Case Study 2 – MUDHOLE, ANDHRA PRADESH, INDIA Contents What Can We Learn from Mudhole? 41 1
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Table of Content Page No's 1-5 6 6 7 8 9 10-12 13-50 51-52 53-82 83-93
Table of Content Executive summary Page No’s i. Introduction 1-5 ii. Background 6 iii. Vision 6 iv. Objective 7 V. Strategy /approach 8 VI. Rationale/ Justification Statement 9 Chapter-I: General Information of the District 1.1 District Profile 10-12 1.2 Demography 13-50 1.3 Biomass and Livestock 51-52 1.4 Agro-Ecology, Climate, Hydrology and Topography 53-82 1.5 Soil Profile 83-93 1.6 Soil Erosion and Runoff Status 94 1.7 Land Use Pattern 95-139 Chapter II: District Water Profile: 2.1 Area Wise, Crop Wise irrigation Status 140-150 2.2 Production and Productivity of Major Crops 151-158 2.3 Irrigation based classification: gross irrigated area, net irrigated area, area under protective 159-160 irrigation, un irrigated or totally rain fed area Chapter III: Water Availability: 3.1: Status of Water Availability 161-163 3.2: Status of Ground Water Availability 164-169 3.3: Status of Command Area 170-194 3.4: Existing Type of Irrigation 195-198 Chapter IV: Water Requirement /Demand 4.1: Domestic Water Demand 199-200 4.2: Crop Water Demand 201-210 4.3: Livestock Water Demand 211-212 4.4: Industrial Water Demand 213-215 4.5: Water Demand for Power Generation 216 4.6: Total Water Demand of the District for Various sectors 217-218 4.7: Water Budget 219-220 Chapter V: Strategic Action Plan for Irrigation in District under PMKSY 221-338 List of Tables Table 1.1: District Profile Table 1.2: Demography Table 1.3: Biomass and Live stocks Table 1.4: Agro-Ecology, Climate, Hydrology and Topography Table 1.5: Soil Profile Table 1.7: Land Use Pattern Table -
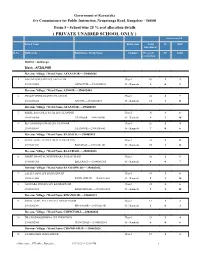
( PRIVATE UNAIDED SCHOOL ONLY ) Seats Reserved
Government of Karnataka O/o Commissioner for Public Instruction, Nrupatunga Road, Bangalore - 560001 Form 5 - School wise 25 % seat allocation details ( PRIVATE UNAIDED SCHOOL ONLY ) Seats reserved School Name Entry class Total SC OBC Enrollment Sl.No DISE Code Habitation / Ward Name Medium 25% seats ST Total reservation District : Gulbarga Block : AFZALPUR Revenue Village / Ward Name AFZALPUR----290402001 1 NAGARAJ BUJARI HPS AFZALPUR Class 1 10 1 2 29040212002 AFZALPUR----29040200101 05 - Kannada 3 0 3 Revenue Village / Ward Name ANOOR----290402004 2 SWAMI VIVEKANAND LPS ANOOR Class 1 42 3 7 29040200403 ANOOR----29040200401 05 - Kannada 11 1 11 Revenue Village / Ward Name ATANOOR----290402005 3 SHREE BASAVRAJ PATIL LPS ATANOOR Class 1 36 3 6 29040200506 ATANOOR----29040200501 05 - Kannada 9 1 10 4 REVANSIDDESHWAR LPS ATANOOR Class 1 26 2 4 29040200507 ATANOOR----29040200501 05 - Kannada 7 0 6 Revenue Village / Ward Name BADADAL----290402011 5 SHREE GURU CHANNAMALLESWAR HPS Class 1 70 5 12 29040201104 BADADAL----29040201101 05 - Kannada 18 1 18 Revenue Village / Ward Name BALURAGI----290402013 6 SHREE SHANTALINGESHWAR LPS BALURAGI Class 1 30 2 5 29040201308 BALURAGI----29040201303 05 - Kannada 8 0 7 Revenue Village / Ward Name BANDARWAD----290402016 7 LALITA DEVI LPS BANDARWAD Class 1 34 3 6 29040201604 BANDARWAD----29040201601 05 - Kannada 9 1 10 8 AKSHARA DHAMA LPS BANDARWAD Class 1 35 3 6 29040201605 BANDARWAD----29040201601 05 - Kannada 9 1 10 Revenue Village / Ward Name BIDANOOR----290402023 9 SHREE GURU PUTTARAJA LPS BIDANOOR Class -

