A Review of Camera Viewpoint Automation in Robotic and Laparoscopic Surgery
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Automated Staging for Virtual Cinematography Amaury Louarn, Marc Christie, Fabrice Lamarche
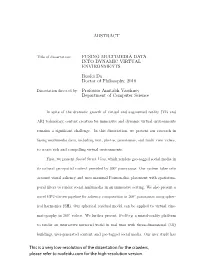
Automated Staging for Virtual Cinematography Amaury Louarn, Marc Christie, Fabrice Lamarche To cite this version: Amaury Louarn, Marc Christie, Fabrice Lamarche. Automated Staging for Virtual Cinematography. MIG 2018 - 11th annual conference on Motion, Interaction and Games, Nov 2018, Limassol, Cyprus. pp.1-10, 10.1145/3274247.3274500. hal-01883808 HAL Id: hal-01883808 https://hal.inria.fr/hal-01883808 Submitted on 28 Sep 2018 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Automated Staging for Virtual Cinematography Amaury Louarn Marc Christie Fabrice Lamarche IRISA / INRIA IRISA / INRIA IRISA / INRIA Rennes, France Rennes, France Rennes, France [email protected] [email protected] [email protected] Scene 1: Camera 1, CU on George front screencenter and Marty 3/4 backright screenleft. George and Marty are in chair and near bar. (a) Scene specification (b) Automated placement of camera and characters (c) Resulting shot enforcing the scene specification Figure 1: Automated staging for a simple scene, from a high-level language specification (a) to the resulting shot (c). Our system places both actors and camera in the scene. Three constraints are displayed in (b): Close-up on George (green), George seen from the front (blue), and George screencenter, Marty screenleft (red). -

Architectural Model for an Augmented Reality Based Mobile Learning Application Oluwaranti, A
Journal of Multidisciplinary Engineering Science and Technology (JMEST) ISSN: 3159-0040 Vol. 2 Issue 7, July - 2015 Architectural Model For An Augmented Reality Based Mobile Learning Application Oluwaranti, A. I., Obasa A. A., Olaoye A. O. and Ayeni S. Department of Computer Science and Engineering Obafemi Awolowo University Ile-Ife, Nigeria [email protected] Abstract— The work developed an augmented students. It presents a model to utilize an Android reality (AR) based mobile learning application for based smart phone camera to scan 2D templates and students. It implemented, tested and evaluated the overlay the information in real time. The model was developed AR based mobile learning application. implemented and its performance evaluated with This is with the view to providing an improved and respect to its ease of use, learnability and enhanced learning experience for students. effectiveness. The augmented reality system uses the marker- II. LITERATURE REVIEW based technique for the registration of virtual Augmented reality, commonly referred to as AR contents. The image tracking is based on has garnered significant attention in recent years. This scanning by the inbuilt camera of the mobile terminology has been used to describe the technology device; while the corresponding virtual behind the expansion or intensification of the real augmented information is displayed on its screen. world. To “augment reality” is to “intensify” or “expand” The recognition of scanned images was based on reality itself [4]. Specifically, AR is the ability to the Vuforia Cloud Target Recognition System superimpose digital media on the real world through (VCTRS). The developed mobile application was the screen of a device such as a personal computer or modeled using the Object Oriented modeling a smart phone, to create and show users a world full of techniques. -

