Mohammad Mumtaz Khan 2000-Ag-1404
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Water and Power Resources of West Pakistan
Water and Power Resources PAKISTAN "& of WEST I1158 Public Disclosure Authorized A Study in Sector Planning g' c - J) A N D e XJ ~~~~~~~ S >>)~~~~~TM RHELA AS H M I R Public Disclosure Authorized VISLAMABA > 2 t \ . Public Disclosure Authorized C ,,'_ o / z 'N ~~VOLUME g,_ -THE MAIN REPORT \ < ,pre~lppared by a World Bank Study Group Headed by X f .,/ ~~~PIETER LIEFTINCK t i '_z ~~~A. ROBERT SADOVE Public Disclosure Authorized tt I ~~~~~~~~~Deputy Hlead S n THOMAS-4 C.CREYKE ~~~~< < /r~~~~~~~~~~~trigation and Agr-icultut-e WATER AND POWER RESOURCES OF WEST PAKISTAN A Study in Sector Planning Volume I: The Main Report $10.00 Volume II: The Development of Irrigation and Agriculture $12.50 Volume III: Background and Methodology $ 12.50 $28.50 the set Prepared by a World Bank Study Group Headed by Pieter Lieftinck; A. Robert Sadove, Deputy Head; Thomas C. Creyke, Irrigation and Agriculture. Without doubt, the greatest single co- ordinated development operation in which the World Bank has been involved is the massive program for development of the Indus Basin. This pioneering study is an integral part of that project and is unique both in its conceptualization and its compre- hensiveness. It demonstrates the feasibility of a new and more rigorous approach to resource planning and development and will serve as an indispensible model for engi- neers, economists, and planners for years to come. Focal points of the Study are the Indus River, which runs the length of west Paki- stan, several of its tributaries, and a huge natural underground reservoir. -

Weekly Epidemiological Bulletin Disease Early Warning System and Response in Pakistan
Weekly Bulletin Epidemiological Disease early warning system and response in Pakistan Volume 3, Issue 15, Wednesday 18 April 2012 Highlights Priority diseases under surveillance Epidemiological week no. 15 (8 to 14 April 2012) in DEWS Acute (Upper) Respiratory Infection • In week 15, 2012, total 82 districts including 3 agencies provided surveillance data to the Pneumonia DEWS on weekly basis from around 2,010 health facilities. Data from mobile teams is reported Suspected Diphtheria through sponsoring BHU or RHC. Suspected Pertussis Acute Watery Diarrhoea Bloody diarrhoea • A total of 684,278 consultations were reported through DEWS of which 19% were acute Other Acute Diarrhoea respiratory infections (ARI); 8% were acute diarrhoea; 4% were suspected malaria; while 4% were Suspected Enteric/Typhoid Fever Skin disease. Suspected Malaria Suspected Meningitis Suspected Dengue fever • A total of 247 alerts reported while 27 outbreaks were identified in week 15, 2012: Alto‐ Suspected Viral Hemorrhagic Fever gether 142 alerts for Measles; 30 for Leishmaniasis; 16 for NNT and Tetanus; 12 for Typhoid; 11 Pyrexia of Unknown Origin for Pertussis; 9 for acute diarrhoea; 7 for Scabies; 5 for ARI; 4 for Acute jaundice syndrome; 3 for Suspected Measles Suspected Acute Viral Hepatitis AWD; 2 each for Bloody diarrhoea and Diphtheria; while 1 each for CCHF, HF, Food poisoning and Chronic Viral Hepatitis Chicken Pox. Neonatal Tetanus Acute Flaccid Paralysis • In this week no new polio cases was reported. As of 16 April 2012, the total number of polio Scabies Cutaneous Leishmaniasis cases confirmed by the laboratory is 15 from 10 districts/towns/tribal agencies and areas. -
