Gi Tract Embryology 1 Development of the Oral Cavity
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Prospective Isolation of NKX2-1–Expressing Human Lung Progenitors Derived from Pluripotent Stem Cells
The Journal of Clinical Investigation RESEARCH ARTICLE Prospective isolation of NKX2-1–expressing human lung progenitors derived from pluripotent stem cells Finn Hawkins,1,2 Philipp Kramer,3 Anjali Jacob,1,2 Ian Driver,4 Dylan C. Thomas,1 Katherine B. McCauley,1,2 Nicholas Skvir,1 Ana M. Crane,3 Anita A. Kurmann,1,5 Anthony N. Hollenberg,5 Sinead Nguyen,1 Brandon G. Wong,6 Ahmad S. Khalil,6,7 Sarah X.L. Huang,3,8 Susan Guttentag,9 Jason R. Rock,4 John M. Shannon,10 Brian R. Davis,3 and Darrell N. Kotton1,2 2 1Center for Regenerative Medicine, and The Pulmonary Center and Department of Medicine, Boston University School of Medicine, Boston, Massachusetts, USA. 3Center for Stem Cell and Regenerative Medicine, Brown Foundation Institute of Molecular Medicine, University of Texas Health Science Center, Houston, Texas, USA. 4Department of Anatomy, UCSF, San Francisco, California, USA. 5Division of Endocrinology, Diabetes and Metabolism, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, Massachusetts, USA. 6Department of Biomedical Engineering and Biological Design Center, Boston University, Boston, Massachusetts, USA. 7Wyss Institute for Biologically Inspired Engineering, Harvard University, Boston, Massachusetts, USA. 8Columbia Center for Translational Immunology & Columbia Center for Human Development, Columbia University Medical Center, New York, New York, USA. 9Department of Pediatrics, Monroe Carell Jr. Children’s Hospital, Vanderbilt University, Nashville, Tennessee, USA. 10Division of Pulmonary Biology, Cincinnati Children’s Hospital, Cincinnati, Ohio, USA. It has been postulated that during human fetal development, all cells of the lung epithelium derive from embryonic, endodermal, NK2 homeobox 1–expressing (NKX2-1+) precursor cells. -

Regulation of Early Lung Morphogenesis: Questions, Facts and Controversies
REVIEW 1611 Development 133, 1611-1624 (2006) doi:10.1242/dev.02310 Regulation of early lung morphogenesis: questions, facts and controversies Wellington V. Cardoso* and Jining Lü During early respiratory system development, the foregut endodermal specification, lung primordium formation, and the endoderm gives rise to the tracheal and lung cell progenitors. regulation of the initial stages of branching morphogenesis and Through branching morphogenesis, and in coordination with differentiation in the embryonic lung. We address questions such as vascular development, a tree-like structure of epithelial ‘when and how is respiratory cell fate established?’, ‘how do lung tubules forms and differentiates to produce the airways and buds form?’, ‘how are stereotypical patterns of airway branching and alveoli. Recent studies have implicated the fibroblast growth cellular diversity generated in the developing lung?’ and ‘which factor, sonic hedgehog, bone morphogenetic protein, retinoic pathways and targets are key to these processes?’. Most of what is acid and Wnt signaling pathways, and various transcription described refers to mouse lung development because of the genetic factors in regulating the initial stages of lung development. data available (Table 1). Lung vascular development and later events, However, the precise roles of these molecules and how they such as sacculation and alveoli formation, are not discussed in this interact in the developing lung is subject to debate. Here, we review (for reviews, see Pauling and Vu, 2004; Williams, -
Branching Morphogenesis of the Lung: New Molecular Insights Into an Old Problem
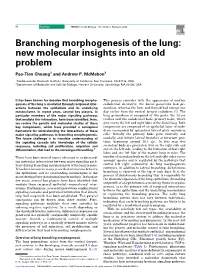
86 Review TRENDS in Cell Biology Vol.13 No.2 February 2003 Branching morphogenesis of the lung: new molecular insights into an old problem Pao-Tien Chuang1 and Andrew P. McMahon2 1Cardiovascular Research Institute, University of California, San Francisco, CA 94143, USA 2Department of Molecular and Cellular Biology, Harvard University, Cambridge, MA 02138, USA It has been known for decades that branching morpho- This process coincides with the appearance of another genesis of the lung is mediated through reciprocal inter- endodermal derivative, the dorsal pancreatic bud pri- actions between the epithelium and its underlying mordium, whereas the liver and thyroid bud emerge one mesenchyme. In recent years, several key players, in day earlier from the ventral foregut endoderm [5]. The particular members of the major signaling pathways lung primordium is composed of two parts: the future that mediate this interaction, have been identified. Here, trachea and two endodermal buds (primary buds), which we review the genetic and molecular studies of these give rise to the left and right lobes of the distal lung. Both key components, which have provided a conceptual components are composed of an epithelial layer of endo- framework for understanding the interactions of these derm surrounded by splanchnic lateral plate mesoderm major signaling pathways in branching morphogenesis. cells. Initially the primary buds grow ventrally and The future challenge is to translate understanding of caudally, and initiate lateral branches at invariant posi- the signaling cascade into knowledge of the cellular tions, beginning around 10.5 dpc. In this way, five responses, including cell proliferation, migration and secondary buds are generated, four on the right side and differentiation, that lead to the stereotyped branching.* one on the left side, leading to the formation of four right lobes and one left lobe of the mature lung in mice. -

