Big Buddy Project Brief
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
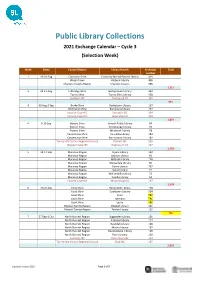
Public Library Collections 2021 Exchange Calendar – Cycle 3 (Selection Week)
Public Library Collections 2021 Exchange Calendar – Cycle 3 (Selection Week) Week Dates Council/Region Library Branch Exchange Total number 1 16-20 Aug Cloncurry Shire Cloncurry Bob McDonald Library 419 Weipa Town Hibberd Library 496 Charters Towers Region Charters Towers 596 1,511 2 23-27 Aug Etheridge Shire Georgetown Library 232 Torres Shire Torres Shire Library 458 Southern IKC Cherbourg IKC 267 957 3 30 Aug-3 Sep Burke Shire Burketown Library 167 Richmond Shire Richmond Library 237 Eastern Cape IKC Yarrabah IKC 334 Eastern Cape IKC Hope Vale IKC 334 1,072 4 6-10 Sep Barcoo Shire Jundah Public Library 94 Barcoo Shire Stonehenge Library 79 Barcoo Shire Windorah Library 78 Carpentaria Shire Karumba Library 184 Carpentaria Shire Normanton Library 182 Torres Strait Island Regional Council Poruma IKC 226 Western Cape IKC Napranum IKC 267 1,110 5 13-17 Sep Maranoa Region Injune Library 102 Maranoa Region Jackson Library 91 Maranoa Region Mitchell Library 128 Maranoa Region Mungallala Library 85 Maranoa Region Roma Library 707 Maranoa Region Surat Library 71 Maranoa Region Wallumbilla Library 73 Maranoa Region Yuleba Library 54 Eastern Cape IKC Wujal Wujal IKC 267 1,578 6 20-24 Sep Cook Shire Bloomfield Library 128 Cook Shire Cooktown Library 504 Cook Shire Coen TBC Cook Shire Lakeland TBC Cook Shire Laura TBC Blackall-Tambo Region Blackall Library 261 Blackall-Tambo Region Tambo Library 102 TBC 7 27 Sep-1 Oct North Burnett Region Biggenden Library 101 North Burnett Region Eidsvold Library 117 North Burnett Region Gayndah Library 168 North -

Local Government
QueenslandQueensland Government Government Gazette Gazette PP 451207100087 PUBLISHED BY AUTHORITY ISSN 0155-9370 Vol. 355] Friday 5 November 2010 VACANCIES GAZETTE NOTICE Please note that Friday, 5th November 2010 is the last edition of the Vacancies Gazette There is no longer a requirement for Agencies to publish the vacancy positions in the Vacancies Gazette as per the Public Service Commission Recruitment and Selection Directive 1/10 as issued in January 2010. However, the requirement to publish the appointment of advertised vacancy positions in the Gazette remains in place. Therefore, all appointment notice submissions received from Monday, 8th November 2010 will be published in the Queensland Government General Gazette . All existing subscriptions to the Vacancies Gazette will be transferred to the General Gazette, i.e. from the week ending Friday, 12th November 2010 all Vacancies Gazette subscribers will receive the General Gazette for the duration of their subscription. If you would prefer to cancel your subscription to the Vacancies Gazette , please contact SDS by emailing [email protected] [599] Queensland Government Gazette Extraordinary PP 451207100087 PUBLISHED BY AUTHORITY ISSN 0155-9370 Vol. 355] Friday 29 October 2010 [No. 63 Transport Infrastructure Act 1994 NOTIFICATION OF REVOCATION OF DECLARATION OF STATE CONTROLLED ROAD AND MOTORWAY Exercising the power under section 24AA of the Acts Interpretation Act 1954 notice is hereby given under section 24 and 27 of the Transport Infrastructure Act 1994 of the revocation of: (a) the declaration as a state controlled road; and (b) the declaration of state controlled road as a motorway, of the road or route or part of the road or route described in the Schedule. -
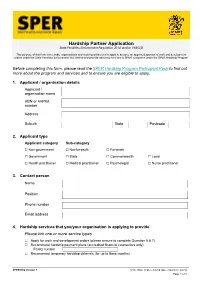
SPER Hardship Partner Application Form
Hardship Partner Application State Penalties Enforcement Regulation 2014 section 19AG(2) This purpose of this form is to enable organisations and health practitioners to apply to become an approved sponsor of work and development orders under the State Penalties Enforcement Act 1999 and/or provide advocacy services to SPER customers under the SPER Hardship Program Before completing this form, please read the SPER Hardship Program Participant Pack to find out more about the program and services and to ensure you are eligible to apply. 