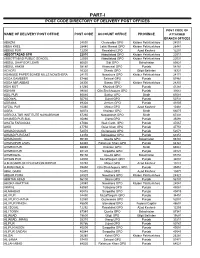
Part-I: Post Code Directory of Delivery Post Offices
PART-I POST CODE DIRECTORY OF DELIVERY POST OFFICES POST CODE OF NAME OF DELIVERY POST OFFICE POST CODE ACCOUNT OFFICE PROVINCE ATTACHED BRANCH OFFICES ABAZAI 24550 Charsadda GPO Khyber Pakhtunkhwa 24551 ABBA KHEL 28440 Lakki Marwat GPO Khyber Pakhtunkhwa 28441 ABBAS PUR 12200 Rawalakot GPO Azad Kashmir 12201 ABBOTTABAD GPO 22010 Abbottabad GPO Khyber Pakhtunkhwa 22011 ABBOTTABAD PUBLIC SCHOOL 22030 Abbottabad GPO Khyber Pakhtunkhwa 22031 ABDUL GHAFOOR LEHRI 80820 Sibi GPO Balochistan 80821 ABDUL HAKIM 58180 Khanewal GPO Punjab 58181 ACHORI 16320 Skardu GPO Gilgit Baltistan 16321 ADAMJEE PAPER BOARD MILLS NOWSHERA 24170 Nowshera GPO Khyber Pakhtunkhwa 24171 ADDA GAMBEER 57460 Sahiwal GPO Punjab 57461 ADDA MIR ABBAS 28300 Bannu GPO Khyber Pakhtunkhwa 28301 ADHI KOT 41260 Khushab GPO Punjab 41261 ADHIAN 39060 Qila Sheikhupura GPO Punjab 39061 ADIL PUR 65080 Sukkur GPO Sindh 65081 ADOWAL 50730 Gujrat GPO Punjab 50731 ADRANA 49304 Jhelum GPO Punjab 49305 AFZAL PUR 10360 Mirpur GPO Azad Kashmir 10361 AGRA 66074 Khairpur GPO Sindh 66075 AGRICULTUR INSTITUTE NAWABSHAH 67230 Nawabshah GPO Sindh 67231 AHAMED PUR SIAL 35090 Jhang GPO Punjab 35091 AHATA FAROOQIA 47066 Wah Cantt. GPO Punjab 47067 AHDI 47750 Gujar Khan GPO Punjab 47751 AHMAD NAGAR 52070 Gujranwala GPO Punjab 52071 AHMAD PUR EAST 63350 Bahawalpur GPO Punjab 63351 AHMADOON 96100 Quetta GPO Balochistan 96101 AHMADPUR LAMA 64380 Rahimyar Khan GPO Punjab 64381 AHMED PUR 66040 Khairpur GPO Sindh 66041 AHMED PUR 40120 Sargodha GPO Punjab 40121 AHMEDWAL 95150 Quetta GPO Balochistan 95151 -

Government of Khyber Pakhtunkhwa
GOVERNMENT OF KHYBER PAKHTUNKHWA COMMUNICATION AND WORK DEPARTMENT TENDER NOTICE (Single stage two envelope procedure) C&W Department (C&W Division Kohat) Government of Khyber Pakhtunkhwa invites electronic Bids from the eligible firms/bidders in accordance with KPPRA Procurement rules 2014 on single stage two envelope procedure for the following works. S.N Name of work. Required Estimated Bid security Period of Last date of Date of Date of category Cost i/c Stamp Completion submission opening of opening of of PEC & duty and time. Technical Financial relevant Bid. Bid. codes/ enlistmen t category ADP No. 1703/200248 (2020- 21) Construction of 1. Technically & Economically Feasible 60-KMs Roads in Kohat Division. S.H: Construction/ Improvement/ 21.12.2020 On the i. Widening of Lachi Dartapi C-5/PK-5 46.860 0.956 (M) As per at 12.00 same day (M) work order Hours & time. Road (3.3-KM) PK-81 District Kohat. Construction of Black Topped ii. Road from Fazal Abad to C-6/PK-6 21.345 0.446 -do- -do- -do- Momin Abad UC Jarma (1.76- (M) (M) KM) PK-81 District Kohat. Date of Construction/ Improvement/ opening of Widening of Black Topped financial C-6/PK-6 bid will be iii. Road from Speena Bangla to 24.581 0.511 -do- -do- -do- (M) (M) announced Haji Dawood Khan Koroona after the (2-KM) PK-81 District Kohat. approval Construction of Black Topped of iv. C-5/PK-5 25.076 0.502 -do- -do- -do- technical Road from Highway to Surgul bid from (M) (M) (2-KM) PK-81 District Kohat. -

WHO Emergency Humanitarian Program Situation Report