IOCL Proposes to Appoint Retail Outlet Dealers in Karnataka, As Per Following Details
Notice for appointment of Regular/Rular Retail Outlet Dealerships IOCL proposes to appoint Retail Outlet dealers in Karnataka, as per following details: Estimated Fixed Security Location Minimum Dimension (in M)/Area of Site (In Finance to be arranged by the Name of location Revenue District Type of RO Monthly Sales Category Type of Site Mode of selection Fee/Minimum Bid Deposit (Rs Sl.NO Sq M) applicant Potential Amt (Rs in Lakhs) in Lakhs) 1 2 3 4 5 6 7 8 9a 9b 10 11 12 SC /SC CC-1/SC CC-2 /SC PH ST /ST CC-1 /ST CC-2 Estimated Estimated Fund /ST PH Working Capital required for (Regular/ MS + HSD (in (Draw of OBC/OBC CC-1/OBC CC/DC/CFS Frontage Depth Area requirement for development of Rural) KLs) Lots/Bidding) CC-2 /OBC PH operations of RO infrastructure at OPEN/OPEN CC- (Rs. In Lakhs) RO (Rs in Lakhs) 1/OPEN CC-2/OPEN PH DOBASPETE - MUDDALINGANAHALLI (LHS) (DODDABALAPUR 1 BANGALORE RURAL REGULAR 180 SC CFS 35 45 1575 0 0 DRAW OF LOTS 0 3 ROAD) 2 SOMPURA INDUSTRIAL AREA 1ST STAGE BANGALORE RURAL REGULAR 180 SC CFS 20 20 400 0 0 DRAW OF LOTS 0 3 T.BEGUR - NELAMANGALA JAZZ TOLL (LHS) - ON BANGALORE 3 BANGALORE RURAL REGULAR 200 SC CFS 35 45 1575 0 0 DRAW OF LOTS 0 3 PUNE HIGHWAY VISVESVARAPURA-BHAVIKERE(RHS) (NELAMANGALA - 4 BANGALORE RURAL REGULAR 180 SC CFS 35 45 1575 0 0 DRAW OF LOTS 0 3 HASSAN MAIN ROAD, NH) THIPPAGONDANAHALLI - KULUVANAHALLI (RHS) ON 5 BANGALORE RURAL REGULAR 300 SC CFS 35 45 1575 0 0 DRAW OF LOTS 0 3 BANGALORE PUNE HIGHWAY MADDENAHALLI TO CHIKKABELAVANGALA (RHS) (ON 6 BANGALORE RURAL REGULAR 150 ST CFS 35 45 1575 -

District Census Handbook, Gulbarga, Part X-A, B, Series-14
CENSUS OF INDIA 1971 SERIES-14 MYSORE DISTRICT CENSUS HANDBOOK GULBARGA DISTRICT PART X-A: TOWN AND VILLAGE DIRECTORY PART X-B: PRIMARY CENSUS ABSTRACT P. PADMANABHA OF THE INDIAN ADMINISTRATIVE SERVICE DIRECTOR OF CENSUS OPERATIONS MYSORB 24 12 0 24 48 72 MILE:S I I ! I M1f~(o)U ~ I ; i : i 20 0 20 40 60 10 100 kiLOMETRES ADMINISTRATIVE DIVISIONS,I971 STATE 80UNDARY --._- DISTRICT " -.-.--- TALUK " STATE CAPITAL '* DISTRICT HEADQUARTERS (j) TALUK " o T. N....upur - TbirumaIaocUu N ....I ,. H9-Hoo.... pur MAlIARASHTRA " H_~ubU ANDHRA PRADESH TAMIL NADU JAMI MASJID, GULBARGA (Motif on the cover) THE picture illustrated on the cover page is that of Jami Masjid of Gulbarga, built by a Persian architect named Rafi in A.D. 1367, during the reign of Muhammad Shah Baihmani I (1358-1375 A.D.). The architecture of this mosque, although plain, possesses considerable