1. Applicant / organisation details Applicant / organisation name ABN or AHPRA number Address Suburb State Postcode 2. Applicant type Applicant category Sub-category ☐ Non-government ☐ Not-for-profit ☐ For-profit ☐ Government ☐ State ☐ Commonwealth ☐ Local ☐ Health practitioner ☐ Medical practitioner ☐ Psychologist ☐ Nurse practitioner 3. Contact person Name Position Phone number Email address 4. Hardship services that you/your organisation is applying to provide Please tick one or more service types ☐ Apply for work and development orders (please ensure to complete Question 6 & 7) ☐ Recommend hardship payment plans (accredited financial counsellors only) FCAQ number ☐ Recommend temporary hardship deferrals (for up to three months) SPER6002 Version 1 ©The State of Queensland (Queensland Treasury) Page 1 of 8 5. Locations where you/your organisation will provide these services ☐ All of Queensland or Select Local Government Area(s) below: ☐ Aurukun Shire ☐ Fraser Coast Region ☐ North Burnett Region ☐ Balonne -

Coalition Government Funding Means Goondiwindi Region Pre-Schoolers Will Be Given the Chance to Learn a Second Language
David Littleproud MP Federal Member for Maranoa Media statement March 21, 2017 Coalition Government funding means Goondiwindi region pre-schoolers will be given the chance to learn a second language SPEAKING a second language isn’t just about making travel easier, the ability can also boost creativity and now – thanks for Federal Government funding – 47 pre-schoolers in the Goondiwindi region will be given the opportunity to learn Mandarin and French, Maranoa MP David Littleproud said. “The Coalition Government’s Early Learning Languages Australia (ELLA) program means Chinese/ Mandarin will be offered at LEAD Childcare Goondiwindi and kids will be able to learn French at the Toobeah Kindergarten,” Mr Littleproud said. “This opportunity will not only start a life-long interest in language learning for our kids but also boost their English and problem-solving skills. “Exposure to another language and culture can have significant benefits on children from a young age – it expands their horizons and opens up exciting opportunities around the world when they reach the workforce.” Mr Littleproud said 566 preschool children across his rural electorate were going to be given the opportunity to learn a second language. “This funding provides a great opportunity for our country kids with French being offered at Toobeah to Spanish on offer in Longreach – just because you live in a small town shouldn’t limit your education access,” he said. ELLA began as a small trial of 41 preschools in 2015 and is a digital, play-based program where preschool children use a series of interactive applications (apps). It is designed for use by educators who do not have formal language training and extensive support, training and resources are provided to assist educators in the effective delivery of early language learning and cultural awareness. -

Corporate Plan 2019-2024 Has Been Prepared with the Assistance of SC Lennon & Associates
Goondiwindi Regional Council Corporate Plan 2019 – 2024 Setting the direction to serve our community THRIVING RICH AGRICULTURAL COUNTRY HISTORY EXCELLENCE CULTURE GOONDIWINDI REGIONAL COUNCIL p: (07) 4671 7400 e: [email protected] w: www.grc.qld.gov.au Message from the Mayor & Chief Executive Officer We are pleased to present the Goondiwindi Regional Council Corporate Plan 2019 – 2024. The corporate plan sets Council’s vision for the region and provides a strategic framework for enhancing the quality lifestyle our communities currently enjoy. Over the life of this plan, Council will work toward its vision to ensure the region’s thriving regional lifestyle and prosperous economy. Council will continue to maintain a strong working relationship with State and Federal Governments to ensure the region’s infrastructure needs into the future are met. It is most important that a growing region such as ours is supported by adequate infrastructure. Councillors and officers of Goondiwindi Regional Council will continue to work with the community by providing service delivery that is timely, decisive and accommodating. This ideology will assist businesses and residents to undertake day-to-day activities with the support of Council. We are confident the continued commitment by Council and the community working together will benefit current and future residents. Council understands the significant challenges, which lay ahead, and the need to carefully manage the growth of the region by balancing the competing demands of financial, social and environmental pressures. The deliverables in this plan will help manage these challenges. We are confident Council and staff working in partnership with our communities to deliver the priority strategies of this corporate plan will not only strengthen Council but ultimately make our region an even a better place to live. -