WHO Emergency Humanitarian Program Situation Report Khyber Pakhtunkhwa and FATA Week 17 Date: April 22-28, 2012 1. Situation around IDP hosting districts A: Situation in “Jalozai” IDP camp, Nowshera district WHO shares updates on the disease situation on the newly influx of IDPs of Jalozai IDP camp with health cluster partners on district, provincial and national levels. WHO along with health cluster partners, UNICEF and provincial health authorities lead the emergency health response for the newly displaced IDPs in Jalozai camp and living in host communities in District Nowshera. Till 28th April, 2012, total IDPs population in KPK and FATA are 148,593families with 689007 individuals. Out of 148,593 families 41745 families are residing in host communities. 6215 families are residing in Jalozai IDP camp. In total Jalozai camp host 11,350 families with 53 970 individuals. This includes the new influx for Khyber and old caseload of Khyber and Bajaur Agencies. A total of 39 families with 173 individuals were registered on 28th April, 2012. Out of which 35 families with 156 individuals opted to live outside the camp and 4 families with 17 individuals elected to reside in Jalozai CAMP. Elsewhere in KP and FATA return has continued with more than 1000 families returning to South Waziristan. A total of 8 alerts including 6 measles and 2 AFP were reported and responded in this week. There were 6,704 consultations provided through health care provider, including acute respiratory infection (19% or 1,271 cases), acute diarrhoea (9.3% or 621 cases), skin infection (2% or 114) and suspected malaria (1% or 39 cases). -

KT15D00002-Repair Approach Street Dispensary Mirahmad Khel 220,000 220,000 220,000 220,000
District Project Description BE 2017-18 Final Budget Releases Expenditure KOHAT KT15D00002-Repair approach street dispensary MirAhmad khel 220,000 220,000 220,000 220,000 KOHAT KT15D00003-Const of Toilets, waiting shed andother 740,000 740,000 740,000 740,000 repair/maintenance of BHU Sherkot KOHAT KT15D00004-Pipe Line at BHU LandiKachai, Repair ofroof of RHC 649,000 649,000 649,000 649,000 UstarZai, Repair Work at RHC Usterzai. KOHAT KT15D00005-Maj; repair, w/s and elect, BHU KhaddarKhel 423,892 423,892 423,892 423,892 KOHAT KT15D00006-R&(M) works, const of waiting shed andG/Lat 04 No. 740,000 740,000 740,000 740,000 at RHC Lachi Bala KOHAT KT15D00007-R&(M) at BHU Ali Kach 740,000 740,000 740,000 740,000 KOHAT KT15D00008-Elect, W/S, Sanitary and building repairBHU Dolli 596,291 596,291 596,291 596,291 Banda KOHAT KT15D00009-Prov; of health related equipments andhygienic kits in 740,000 740,000 740,000 - civil hospital Shakardara Urban. Dev; works at civilHospital Shakardara. KOHAT KT15D00010-Solarization at BHU Gabari in U/CShakardara Rural-II. 740,000 740,000 740,000 - KOHAT KT15D00011-Major Repair of buildings and w/s of BHUGabari 740,000 740,000 740,000 740,000 KOHAT KT15D00012-Const;/repair works and S/F of Hand Pumpat BHU 488,122 488,122 488,122 488,122 Surgul KOHAT KT15D00013-Pavement of Dispensary street at U/CUrban III 507,090 507,090 507,090 507,000 KOHAT KT15D00014-Purchase of Hygienic kits,Purchase ofHematology 3,981,535 3,981,535 3,981,535 1,204,000 analyzer, for LMH Kohat, Purchase of Spray Pumps andInsecticides KOHAT KT15D00015-Const: -

1. Introduction the Punjab Urial Ovis Vignei Punjabiensis Is Endemic to Northern Punjab, Pakistan, and Is Currently Classified As Endangered by the IUCN