fascination because of the sense of proportion and beauty of line displayed in the building. A novel feature of this mosque is that it has no open court in front of the prayer-hall, and the entire area, consisting of the aisles, the central passages and the prayer-hall is covered over on the model of the mosque of Cordova in Spain. The architect has, in this mosque, given a variety of forms to the arches by adopting different spans and using imposts of various heights. For example, the span of the arches of the aisles is extremely wide in comparison with their imposts, thus producing a new form which later became very popular in the buildings of Bijapur and Bidar. -

Government of Karnataka, Dy.Director for Public Instrictions, Kalaburagi D-Group Attender's Final Seniority List As Per Govt
GOVERNMENT OF KARNATAKA, DY.DIRECTOR FOR PUBLIC INSTRICTIONS, KALABURAGI D-GROUP ATTENDER'S FINAL SENIORITY LIST AS PER GOVT. ORDER NO . DPAR 186 SRS 2018 DT.15/5/2019 OF KALABURAGI DIST AS ON 01-01- 2021 ) C2(4)/114/2020-21 ( Seniority is based on BATCH NO, RECRUITMENT TYPE, DATE OF PROMOTION ,DATE OF ENTRY INTO DIST, DATE OF BIRTH Seniority kgidno name sex schoolname DESIG_NAME Entry to datebirth caste LC-YES / Mode of Taluk No. District date RPC-NO Appointment schoolcode REMARKS District Employeecode HM_date Eligability Date BATCH NO: 1 FROM 01/01/1980 TO 30/06/2020 16/06/1990 YES 1 1138886 MD SALIMODDIN M GHS FARTABAD ATTENDER 01/06/1966 GM COMPENSA GULBARGA SOUTH 24/03/1998 TORY GULBARGA 20 24/03/1998 29040502907 24/09/1988 YES 2 1134790 VIJAY KUMAR M GHS NIBMBARGA ATTENDER 27/11/1969 GM COMPENSA ALAND 26/03/1998 TORY PROMOTED AS SDA GULBARGA 9 26/03/1998 29040109509 09/06/1988 YES 3 1136013 MUSA AHMED M GOVT MPHS * GULBARGA ATTENDER 01/08/1968 GM COMPENSA GULBARGA NORTH 06/08/1998 TORY GULBARGA 16 06/08/1998 29041108514 17/12/1988 YES 4 1139032 KARUNA SAGAR M GOVT HS HARSOOR ATTENDER 01/06/1963 GM COMPENSA GULBARGA NORTH 20/07/1999 TORY REFUSE GULBARGA 18 20/07/1999 29041102308 Monday, April 26, 2021 Page 1 of 8 Seniority kgidno name sex schoolname DESIG_NAME Entry to datebirth caste LC-YES / Mode of Taluk No. District date RPC-NO Appointment schoolcode REMARKS District Employeecode HM_date Eligability Date 03/08/1987 YES 5 1133840 NAZIR AHMED M GHS JAGAT GIRLS GLB ATTENDER 01/06/1963 GM COMPENSA GULBARGA SOUTH 14/06/2006 TORY GULBARGA -

Primary Health Centre List As Per HMIS SR
Primary health centre list as per HMIS SR. DISTRICT NAME SUB DISTRICT FACILITY NAME NO. 1 Bagalkote Badami BELUR (24X7) 2 Bagalkote Badami HALAKURKI (24X7) 3 Bagalkote Badami KAKNUR (24X7) 4 Bagalkote Badami KATAGERI (24X7) 5 Bagalkote Badami KULAGERICROSS (24X7) 6 Bagalkote Badami MUSTIGERI (24X7) 7 Bagalkote Badami NANDIKESHWAR (24X7) 8 Bagalkote Badami PATTDAKAL (24X7) 9 Bagalkote Badami TOGUNSHI (24X7) 10 Bagalkote Bagalkot BENNUR (24X7) 11 Bagalkote Bagalkot BEWOOR (24X7) 12 Bagalkote Bagalkot KALADAGI (24X7) 13 Bagalkote Bagalkot Navnagar UPHC 14 Bagalkote Bagalkot Old city