Virtual Cinematography Using Optimization and Temporal Smoothing
Virtual Cinematography Using Optimization and Temporal Smoothing Alan Litteneker Demetri Terzopoulos University of California, Los Angeles University of California, Los Angeles [email protected] [email protected] ABSTRACT disagree both on how well a frame matches a particular aesthetic, We propose an automatic virtual cinematography method that takes and on the relative importance of aesthetic properties in a frame. a continuous optimization approach. A suitable camera pose or path As such, virtual cinematography for scenes that are planned is determined automatically by computing the minima of an ob- before delivery to the viewer, such as with 3D animated films made jective function to obtain some desired parameters, such as those popular by companies such as Pixar, is generally solved manu- common in live action photography or cinematography. Multiple ally by a human artist. However, when a scene is even partially objective functions can be combined into a single optimizable func- unknown, such as when playing a video game or viewing a pro- tion, which can be extended to model the smoothness of the optimal cedurally generated real-time animation, some sort of automatic camera path using an active contour model. Our virtual cinematog- virtual cinematography system must be used. raphy technique can be used to find camera paths in either scripted The type of system with which the present work is concerned or unscripted scenes, both with and without smoothing, at a rela- uses continuous objective functions and numerical optimization tively low computational cost. solvers. As an optimization problem, virtual cinematography has some difficult properties: it is generally nonlinear, non-convex, CCS CONCEPTS and cannot be efficiently expressed in closed form. -

Teaching Visual Storytelling for Virtual Production Pipelines Incorporating Motion Capture and Visual Effects
Teaching Visual Storytelling for virtual production pipelines incorporating Motion Capture and Visual Effects Gregory Bennett∗ Jan Krusey Auckland University of Technology Auckland University of Technology Figure 1: Performance Capture for Visual Storytelling at AUT. Abstract solid theoretical foundation, and could traditionally only be ex- plored through theory and examples in a lecture/lab style context. Film, television and media production are subject to consistent Particularly programs that aim to deliver content in a studio-based change due to ever-evolving technological and economic environ- environment suffer from the complexity and cost-time-constraints ments. Accordingly, tertiary teaching of subject areas such as cin- inherently part of practical inquiry into storytelling through short ema, animation and visual effects require frequent adjustments re- film production or visual effects animation. Further, due to the garding curriculum structure and pedagogy. This paper discusses a structure and length of Film, Visual Effects and Digital Design de- multifaceted, cross-disciplinary approach to teaching Visual Narra- grees, there is normally only time for a single facet of visual nar- tives as part of a Digital Design program. Specifically, pedagogical rative to be addressed, for example a practical camera shoot, or challenges in teaching Visual Storytelling through Motion Capture alternatively a visual effects or animation project. This means that and Visual Effects are addressed, and a new pedagogical frame- comparative exploratory learning is usually out of the question, and work using three different modes of moving image storytelling is students might only take a singular view on technical and creative applied and cited as case studies. Further, ongoing changes in film story development throughout their undergraduate years. -
Fusing Multimedia Data Into Dynamic Virtual Environments
ABSTRACT Title of dissertation: FUSING MULTIMEDIA DATA INTO DYNAMIC VIRTUAL ENVIRONMENTS Ruofei Du Doctor of Philosophy, 2018 Dissertation directed by: Professor Amitabh Varshney Department of Computer Science In spite of the dramatic growth of virtual and augmented reality (VR and AR) technology, content creation for immersive and dynamic virtual environments remains a signifcant challenge. In this dissertation, we present our research in fusing multimedia data, including text, photos, panoramas, and multi-view videos, to create rich and compelling virtual environments. First, we present Social Street View, which renders geo-tagged social media in its natural geo-spatial context provided by 360° panoramas. Our system takes into account visual saliency and uses maximal Poisson-disc placement with spatiotem- poral flters to render social multimedia in an immersive setting. We also present a novel GPU-driven pipeline for saliency computation in 360° panoramas using spher- ical harmonics (SH). Our spherical residual model can be applied to virtual cine- matography in 360° videos. We further present Geollery, a mixed-reality platform to render an interactive mirrored world in real time with three-dimensional (3D) buildings, user-generated content, and geo-tagged social media. Our user study has identifed several use cases for these systems, including immersive social storytelling, experiencing the culture, and crowd-sourced tourism. We next present Video Fields, a web-based interactive system to create, cal- ibrate, and render dynamic videos overlaid on 3D scenes. Our system renders dynamic entities from multiple videos, using early and deferred texture sampling. Video Fields can be used for immersive surveillance in virtual environments. Fur- thermore, we present VRSurus and ARCrypt projects to explore the applications of gestures recognition, haptic feedback, and visual cryptography for virtual and augmented reality. -