Survey of the status, distribution and home range requirements of the Punjab Urial 1. Introduction The Punjab urial Ovis vignei punjabiensis is endemic to northern Punjab, Pakistan, and is currently classified as endangered by the IUCN. The distribution of the animal in Pakistan is between the Indus and Jhelum rivers at elevations of 250 -1,500 m primarily in the Kala Chitta and Salt Ranges. The dominant habitat type in the area is dry sub-tropical, semi-evergreen scrub forest. Punjab urial were once present over all northern Punjab Mountains, but in recent decades underwent a severe decline in both range and numbers, disappearing from much of their historic range. The main reasons for the rapid decline in numbers appear to be poaching, the capture of newborn lambs that are kept as pets, fragmentation of home ranges, competition with domestic livestock and habitat disturbance and destruction associated with increasing agriculture, forestry and mining. In addition, infusion of exotic but compatible mouflon sheep genes may have occurred. The recent construction of the M-2 Motorway between Islamabad and Lahore created a substantial barrier to seasonal migrations and to dispersal. The main factors affecting the continued persistence of the wild population are inadequate protection against poaching and habitat loss. Initial conservation measures should include, increasing the law enforcement capabilities, to incorporate community participation in the management of urial and reduce the number of competing livestock. The present study is also as an attempt to collect basic ecological information on the urial in the Salt Range area. The overall aim of the project is to accurately determine the status and distribution of the Punjab urial throughout its current home range in northern Punjab and to determine what its ideal habitat requirements are. -

R Functional 2 332101 BHU Barh Kohat
DISTRICT KOHAT BASIC HEALTH UNIT S.No ID No Institute Name Tehsil Class Beds Locality Status 1 332099 BHU Ali Kach Lachi 1 - R Functional 2 332101 BHU Barh Kohat 1 - R Functional 3 332100 BHU Bazid Khel Kohat 1 - R Functional 4 332023 BHU Dhoda Kohat 1 - R Functional 5 332024 BHU Gabari Lachi 1 - R Functional 6 332026 BHU Kachai Kohat 1 - R Functional 7 332027 BHU Khaddar Khel Lachi 1 - R Functional 8 332028 BHU Marai Payan Kohat 1 - R Functional 9 332029 BHU Mohammad Zai Kohat 1 - R Functional 10 332030 BHU Nakband Kohat 1 - R Functional 11 332031 BHU Pershai Kohat 1 - R Functional 12 332033 BHU Shawaki Lachi 1 - R Functional 13 332035 BHU Suleman Talab Kohat 1 - R Functional 14 332036 BHU Sumari Payan Lachi 1 - R Functional 15 332037 BHU Togh Bala Kohat 1 - R Functional 16 332038 BHU Toolang Kohat 1 - R Functional 17 332039 BHU Ziarat Shaikh Aladad Kohat 1 - R Functional 18 332041 BHU Duli Banda Lachi 1 - R Functional 19 332042 BHU Kamal Khel Kohat 1 - R Functional 20 332045 BHU Sher Kot Kohat 1 - R Functional DISPENSARY 1 332050 Civil Dispy. Bezadi chikar kot Kohat 1 - U Functional 2 332052 Civil Dispy. Dartappi Lachi 1 - R Functional 3 332053 Civil DispY: Garhi mawaz khan Kohat 1 - R Functional 4 332054 Civil Dispy: Jangle khel kohat Kohat 1 - U Functional 5 332055 Civil Dispy: Kharmatoo Kohat 1 - R Functional 6 332056 Civil Dispy: Shadi khel Kohat 1 - R Functional 7 332057 Civil Dispy: Shadi pur Kohat 1 - R Functional 8 332064 Urban Dispy: Mir ahmad khel Kohat 1 - U Functional 9 332065 Urban Dispy: Lachi Lachi 1 - U Functional 10 -