UPHC 15 Bagalkote Bagalkot RAMPUR (24X7) 16 Bagalkote Bagalkot SHIRUR (24X7) 17 Bagalkote Bagalkot SUTAGUNDAR (24X7) 18 Bagalkote Bilagi GALAGALI (24X7) 19 Bagalkote Bilagi KUNDARAGI (24X7) 20 Bagalkote Hunagund AIHOLE (24X7) 21 Bagalkote Hunagund AMEENAGAD (24X7) 22 Bagalkote Hunagund DHANNUR 23 Bagalkote Hunagund GUDUR (24X7) 24 Bagalkote Hunagund HAVARAGI 25 Bagalkote Hunagund HIRESHINGANAGUTTI 24X7 26 Bagalkote Hunagund KAMTAGI (24X7) 27 Bagalkote Hunagund KANDAGAL (24X7) 28 Bagalkote Hunagund KARADI (24X7) 29 Bagalkote Hunagund MAROLA 30 Bagalkote Hunagund NAGUR (24X7) 31 Bagalkote Hunagund P.H.U CHITTARGI 32 Bagalkote Hunagund SULEBHAVI (24X7) Bagalkote Jamakhandi CHIKKALGI CROSS REHIBILITATION 33 CENTRE 34 Bagalkote Jamakhandi CHIMMAD 35 Bagalkote Jamakhandi GOTHE (24X7) 36 Bagalkote Jamakhandi HIPPARAGI (24X7) 37 Bagalkote Jamakhandi Jamkhandi UPHC 38 Bagalkote Jamakhandi KONNUR (24X7) 39 Bagalkote Jamakhandi LINGANUR 24X7 40 Bagalkote Jamakhandi NAVALAGHI 41 Bagalkote Jamakhandi SAVALAGI (24X7) 42 Bagalkote Jamakhandi TERADAL (24X7) 43 Bagalkote Mudhole BELAGALI (24X7) 44 Bagalkote Mudhole HALAGALI (24X7) 45 Bagalkote Mudhole KASABAJAMBAGI (24X7) 46 Bagalkote Mudhole LOKAPURA 24*7 Primary health centre list as per HMIS SR. DISTRICT NAME SUB DISTRICT FACILITY NAME NO. -

Planning for VISION 2020 at the District Level: a Manual
INTERNATIONAL CENTRE FOR EYE HEALTH Planning for VISION 2020 at the District Level A Manual Acknowledgements The preparation of this manual has depended heavily on the advice and support of the key personnel responsible for leading the selected eye care programmes so successfully over recent years. Kitwe Asiwome Seneadza, Medical Director Winston Mbao, Administrator Mudhole Sirigiri Babu Rao, Administrator Shamanna Ramaswamy, Group Leader ICARE Yaruquí Felipe Chiriboga, Medical Director María Agusta Vega, Administrator My gratitude respects the time devoted to my enquiries, both while visiting their eye care centres and also their patience and care in meeting my many subsequent e-mail requests. I hope that what I have written represents clearly and accurately the wise and whole-hearted commitment of these project leaders and their teams to the development of community eye health for their local communities. I also wish to acknowledge the support of Allen Foster and many colleagues at ICEH who have made very helpful suggestions as the work has progressed. Graham Dyer December 2006 ISBN 1 - 90 - 2541 - 20 - 0 Planning for VISION 2020 at the District Level A Manual Graham Dyer ICEH Preface VISION 2020: The Right to Sight was launched by WHO in February 1999. In the intervening seven years national governments and non-governmental organisations have progressively accepted this initiative as the best approach for improving eye health and preventing blindness. The realisation of VISION 2020 requires a commitment to develop programmes serving populations at the district level, where needs can be assessed, resources identified and community support motivated. While the need for district planning is clear, the means of bringing this about is more difficult to define. -