Joint Vr Conference of Eurovr and Egve, 2011
VTT CREATES BUSINESS FROM TECHNOLOGY Technology and market foresight • Strategic research • Product and service development • IPR and licensing VTT SYMPOSIUM 269 • Assessments, testing, inspection, certification • Technology and innovation management • Technology partnership • • • VTT SYMPOSIUM 269 JOINT VR CONFERENCE OF EUROVR AND EGVE, 2011. CURRENT AND FUTURE PERSPECTIVE... • VTT SYMPOSIUM 269 JOINT VR CONFERENCE OF EUROVR AND EGVE, 2011. The Joint Virtual Reality Conference (JVRC2011) of euroVR and EGVE is an inter- national event which brings together people from industry and research including end-users, developers, suppliers and all those interested in virtual reality (VR), aug- mented reality (AR), mixed reality (MR) and 3D user interfaces (3DUI). This year it was held in the UK in Nottingham hosted by the Human Factors Research Group (HFRG) and the Mixed Reality Lab (MRL) at the University of Nottingham. This publication is a collection of the industrial papers and poster presentations at the conference. It provides an interesting perspective into current and future industrial applications of VR/AR/MR. The industrial Track is an opportunity for industry to tell the research and development communities what they use the tech- nologies for, what they really think, and their needs now and in the future. The Poster Track is an opportunity for the research community to describe current and completed work or unimplemented and/or unusual systems or applications. Here we have presentations from around the world. Joint VR Conference of -

VR As a Content Creation Tool for Movie Previsualisation
Online Submission ID: 1676 VR as a Content Creation Tool for Movie Previsualisation Category: Application Figure 1: We propose a novel VR authoring tool dedicated to sketching movies in 3D before shooting them (a phase known as previsualisation). Our tool covers the main stages in film-preproduction: crafting storyboards (left), creating 3D animations (center images), and preparing technical aspects of the shooting (right). ABSTRACT previsualisation technologies as a way to reduce the costs by early anticipation of issues that may occur during the shooting. Creatives in animation and film productions have forever been ex- ploring the use of new means to prototype their visual sequences Previsualisations of movies or animated sequences are actually before realizing them, by relying on hand-drawn storyboards, phys- crafted by dedicated companies composed of 3D artists, using tra- ical mockups or more recently 3D modelling and animation tools. ditional modelling/animation tools such as Maya, 3DS or Motion However these 3D tools are designed in mind for dedicated ani- Builder. Creatives in film crews (editors, cameramen, directors of mators rather than creatives such as film directors or directors of photography) however do not master these tools and hence can only photography and remain complex to control and master. In this intervene by interacting with the 3D artists. While a few tools such paper we propose a VR authoring system which provides intuitive as FrameForge3D, MovieStorm or ShotPro [2, 4, 6] or research pro- ways of crafting visual sequences, both for expert animators and totypes have been proposed to ease the creative process [23, 27, 28], expert creatives in the animation and film industry. -