Embryology Dr. Azal N.Al-Nusear Respiratory System 1-Upper
Embryology Dr. Azal N.Al-Nusear Respiratory System 1-Upper Respiratory System: The upper respiratory system consists of the nose, nasopharynx, and oropharynx. 2-Lower Respiratory system: The lower respiratory system consists of the larynx, trachea, bronchi, and lungs. The first sign of development is the formation of the respiratory diverticulum in the ventral wall of the primitive foregut during week 4. The distal end of the respiratory diverticulum enlarges to form the lung bud. The lung bud divides into two bronchial buds that branch into the primary, secondary, tertiary, and subsegmental bronchi. The respiratory diverticulum initially is in open communication with the foregut, but eventually they become separated by mesoderm (tracheoesophageal folds). When the tracheoesophageal folds fuse in the midline to form the tracheoesophageal septum, the foregut is divided into the trachea ventrally and esophagus dorsally. RD: respiratory diverticulum F: foregut. VM: visceral mesoderm. TEF : tracheoesophageal folds the trachea (T) and esophagus (E). B = bronchial buds. LL = left lung; L = right lung; Development of Individual Parts of the Respiratory System Larynx The larynx develops from the cranial part of laryngotracheal diverticulum. The opening of the respiratory diverticulum into the foregut becomes the laryngeal orifice. The mesenchyme (of fourth and sixth pharyngeal arches) surrounding the laryngeal orifice proliferates. As a result, the slit-like laryngeal orifice becomes T shaped. Subsequently laryngeal orifice acquires a characteristic adult shape. The lining epithelium of larynx develops from endoderm of this diverticulum. At first the endodermal cells proliferate and completely obliterate lumen of larynx. Later the cells breakdown and recanalization of larynx take place. -