Adilabad District, Andhra Pradesh
For Official Use Only CENTRAL GROUND WATER BOARD MINISTRY OF WATER RESOURCES GOVERNMENT OF INDIA GROUND WATER BROCHURE ADILABAD DISTRICT, ANDHRA PRADESH SOUTHERN REGION HYDERABAD September 2013 CENTRAL GROUND WATER BOARD MINISTRY OF WATER RESOURCES GOVERNMENT OF INDIA GROUND WATER BROCHURE ADILABAD DISTRICT, ANDHRA PRADESH (AAP-2012-13) BY DR. PANDITH MADHNURE SCIENTIST-C SOUTHERN REGION BHUJAL BHAWAN, GSI Post, Bandlaguda NH.IV, FARIDABAD -121001 Hyderabad-500068 HARYANA, INDIA Andhra Pradesh Tel: 0129-2418518 Tel: 040-24225201 Gram: Bhumijal Gram: Antarjal GROUND WATER BROCHURE ADILABAD DISTRICT, ANDHRA PRADESH DISTRICT AT A GLANCE C O N T E N T S Chapter Content No. 1 INTRODUCTION 1.1 General 1.2 Demography 1.3 Physiography 1.4 Geomorphology 1.5 Drainage 1.6 Soils 1.7 Flora and Fauna 1.8 Land Use and Land Cover 1.9 Cropping pattern (2009-2010) 1.10 Size of agricultural holdings 1.11 Economic Minerals 1.12 Previous Studies by CGWB 1.13 Places of tourist importance 2 CLIMATE 3 HYDROLOGY 3.1 Major Irrigation Projects (Capacity > 10000 Ha) 3.2 Medium Irrigation Projects (Capacity > 2000-10000 Ha) 3.3 Minor Irrigation Projects (Capacity > 40-2000 and <40 ha) 3.4 Ground Water Irrigation 4 HYDROGEOLOGICAL SET-UP 4.1 Geology 4.2 Occurrence and Movement of Ground water 4.2.1 Consolidated Rocks 4.2.2 Semi-consolidated formations 4.2.3 Unconsolidated formations 4.3 Depth to Water Level (DTW) 4.3.1 Pre-monsoon (May-2011) 4.3.2 Post-monsoon (November-2011) 4.4 Water level fluctuation (WLF) (Pre and Post-monsoon season-2011) 4.5 Decadal Water Level Trends (2002-2011): 5 GROUND WATER RESOURCES (As on 2008-09) 6 GROUND WATER QUALITY 7 GROUND WATER DEVELOPMENT& MANAGEMENT 7.1 Ground Water Development 7.2 Ground Water Management 7.3 Ground Water Issues 8 RECOMMENDATIONS Acknowledgements LIST OF FIGURES Figure-1 Administrative map of Adilabad District, A.P. -

Census of India 2011
Census of India 2011 KARNATAKA SERIES-30 PART XII-A DISTRICT CENSUS HANDBOOK GULBARGA VILLAGE AND TOWN DIRECTORY DIRECTORATE OF CENSUS OPERATIONS KARNATAKA © Government of India copyright, 2014. The maps included in this publication are under © Government of India copyright, 2014. The responsibility for the correctness of internal details rests with the publisher. The territorial water of India extend into the sea to a distance of twelve nautical miles measured from the appropriate base line. The external boundaries and coastlines of India agree with the Record/Master Copy certified by Survey of India. CENSUS OF INDIA 2011 KARNATAKA SERIES-30 PART XII-A DISTRICT CENSUS HANDBOOK GULBARGA VILLAGE AND TOWN DIRECTORY DIRECTORATE OF CENSUS OPERATIONS KARNATAKA Motif THE GULBARGA FORT The Gulbarga Fort is located in Gulbarga City. The fort lieved, yet there is a continuous parapet of merlons, raised at Gulbarga, originally