(12) United States Patent (10) Patent No.: US 9,729,765 B2 Balakrishnan Et Al
USOO9729765B2 (12) United States Patent (10) Patent No.: US 9,729,765 B2 Balakrishnan et al. (45) Date of Patent: Aug. 8, 2017 (54) MOBILE VIRTUAL CINEMATOGRAPHY A63F 13/70 (2014.09); G06T 15/20 (2013.01); SYSTEM H04N 5/44504 (2013.01); A63F2300/1093 (71) Applicant: Drexel University, Philadelphia, PA (2013.01) (58) Field of Classification Search (US) None (72) Inventors: Girish Balakrishnan, Santa Monica, See application file for complete search history. CA (US); Paul Diefenbach, Collingswood, NJ (US) (56) References Cited (73) Assignee: Drexel University, Philadelphia, PA (US) PUBLICATIONS (*) Notice: Subject to any disclaimer, the term of this Lino, C. et al. (2011) The Director's Lens: An Intelligent Assistant patent is extended or adjusted under 35 for Virtual Cinematography. ACM Multimedia, ACM 978-1-4503 U.S.C. 154(b) by 651 days. 0616-Apr. 11, 2011. Elson, D.K. and Riedl, M.O (2007) A Lightweight Intelligent (21) Appl. No.: 14/309,833 Virtual Cinematography System for Machinima Production. Asso ciation for the Advancement of Artificial Intelligence. Available (22) Filed: Jun. 19, 2014 from www.aaai.org. (Continued) (65) Prior Publication Data US 2014/O378222 A1 Dec. 25, 2014 Primary Examiner — Maurice L. McDowell, Jr. (74) Attorney, Agent, or Firm — Saul Ewing LLP: Related U.S. Application Data Kathryn Doyle; Brian R. Landry (60) Provisional application No. 61/836,829, filed on Jun. 19, 2013. (57) ABSTRACT A virtual cinematography system (SmartWCS) is disclosed, (51) Int. Cl. including a mobile tablet device, wherein the mobile tablet H04N 5/222 (2006.01) device includes a touch-sensor Screen, a first hand control, a A63F 3/65 (2014.01) second hand control, and a motion sensor. -

VR As a Content Creation Tool for Movie Previsualisation
VR as a Content Creation Tool for Movie Previsualisation Quentin Galvane* I-Sheng Lin Fernando Argelaguet† Tsai-Yen Li‡ Inria, CNRS, IRISA, M2S National ChengChi Inria, CNRS, IRISA National ChengChi France University France University Taiwan Taiwan Marc Christie§ Univ Rennes, Inria, CNRS, IRISA, M2S France Figure 1: We propose a novel VR authoring tool dedicated to sketching movies in 3D before shooting them (a phase known as previsualisation). Our tool covers the main stages in film-preproduction: crafting storyboards (left), creating 3D animations (center images), and preparing technical aspects of the shooting (right). ABSTRACT storyboards or digital storyboards [8] remain one of the most tradi- Creatives in animation and film productions have forever been ex- tional ways to design the visual and narrative dimensions of a film ploring the use of new means to prototype their visual sequences sequence. before realizing them, by relying on hand-drawn storyboards, phys- With the advent of realistic real-time rendering techniques, the ical mockups or more recently 3D modelling and animation tools. film and animation industries have been extending storyboards by However these 3D tools are designed in mind for dedicated ani- exploring the use of 3D virtual environments to prototype movies, mators rather than creatives such as film directors or directors of a technique termed previsualisation (or previs). Previsualisation photography and remain complex to control and master. In this consists in creating a rough 3D mockup of the scene, laying out the paper we propose a VR authoring system which provides intuitive elements, staging the characters, placing the cameras, and creating ways of crafting visual sequences, both for expert animators and a very early edit of the sequence. -

Near-Eye Display and Tracking Technologies for Virtual and Augmented Reality
EUROGRAPHICS 2019 Volume 38 (2019), Number 2 A. Giachetti and H. Rushmeier STAR – State of The Art Report (Guest Editors) Near-Eye Display and Tracking Technologies for Virtual and Augmented Reality G. A. Koulieris1 , K. Ak¸sit2 , M. Stengel2, R. K. Mantiuk3 , K. Mania4 and C. Richardt5 1Durham University, United Kingdom 2NVIDIA Corporation, United States of America 3University of Cambridge, United Kingdom 4Technical University of Crete, Greece 5University of Bath, United Kingdom Abstract Virtual and augmented reality (VR/AR) are expected to revolutionise entertainment, healthcare, communication and the manufac- turing industries among many others. Near-eye displays are an enabling vessel for VR/AR applications, which have to tackle many challenges related to ergonomics, comfort, visual quality and natural interaction. These challenges are related to the core elements of these near-eye display hardware and tracking technologies. In this state-of-the-art report, we investigate the background theory of perception and vision as well as the latest advancements in display engineering and tracking technologies. We begin our discussion by describing the basics of light and image formation. Later, we recount principles of visual perception by relating to the human visual system. We provide two structured overviews on state-of-the-art near-eye display and tracking technologies involved in such near-eye displays. We conclude by outlining unresolved research questions to inspire the next generation of researchers. 1. Introduction it take to go from VR ‘barely working’ as Brooks described VR’s technological status in 1999, to technologies being seamlessly inte- Near-eye displays are an enabling head-mounted technology that grated in the everyday lives of the consumer, going from prototype immerses the user in a virtual world (VR) or augments the real world to production status? (AR) by overlaying digital information, or anything in between on the spectrum that is becoming known as ‘cross/extended reality’ The shortcomings of current near-eye displays stem from both im- (XR). -