Dnmt1 Is Required for Proximal-Distal Patterning of the Lung Endoderm and for Restraining Alveolar Type 2 Cell Fate
Developmental Biology 454 (2019) 108–117 Contents lists available at ScienceDirect Developmental Biology journal homepage: www.elsevier.com/locate/developmentalbiology Original research article Dnmt1 is required for proximal-distal patterning of the lung endoderm and for restraining alveolar type 2 cell fate Derek C. Liberti a,b,c,1, Jarod A. Zepp b,c,1, Christina A. Bartoni b,c, Kyle H. Liberti d, Su Zhou c, Minmin Lu c, Michael P. Morley b,c, Edward E. Morrisey a,b,c,e,f,* a Department of Cell and Developmental Biology, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, 19104, USA b Penn Cardiovascular Institute, University of Pennsylvania, Philadelphia, PA, 19104, USA c Penn Center for Pulmonary Biology, University of Pennsylvania, Philadelphia, PA, 19104, USA d Middleware Engineering, Red Hat, Westford, MA, 01886, USA e Department of Medicine, University of Pennsylvania, Philadelphia, PA, 19104, USA f Penn-CHOP Lung Biology Institute, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, 19104, USA ABSTRACT Lung endoderm development occurs through a series of finely coordinated transcriptional processes that are regulated by epigenetic mechanisms. However, the role of DNA methylation in regulating lung endoderm development remains poorly understood. We demonstrate that DNA methyltransferase 1 (Dnmt1) is required for early branching morphogenesis of the lungs and for restraining epithelial fate specification. Loss of Dnmt1 leads to an early branching defect, a loss of epithelial polarity and proximal endodermal cell differentiation, and an expansion of the distal endoderm compartment. Dnmt1 deficiency also disrupts epithelial-mesenchymal crosstalk and leads to precocious distal endodermal cell differentiation with premature expression of alveolar type 2 cell restricted genes. -
Development of Respiratory System
Development of respiratory system Respiratory block-Anatomy-Lecture 5 Editing file Color guide : Only in boys slides in Green Only in girls slides in Purple Objectives important in Red Doctor note in Blue Extra information in Grey ➔ Identify the development of the laryngotracheal (respiratory) diverticulum. ➔ Identify the development of the larynx. ➔ Identify the development of the trachea. ➔ Identify the development of the bronchi & Lungs. ➔ Describe the periods of the maturation of the lung. ➔ Identify the most congenital anomaly 3 Respiratory system Upper respiratory Lower respiratory tract tract Nasal cavity & Nose paranasal Laryngopharynx Larynx Trachea Bronchi Lungs sinuses Development of the respiratory tract 4 The endoderm & Begins during the 4th week of Development of longitudinal Proximal & distal parts of the surrounding splanchnic development tracheoesophageal septum respiratory diverticulum mesoderm ▹ Divides the diverticulum ▹ Begins as a median ▹ The proximal part of the ▹ The endoderm lining the into: outgrowth (laryngotracheal respiratory diverticulum laryngotracheal ▸ Dorsal portion*: groove) from the caudal part remains tubular and forms diverticulum (respiratory primordium (in the of the ventral wall of the larynx & trachea. diverticulum) gives rise to earliest stage of primitive pharynx (foregut). ▹ The distal end of the the: development) of the ▹ The groove invaginates (fold diverticulum dilates to form ▸ Epithelium & glands oropharynx & within itself) and forms lung bud, which divides to of the respiratory esophagus. laryngotracheal give rise to 2 lung buds tract. ▸ Ventral portion*: (respiratory) diverticulum. (primary bronchial buds). ▹ The surrounding splanchnic primordium (=give mesoderm gives rise to the: rise) of larynx, ▸ Connective tissue, trachea, bronchi & cartilage & smooth lungs. muscles of the respiratory tract. * Remember that the larynx, trachea, bronchi & lungs lie anteriorly while the oropharynx & esophagus lie posteriorly. -

1Physiologic Principles of the Respiratory System
Acute Respiratory Care of the Neonate Physiologic Principles 1of the Respiratory System Bill Diehl-Jones, RN, PhD central issue in caring for ill or premature infants EMBRYONIC LUNG DEVelOPMENT A is the successful management of respiratory sta Late in the embryonic period (four weeks postcon tus. Management can be complicated by the relative ception), the rudiments of the respiratory system are lack of development of these infants’ respiratory struc established. The lower respiratory structures, which tures and the functional immaturity of their respiratory include the larynx, trachea, bronchi, and lungs, begin systems. This chapter therefore begins with a review of to form in this period.2 The anatomic precursor of the the developmental and functional anatomy of the lungs future respiratory system is the laryngotracheal groove, and associated structures. Subsequent sections address an outgrowth of the primordial pharynx, which is visi lung mechanics, the synthesis and roles of pulmonary ble by approximately day 24 of embryonic development surfactant, and the physiology of lung fluid and of fetal (Figure 11). This groove extends downward and is grad breathing. The events of transition and other elements ually separated from the future esophagus by a septum. of neonatal respiratory physiology are also discussed. Failure of the septum to develop completely results in Particular attention is given to those issues that are a tracheoesophageal fistula. Several other congenital unique to the neonate, with the hope that this infor anomalies of the respiratory system can develop during mation will assist the clinician in understanding and the embryonic and/or early fetal periods; they are sum optimally facilitating respiration in the newborn infant. -