built by Raja Gulchand and after- over the gateways, provided with narrow openings from wards strengthened by Ala-ud-din Bahmani, is a fine work, which to fire muskets. Within the centre of the fort, is situ- containing 15 bastions and 26 guns, one of which is 25 ft. ated a great mosque 216 ft. by 176 ft. large enough to ac- long. The walls 16 cm. thick are frequently punctuated by commodate about five thousand worshippers and is the semi – circular bastions and surrounded by a 30m. wide only one of its kind in India built by Rafi, son of shams from moat. The Principal gateways on the East and the West Qazsvin in Iran in 1367 A.D., the mosque is entered from the sides consist of pointed arched openings flanked by bas- north and has arched halls on all sides except the west. -

Secondary Glb Pdf
Office of Deputy Director of Public Instruction Gulbarga List of Govt Secondary Schools having Potable Drinking water Name of the District : Gulbarga Sl School Dise Availability Name of the Block Name of the School Released Under Scheme Amount No code/ Number Drinking Water 1 AFZALPUR 29040202502 HS BOSAGA YES RMSA 0.7 2 AFZALPUR 29040203605 HS GATTARAGA YES RMSA 0.7 3 AFZALPUR 29040204503 HS HASARAGUNDAGI YES PANCH SOULABHYA 0.7 4 AFZALPUR 29040202303 HS BIDANOOR YES SDP 0.7 5 AFZALPUR 29040200505 HS URDU ATANOOR YES SDP 0.7 6 AFZALPUR 29040203605 HS DESAI KALLUR YES PANCH SOULABHYA 0.7 7 ALAND GHS SUNTANUR YES SDP 0.7 8 ALAND GHS V.K.SALAGAR YES PANCH SOULABHYA 0.7 9 ALAND GHS SARASAMBA YES SDP 0.7 10 ALAND GHS JIDAGA YES SDP 0.7 11 ALAND GHS NIMBARGA YES SDP 0.7 12 ALAND GHS DARGA SIROOR YES SDP 0.7 13 ALAND GHS BASAVANSANGOLGI YES SDP 0.7 14 CHINCHOLI 0305504 GHS KALLUR ROAD YES PANCH SOULABHYA 0.7 15 CHINCHOLI 0301708 GHS CHENGTA YES PANCH SOULABHYA 0.7 16 CHINCHOLI 0304302 GHS HASARGUNDGI YES PANCH SOULABHYA 0.7 17 CHINCHOLI 0305802 GHS KEROLLI YES PANCH SOULABHYA 0.7 18 CHINCHOLI 0309502 GHS RAIKOD YES PANCH SOULABHYA 0.7 19 CHINCHOLI 0310704 GHS SHADIPUR YES PANCH SOULABHYA 0.7 20 CHINCHOLI 0309807 GHS RATKAL YES PANCH SOULABHYA 0.7 21 CHINCHOLI 0303602 GHS GARAGPALLI YES PANCH SOULABHYA 0.7 22 CHINCHOLI 0311308 GHS SULEPET YES SDP 0.7 23 CHINCHOLI 0311309 GHS SULEPET GIRLS YES PANCH SOULABHYA 0.7 24 CHINCHOLI 0311310 GHS SULEPET URDU YES PANCH SOULABHYA 0.7 25 CHINCHOLI UPGRADED GHS SALEBEERANALLI YES PANCH SOULABHYA 0.7 26 CHINCHOLI -

Sc/St Backlog -2018)
PROVISIONAL COMMON LIST OF JUNIOR ASSISTANTS (SC/ST BACKLOG -2018) Local / Application Name of the Father / Qualification Total Marks Percentag Male/ Mobile Date of Birth Caste Non District Full Address of the applicant DISTRICT Remarks Sl.No. Applicant Spouse Name ( Category ) Marks obtained e Female Number Local H.NO 7-65/3/2, VIDYANAGAR, 1 UYKE YOGESHWER BALIRAM 05.08.1991 B.Pharmacy 6025 3490 57.93 M ST Local Adilabad BESIDE SATOSHIMATHA TEMPALE ADILABAD 9533378080 ICHODA, ADILABAD H.NO 1-1-86 NEAR ERODRAM SRI MAMIDI VAISHALI LAXMAN 10.06.1995 B.Sc 2200 1601 72.77 F SC Local Adilabad ADILABAD 