Goondiwindi Steven Crimp and Mark Howden, Australian National University
Changes in northern farming system climate conditions - Goondiwindi Steven Crimp and Mark Howden, Australian National University Key words climate projections, production impacts, adaptation options Take home messages • Greenhouse gas (GHG) emissions continue to accumulate in the earth’s atmosphere and drive warmer global temperatures. Warming of globally averaged air temperatures of just over 1oC since records began in 1850 has produced national, regional and local changes in environmental conditions. These changes have shifted debate from “Is climate change real?” to “What should we do about it?” • Adapting agricultural practises will be required to respond to changing environmental conditions and will require all components of the agricultural value chain to work together in order to maintain resilient and profitable food systems Historical changes in climate? Preliminary results suggest that 2019 is likely to be either the second or third warmest year on record, with globally annual averaged air temperatures now 1oC warmer than the long-term average calculated for the period 1961 to 1990. This warming is driven by increasing concentrations of all the major long-lived greenhouse gases in the atmosphere, with carbon dioxide (CO2) concentrations rising from 208ppm prior to the industrial revolution, to 413.65 ppm as of 4 January 2020 (NOAA, 2020). In Australia, warming in average temperature (average temperature) has resulted in 2019 being the warmest year on record (1.52oC above the 1961 to 1990 average of 21.8oC) (BoM, 2020). Average daytime maximum temperatures in 2019 of 30.69oC were 2.09oC above the 1961 to 1990 average. In December 2019 more than 40% of the entire country recorded maximum temperatures greater than the 97th percentile i.e. -

Proceedings of the 1St Queensland Pest Animal and Weed Symposium
PAWS 2019 PEST ANIMAL & WEED SYMPOSIUM 2019 20-23 MAY 2019, SEA WORLD RESORT CONFERENCE CENTRE, GOLD COAST, AUSTRALIA Get on board Proceedings of the 1st Queensland Pest Animal and Weed Symposium www.wsq.org.auwww.QWS2017.com #QWS2017 | 1 PEST ANIMAL & WEED SYMPOSIUM 2019 WELCOME MESSAGE It is my pleasure to welcome you all to the inaugural 2019 Pest Animal and Weed Symposium on the Gold Coast. Thanks to the backing of the Weed Society of Queensland and the strong support from delegates and presenters, we are pleased to deliver a symposium that is relevant to the entire industry. I would also like to thank our sponsors, exhibitors, event managers and committee volunteers for their contributions towards the success of this year’s symposium. I’m sure you will agree we have a great program, with an inspiring opening address, three exceptional keynote speakers, 50 oral presentations, five speed presentations, eight video submissions and 20 posters on display, we hope to encourage delegates to challenge themselves in managing pest animals and weeds. Please take the time to share your knowledge and I look forward to meeting all of you at this year’s symposium. Chairperson 2019 Queensland Pest Animal and Weed Symposium BROUGHT TO YOU BY www.wsq.org.au @weedsocietyqld #paws2019 SYMPOSIUM PROGRAM DAY ONE: MONDAY, 20 MAY 2019 4:30pm - 7:00pm Registration Desk Open Sea World Resort Conference Centre 5:00pm - 7:00pm Welcome Reception Location: Exhibition Area, Sea World Resort Conference Centre Dress: Smart Casual 6:00pm Welcome Address Cr Hermann -
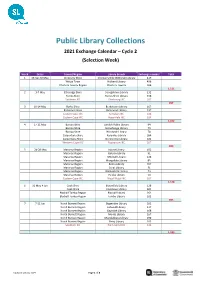
Public Library Collections 2021 Exchange Calendar – Cycle 2 (Selection Week)