Lung Development
12. LUNG DEVELOPMENT Peter Rothstein, MD [email protected] RECOMMENDED READING: Larsen, Human Embryology, 3rd edition, pp 143-155. Additional sources: 1. DiFiore JW, Wilson JM. Lung development. Seminars in Pediatric Surgery 3:221-32, 1994. 2. Harding R, Hooper SB. Regulation of lung expansion and lung growth before birth. J. Appl. Physiol. 81:209-24, 1996. 3. Gregory GA, Kitterman JA, Phibbs RH, Tooley WH, Hamilton WK. Treatment of the idiopathic respiratory distress syndrome with continuous positive airway pressure. N. Eng. J. Med. 284:1333-40, 1971. This paper describes how a simple clinical observation led to a tremendous breakthrough in the treatment of neonatal respiratory distress syndrome. 4. Whitsett JA, Weaver TE. Hydrophobic surfactant proteins in lung function and disease. N. Eng. J Med 347:2141-48, 2002. LEARNING OBJECTIVES: You should be able to: 1. Discuss the growth and functional development of the respiratory system. 2. Discuss the stages of lung development and the major events of each stage. 3. Describe the physical and biochemical requirements for alveolar development and function. 4. Identify the developmental causes of neonatal respiratory failure, tracheoesophageal fistula and diaphragmatic hernia. GLOSSARY: Surfactant – Macromolecular complex of phospholipids and hydrophobic proteins present in alveoli that decreases surface tension and prevents alveolar collapse during exhalation. Largest lipid components are phosphatidylcholine (lecithin) and phosphatidylglycerol Type I cell (pneumocyte) – found in the airways -

Jeanine D'armiento, M.D., Ph.D. Function of Breathing Conducting
Function of Breathing Jeanine D’Armiento, M.D., Ph.D. Ventilation-air conduction Moving gas in and out of the chest Associate Professor Gas Exchange Moving gas Oxygen and carbon Department of Medicine dioxide in and out of the blood oxygen from air to blood P&S 9-449 carbon dioxide from blood to air 5-3745 Air Sacs [email protected] (alveoli) Main stem bronchus Critical to the Development of the Lung Lobar bronchus (5 lung lobes) • Need a branched respiratory tree with a Segmental bronchus (10 mucociliary cleaning mechanism bronchopulmonary segments • A complex gas-exchange region with on right, 9 on left efficient diffusion and short diffusion Branching continues as distance airways become bronchioles, then at terminal bronchioles • Network of capillaries in close contact with airways transition into the airspaces respiratory bronchioles • A surface film to reduce the surface About 20 branch generations tension of the alveoli and prevent collapse from beginning to end Conducting Portion Respiratory Portion • Naval Cavity-hairs for filter, olfactory mucosa for smell • Pharynx-cavity for speech and part of alimentary tract • Respiratory bronchioles-lead to alveolar component • Larynx-vocal cords • Alveolar Ducts-proportion of interspersed alveoli • Trachea-Flexible connection between lungs and more increases such that they occupy the majority of the rigid structures of upper respiratory tract airway surface • Bronchi-Trachea divides into 2 primary bronchi which • Alveolar Sacs-end of alveolar ducts (cluster of lead to left and right lung alveoli) • Bronchioles-final Conducting portions. Devoid of cartilage, undergo more branching and final segments • Alveolus-Unit of gas exchange are called terminal bronchioles. -

The Respiratory System
Embryology18 Dr.Ban The respiratory system Respiratory system development is a highly coordinated and complex process it’s development is tightly associated with the digestive system from the beginning.The respiratory tract is divided anatomically into 2 main parts: A-upper respiratory tract, consisting of the nose, nasal cavity and the pharynx B-lower respiratory tract consisting of the larynx, trachea, bronchi and the lungs. The pharynx is the part of the throat behind the mouth and nasal cavity, and above the esophagus and larynx. In humans, the pharynx is part of the digestive system and the conducting zone of the respiratory system. The conducting zone which also includes the nostrils of the nose, the larynx, trachea, bronchi, and bronchioles filters, warms and moistens air and conducts it into the lungs). The human pharynx is divided into three sections: . nasopharynx . oropharynx . laryngopharynx 1 Embryology18 Dr.Ban The larynx The internal lining of the larynx originates from endoderm, but the cartilages and muscles originate from mesenchyme of the 4th and 6th pharyngeal arches. As a result of rapid proliferation of this mesenchyme, the laryngeal orifice changes in appearance from a sagital slit to a T-shaped opening. When the mesenchyme of the two arches transforms into the thyroid, cricoid and arytenoid cartilages the adult shape of the laryngeal orifice can be recognized. The laryngeal epithelium proliferates rapidly, resulting in a temporary occlusion of the lumen. Subsequently, vacuolization and recanalization produces a pair of lateral recesses, the laryngeal ventricles that are bounded by folds of tissue that differentiate into the false and true vocal cords. -