Near-Eye Display and Tracking Technologies for Virtual and Augmented Reality
EUROGRAPHICS 2019 Volume 38 (2019), Number 2 A. Giachetti and H. Rushmeier STAR – State of The Art Report (Guest Editors) Near-Eye Display and Tracking Technologies for Virtual and Augmented Reality G. A. Koulieris1 , K. Ak¸sit2 , M. Stengel2, R. K. Mantiuk3 , K. Mania4 and C. Richardt5 1Durham University, United Kingdom 2NVIDIA Corporation, United States of America 3University of Cambridge, United Kingdom 4Technical University of Crete, Greece 5University of Bath, United Kingdom Abstract Virtual and augmented reality (VR/AR) are expected to revolutionise entertainment, healthcare, communication and the manufac- turing industries among many others. Near-eye displays are an enabling vessel for VR/AR applications, which have to tackle many challenges related to ergonomics, comfort, visual quality and natural interaction. These challenges are related to the core elements of these near-eye display hardware and tracking technologies. In this state-of-the-art report, we investigate the background theory of perception and vision as well as the latest advancements in display engineering and tracking technologies. We begin our discussion by describing the basics of light and image formation. Later, we recount principles of visual perception by relating to the human visual system. We provide two structured overviews on state-of-the-art near-eye display and tracking technologies involved in such near-eye displays. We conclude by outlining unresolved research questions to inspire the next generation of researchers. 1. Introduction it take to go from VR ‘barely working’ as Brooks described VR’s technological status in 1999, to technologies being seamlessly inte- Near-eye displays are an enabling head-mounted technology that grated in the everyday lives of the consumer, going from prototype immerses the user in a virtual world (VR) or augments the real world to production status? (AR) by overlaying digital information, or anything in between on the spectrum that is becoming known as ‘cross/extended reality’ The shortcomings of current near-eye displays stem from both im- (XR). -

Design of a Virtual Film Set for Cinematography Practice
Pacific Graphics (2017) Poster Y.-S. Wang and A. Jacobson (Editors) Design of a Virtual Film Set for Cinematography Practice I-Sheng Lin1, Tsai-Yen Li1, Hui-Yin Wu2, and Marc Christie2 1National Chengchi University 2IRISA/INRIA Rennes Bretagne Atlantique Abstract The way scenes and characters are filmed–through the design of camera style, lighting, and color–can completely change the way the audience interprets the story. However, as filmmaking is costly, beginners and amateurs don’t often have the opportunity to experiment on the set. In this work we bring the shooting into a virtual environment, allowing the user to play the roles of the director, cinematographer, and cameraman in a virtual film set. Our system integrates automated camera placement and smart assistance to recommend camera styles for a personalized movie. We conducted a pilot study on amateur users to observe the educational properties of the tool. CCS Concepts •Computing methodologies ! Animation; Virtual reality; 1. Background 2.1. Four Modes of Operation Traditionally, filmmaking is costly, and every second on the set is precious, leaving little time to experiment and make mistakes on The God Perspective mode provides a top-down viewpoint provid- the set. However, with advances in virtual reality, head mounted ing a clear overview of the whole studio, including each actor’s po- displays, and enhanced motion detection techniques, have brought sition, placement of camera, and layout of scene. The God Perspec- us one step closer to developing affordable applications to make tive can help the director have a complete overview of the shooting filmmaking much more approachable to individuals, whether pro- environment.