00 PM Barasat-Krishnagar-Berhampore-Dhulian-Farakka 8 Raiganj 06:00 AM, 07:30 AM, 08:30 AM Barasat-Krishnagar-Berhampore-Dhulian-Farakka 9 Siliguri (Express) 06:00 AM Barasat-Krishnagar-Berhampore-Kisangunj-Islampur 10 Siliguri (Rocket) 06:00 PM, 07:00 PM, 08:00 PM Barasat-Krishnagar-Berhampore-Kisangunj-Islampur