Posterior Lung Herniation in Pulmonary Agenesis and Aplasia
Brief Research Report | Pediatric Imaging eISSN 2005-8330 https://doi.org/10.3348/kjr.2021.0155 Korean J Radiol 2021;22(10):1690-1696 Posterior Lung Herniation in Pulmonary Agenesis and Aplasia: Chest Radiograph and Cross-Sectional Imaging Correlation Ji Young Kim1, 2, Woo Sun Kim1, 3, 4, Kyung Soo Lee5, Bo-Kyung Je6, Ji Eun Park7, Young Jin Ryu1, 2, Young Hun Choi1, 3, Jung-Eun Cheon1, 3, 4 1Department of Radiology, Seoul National University College of Medicine, Seoul, Korea; 2Department of Radiology, Seoul National University Bundang Hospital, Seongnam, Korea; 3Department of Radiology, Seoul National University Hospital, Seoul, Korea; 4Institute of Radiation Medicine, Seoul National University Medical Research Center, Seoul, Korea; 5Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine (SKKU-SOM), Seoul, Korea; 6Department of Radiology, Korea University College of Medicine, Ansan Hospital, Ansan, Korea; 7Department of Radiology, Ajou University Medical Center, Suwon, Korea Objective: To describe the anatomic locations and imaging features of posterior lung herniation in unilateral pulmonary agenesis and aplasia, focusing on radiograph-CT/MRI correlation. Materials and Methods: A total of 10 patients (seven with pulmonary agenesis and three with pulmonary aplasia, male: female = 1:9, mean age 7.3 years, age range from 1 month to 20 years) were included. Chest radiographs (n = 9), CT (n = 9), and MRI (n = 1) were reviewed to assess the type of lung underdevelopment, presence of anterior and posterior lung herniation, bronchus origin, supplying artery, and draining vein of the herniated lung. Results: Pulmonary agenesis/aplasia more commonly affected the left lung (n = 7) than the right lung (n = 3). -

Embryology of the Respiratory System Respiratory Block - Lecture 1
Embryology of the respiratory system Respiratory Block - Lecture 1 Color index: Important In male’s slides only In female’s slides only Extra information, explanation Doctors notes Editing File Objectives: ● Identify the development of the laryngotracheal (respiratory) diverticulum ● Identify the development of the larynx ● Identify the development of the trachea ● Identify the development of the bronchi & lungs ● Describe the periods of the maturation of the lung ● Identify the most congenital anatomy Respiratory system Upper respiratory tract: ● Nose ● Nasal cavity & paranasal sinuses ● Laryngo-pharynx ● Larynx Lower respiratory tract: ● Trachea ● Bronchi ● Lungs In embryology, the lower respiratory tract includes the larynx Development of the respiratory tract ● Begins during the 4th week of development. ● Begins as a median outgrowth ( laryngo-tracheal groove) from the caudal part of the ventral wall of the primitive pharynx (foregut) ● The groove envaginates and forms laryngotracheal (respiratory) diverticulum. A longitudinal tracheo- esophageal septum develops and divides the diverticulum into a: ● Dorsal portion: Primordium of the oropharynx and esophagus (digestive) ● Ventral portion: Primordium of larynx,trachea,bronchi and lungs (respiratory) ● The proximal part of the respiratory diverticulum remains tubular and forms larynx & trachea. ● The distal end of the diverticulum dilates to form lung bud, which divides to give rise to 2 lung buds ( primary bronchial buds) The endoderm lining the laryngotracheal diverticulum ( respiratory diverticulum) gives rise to the : ● Epithelium & glands of the respiratory tract The surrounding splanchnic mesoderm gives rise to the: ● Connective tissue,cartilage & smooth muscles of the respiratory tract Development of the larynx ● The opening of the laryngotracheal diverticulum into the primitive foregut becomes the laryngeal orifice.