1 Annexure - D Names of Village / Neighbourhood Councils Alongwith Seats Detail of Khyber Pakhtunkhwa
1 Annexure - D Names of Village / Neighbourhood Councils alongwith seats detail of Khyber Pakhtunkhwa No. of General Seats in No. of Seats in VC/NC (Categories) Names of S. Names of Tehsil Councils No falling in each Neighbourhood Village N/Hood Total Col Peasants/Work S. No. Village Councils (VC) S. No. Women Youth Minority . district Council Councils (NC) Councils Councils 7+8 ers 1 2 3 4 5 6 7 8 9 10 11 12 13 Abbottabad District Council 1 1 Dalola-I 1 Malik Pura Urban-I 7 7 14 4 2 2 2 2 Dalola-II 2 Malik Pura Urban-II 7 7 14 4 2 2 2 3 Dabban-I 3 Malik Pura Urban-III 5 8 13 4 2 2 2 4 Dabban-II 4 Central Urban-I 7 7 14 4 2 2 2 5 Boi-I 5 Central Urban-II 7 7 14 4 2 2 2 6 Boi-II 6 Central Urban-III 7 7 14 4 2 2 2 7 Sambli Dheri 7 Khola Kehal 7 7 14 4 2 2 2 8 Bandi Pahar 8 Upper Kehal 5 7 12 4 2 2 2 9 Upper Kukmang 9 Kehal 5 8 13 4 2 2 2 10 Central Kukmang 10 Nawa Sher Urban 5 10 15 4 2 2 2 11 Kukmang 11 Nawansher Dhodial 6 10 16 4 2 2 2 12 Pattan Khurd 5 5 2 1 1 1 13 Nambal-I 5 5 2 1 1 1 14 Nambal-II 6 6 2 1 1 1 Abbottabad 15 Majuhan-I 7 7 2 1 1 1 16 Majuhan-II 6 6 2 1 1 1 17 Pattan Kalan-I 5 5 2 1 1 1 18 Pattan Kalan-II 6 6 2 1 1 1 19 Pattan Kalan-III 6 6 2 1 1 1 20 Sialkot 6 6 2 1 1 1 21 Bandi Chamiali 6 6 2 1 1 1 22 Bakot-I 7 7 2 1 1 1 23 Bakot-II 6 6 2 1 1 1 24 Bakot-III 6 6 2 1 1 1 25 Moolia-I 6 6 2 1 1 1 26 Moolia-II 6 6 2 1 1 1 1 Abbottabad No. -

Indian Soldiers Died in Italy During World War II: 1943-45
Indian Soldiers died in Italy during World War II: 1943-45 ANCONA WAR CEMETERY, Italy Pioneer ABDUL AZIZ , Indian Pioneer Corps. Gurdaspur, Grave Ref. V. B. 1. Sepoy ABDUL JABAR , 10th Baluch Regiment. Hazara, Grave Ref. V. B. 4. Sepoy ABDUL RAHIM , 11th Indian Inf. Bde. Jullundur, Grave Ref. V. D. 6. Rifleman AITA BAHADUR LIMBU , 10th Gurkha Rifles,Dhankuta, Grave Ref. VII. D. 5. Sepoy ALI GAUHAR , 11th Sikh Regiment. Rawalpindi, Grave Ref. V. D. 4. Sepoy ALI MUHAMMAD , 11th Sikh Regiment, Jhelum, Grave Ref. V. B. 6. Cook ALLAH RAKHA , Indian General Service Corps,Rawalpindi, Grave Ref. III. L. 16. Sepoy ALTAF KHAN , Royal Indian Army Service Corps,Alwar, Grave Ref. V. D. 5. Rifleman ANAND KHATTRI, 2nd King Edward VII's Own Gurkha Rifles (The Sirmoor Rifles). Grave Ref. VII. B. 7. Sapper ARUMUGAM , 12 Field Coy., Queen Victoria's Own Madras Sappers and Miners. Nanjakalikurichi. Grave Ref. V. B. 2. Rifleman BAL BAHADUR ROKA, 6th Gurkha Rifles. , Grave Ref. VII. B. 5. Rifleman BAL BAHADUR THAPA, 8th Gurkha Rifles.,Tanhu, , Grave Ref. VII. D. 8. Rifleman BHAGTA SHER LIMBU , 7th Gurkha Rifles, Dhankuta, ,Grave Ref. VII. F. 1. Rifleman BHAWAN SING THAPA , 4th Prince of Wales' Own Gurkha Rifles. Gahrung, , Grave Ref. VII. C. 4. Rifleman BHIM BAHADUR CHHETRI , 6th Gurkha Rifles. Gorkha, Grave Ref. VII. C. 5. Rifleman BHUPAL THAPA , 2nd King Edward VII's Own Gurkha Rifles (The Sirmoor Rifles). Sallyan, Grave Ref. VII. E. 4. Rifleman BIR BAHADUR SUNWAR , 7th Gurkha Rifles. Ramechhap, Grave Ref. VII. F. 8. Rifleman BIR BAHADUR THAPA, 8th Gurkha Rifles, Palpa, Grave Ref. -

Emergency Response Report Kohat February 2010