9059386119 2 RAM COLONY ADILABAD H.NO 2-104/12, VILL & MDL BALIRAM A VITTAL 15.06.1986 B.Sc 2200 1105 50.23 M ST Local Adilabad ADILABAD 7993792754 3 BHEEMPUR DIST ADILABAD MUKKERA MUKKERA H.NO 4-65 VILL PENDALWADA I TO X BONAFIDES NOT 13.01.1996 B.Sc 2200 1383 62.86 M SC Local Adilabad ADILABAD 9676515592 4 SANTOSH BORRANNA MDL JAINATH ADILABAD SUBMITTED KUMRA ANIL KUMRA KESHAV H.NO 1-11 VILL CHINCHUGHAT, 20.06.1994 BA 1600 679 42.44 M ST Local Adilabad ADILABAD 7013965771 5 KUMAR RAO ADILABAD H.NO 8-29, VILL SHANKAR TANDA I TO IV BONAFIDES NOT 6 JADHAV SATEESH JADHAV BHIKKU 03.05.1992 B.Tech 5200 2962 56.96 M ST Local Adilabad HASNAPUR MDL UTNOOR ADILABAD 9542906066 ADILABAD SUBMITTED T. SARVESHWAR H.NO 2-4-267/1, KOLIPURA I TO III BONAFIDES NOT T.SRINIVAS 12.02.1985 BA 1600 781 48.81 M SC Local Adilabad ADILABAD 9949867303 8 RAO COLONY ADILABAD SUBMITTED MANDA PRAVEEN H.NO 4-106 VILL KONDAPUR MDL SHANKAR 03.08.1989 B.Com 1900 942 49.58 M SC -

Government of Karnataka Provisional Habitation Wise Neighbourhood
Government of Karnataka O/o Commissioner for Public Instruction, Nrupatunga Road, Bangalore - 560001 RURAL Provisional Habitation wise Neighbourhood Schools - 2016 ( RURAL ) Habitation Name School Code Management Lowest Highest Entry type class class class Habitation code / Ward code School Name Medium Sl.No. District : Gulbarga Block : ALAND Habitation : --- 29040110805 Govt. 1 8 Class 1 GOVT HPS SANGOLAGI (G ) 05 - Kannada 1 29040110803 Govt. 1 5 Class 1 GOVT LPS SANGOLAGI TANDA 05 - Kannada 2 29040110806 Govt. 1 5 Class 1 GOVT LPS SNGOLAGI(G)3 05 - Kannada 3 29040110802 Govt. 1 5 Class 1 GOVT LPS SANGOLAGI KEREHOSAHAT 05 - Kannada 4 29040117305 Pvt Unaided 1 6 Class 1 JNANA DIKSHS HPS VENKATESH NAGAR 05 - Kannada 5 29040116901 Pvt Unaided 1 5 Class 1 AL-QUALAM LPS (URDU) ALAND 18 - Urdu 6 29040110810 Pvt Unaided 1 10 Class 1 VIVEKAVARDHINI HPS KORALLI CROSS 19 - English 7 29040117202 Pvt Unaided 1 7 Class 1 MMJ URDU HPS ALAND 18 - Urdu 8 Habitation : ALANGA---29040100201 29040100201 29040100201 Govt. 1 8 Class 1 ALANGA GOVT HPS ALANGA 10 - Marathi 9 29040100201 29040100202 Govt. 1 5 Class 1 ALANGA GLPS ALANGA (K) 05 - Kannada 10 29040100201 29040100204 Pvt Unaided 1 5 Class 1 ALANGA SHREE SARASWATI LPS ALANGA 05 - Kannada 11 Habitation : ALUR (B)---29040100501 29040100501 29040100502 Govt. 1 8 Class 1 ALUR (B) GOVT HPS ALOOR (B) 05 - Kannada 12 Habitation : AMBALGA---29040100601 29040100601 29040100604 Govt. 1 5 Class 1 AMBALGA GLPS AMBALGA URDU 18 - Urdu 13 29040100601 29040100606 Govt. 1 7 Class 1 AMBALGA GHPS AMBALGA 05 - Kannada 14 29040100601 29040100607 Pvt Unaided 1 6 Class 1 e-Governance, CPI office, Bangalore 2/22/2016 -5:39:28 PM 1 Government of Karnataka O/o Commissioner for Public Instruction, Nrupatunga Road, Bangalore - 560001 RURAL Provisional Habitation wise Neighbourhood Schools - 2016 ( RURAL ) Habitation Name School Code Management Lowest Highest Entry type class class class Habitation code / Ward code School Name Medium Sl.No.