Responding to Emergencies Reducing the cries Table of Contents 1. Introduction……………………………………………………………………………. 03 2. Emergency Situation updates…………………………………………………. 03 3. IDPs Registration…………………………………………………………………….. 03 4. Relief Assistance…………………………………………………………………….. 04 5. Women in the Area………………………………………………………………… 04 6. Gaps Indentified……………………………………………………………………. 04 7. GPP Intervention…………………………………………………………………… 05 8. Summary of NFI Kits distribution……………………………………………. 05 9. IDPs Testimonials…………………………………………………………………… 06 10.Snap Shot of GPP NFI Kit distribution…………………………………….. 07 Global Peace Pioneers (GPP) 2 Responding to Emergencies Reducing the cries Global Peace Pioneer - Response for Conflict-Affected Children and Families in Pakistan “Emergency Relief Distribution” in Kohat February 2010. At age 6 Murad Khan, resident of Terah now displaced in Kohat district receives Hygiene Kit on behalf of his mother, Global Peace Pioneers distributed Hygiene Kits & Blankets among the IDPs settled in Jumrah UC in Kohat Global Peace Pioneers (GPP) distributed Hygiene Kits and Blankets among IDPs from Orkzai Agency and Valley Terah on Feb 24, 2010 in coordination with District Government Kohat. GPP aims to assist IDPs in the WASH sector through the provision of better sanitation facilities for the women and children of IDPs living in Host Communities, distribution of NFIs kit (Hygiene Kit & Clothes Washing Kit) and building on the capacities through awareness raising sessions / campaign among women and children on best health & hygiene practices. Emergency Situation Updates: Kohat is of the district in NWFP with district administration history from 1847.It has an area of 2545 Sq. Kilometers with population of around 7, 80,000 where male female ration is 52:48. Kohat is considered as one of the Model Districts in NWFP. Kohat district shares its boundaries with Kurram Agency, there are Afghan Refugees inhabited areas and camps present in the district for 30 years now. -

Evaluation of Tree Foliage As a Feed for Ruminant Livestock in NWFP, Pakistan
Sarhad J. Agric. Vol.29, No.1, 2013 MINERAL COMPOSITION OF LOCAL TREE LEAVES FOR FEEDING SHEEP AND GOATS IN KOHAT DISTRICT OF KHYBER PAKHTUNKHWA GHULAM HABIB, MOHAMMAD SALEEM and ABDUL HAMEED Faculty of Animal Husbandry & Veterinary Sciences, The University of Agriculture, Peshawar – Pakistan. E-mail: [email protected] ABSTRACT Mineral profile of tree leaves from eight local species (Acacia modesta, Albezia lebbeck, Capparis aphyla, Prosopes Juliflora, Tecoma undulata, Olea cuspidate, Ziziphus mauritiana and Ziziphus jujuba) was evaluated for feeding to sheep and goats. Leave samples were collected from three different locations (Surgul, Shakardara and Gumbat) in Kohat district of Khyber Pakhtunkhwa, Pakistan province and analyzed for total mineral matter, Ca, P, Na, K, Cu, Zn, Fe and Mn and In vitro DM digestibility. Statistical variations due to tree species and location were inconsistent for macro and micro minerals. Except Na, the contents of Ca, P and K were significantly influenced by tree species. Calcium contents were in the optimum range (1.66 to 5.14%) in all the leaves except Capparis aphyla (0.22%). Conversely, P was in the lower range (0.05-0.14%) in all samples that resulted in wide Ca:P ratio. Na in all samples was found ten times less than the required levels. Potassium was two folds higher than the recommended dietary level. Among the four micro-minerals, only Zn and Mn responded to difference in tree species and none varied due to location. Copper contents averaged 3.32 ppm across the tree species as against the required dietary levels 4 to10 ppm. The contents of Zn.