Public Library Collections 2021 Exchange Calendar – Cycle 2 (Selection Week) Week Dates Council/Region Library Branch Exchange number Total 1 26 Apr-30 May Cloncurry Shire Cloncurry Bob McDonald Library 419 Weipa Town Hibberd Library 496 Charters Towers Region Charters Towers 596 1,511 2 3-7 May Etheridge Shire Georgetown Library 232 Torres Shire Torres Shire Library 458 Southern IKC Cherbourg IKC 267 957 3 10-14 May Burke Shire Burketown Library 167 Richmond Shire Richmond Library 237 Eastern Cape IKC Yarrabah IKC 334 Eastern Cape IKC Hope Vale IKC 334 1,072 4 17-21 May Barcoo Shire Jundah Public Library 94 Barcoo Shire Stonehenge Library 79 Barcoo Shire Windorah Library 78 Carpentaria Shire Karumba Library 184 Carpentaria Shire Normanton Library 182 Western Cape IKC Napranum IKC 267 884 5 24-28 May Maranoa Region Injune Library 102 Maranoa Region Jackson Library 91 Maranoa Region Mitchell Library 128 Maranoa Region Mungallala Library 85 Maranoa Region Roma Library 707 Maranoa Region Surat Library 71 Maranoa Region Wallumbilla Library 73 Maranoa Region Yuleba Library 54 Eastern Cape IKC Wujal Wujal IKC 267 1,578 6 31 May-4 Jun Cook Shire Bloomfield Library 128 Cook Shire Cooktown Library 504 Blackall-Tambo Region Blackall Library 261 Blackall-Tambo Region Tambo Library 102 995 7 7-11 Jun North Burnett Region Biggenden Library 101 North Burnett Region Eidsvold Library 117 North Burnett Region Gayndah Library 168 North Burnett Region Monto Library 167 North Burnett Region Mundubbera Library 196 North Burnett Region Perry Library 102 Southern -
Talk-About Newsletter
Talk-About The official newsletter for the Aboriginal and Torres Strait Islander Health Leadership Team April/May 2020 Metro North Hospital and Health Service Artist Elaine Chambers-Hegarty designed the ‘Better Together’ artwork for the van. Better Together Health Van unveiled to help close the gap on health outcomes A new Better Together Health Van unveiled on National Close the Gap Day (19 March 2020) is set to provide more convenient access to health care information for members of the Aboriginal and Torres Strait Islander community in Brisbane’s north. Metro North Aboriginal and Torres “Between 2011 and 2016, the “The introduction of the Better Strait Islander Leadership Team Aboriginal and Torres Strait Islander Together Health Van will allow Metro Director Sherry Holzapfel said the population residing in the Metro North North to deliver health promotion initiative would assist with education region increased by 37.6 per cent, and education, clinical service and service delivery in line with the compared to 18 per cent nationally. delivery and engagement activities for growing Indigenous population in By 2031, the Indigenous population Aboriginal and Torres Strait Islander Brisbane’s northern suburbs. in South East Queensland is projected people to improve health outcomes to be 133,189, the largest of any other and contribute to closing the gap on State’s population projection,” Ms life expectancy.” Holzapfel said. Give us Contact information feedback Royal Brisbane and Women’s Hospital We welcome your feedback, Indigenous Hospital Liaison Officer Ph: 07 3646 7489 contributions, story ideas and details on any upcoming events. Please contact Indigenous Hospital Liaison Officer Ph: 07 3646 1696 Aboriginal and Torres Strait Islander Health Unit Communications Manager Indigenous Hospital Liaison Officer Ph: 07 3646 7489 Renee Simon at Renee.Simon@health. -
Caravan & Camping
Goondiwindi Region Yelarbon � Inglewood Inglewood Caravan & Camping � Toobeah Toobeah � www.grc.qld.gov.au Goondiwindi Goondiwindi � Texas Texas Swimming Fishing Hour Limit 24 48 Hour Limit 72 Hour Limit Limit 14 Day Tables Barbeques Bins Laundry Dump Spot Onsite Good TV Reception Reception Telstra Cabins / Accommodation � www.facebook.com/grcqld Bungunya Bungunya Talwood Talwood Tent Area Tent Accessible Camper Trailer Accessible / Motorhome RV Only Road Caravans Off / Bus Accessible Big Rig Cost Free Donation Available Power Toilets Disabled Access Showers Drinking Water Dogs Allowed Amenities within the region No. Address How to get there/ Description Amenities Caravan Parks 2 Goondiwindi 36 Old Cunningham Hwy, Goondiwindi Goondiwindi Holiday Park welcomes business travellers, holidaymakers and tourists alike to our immaculate and spacious 13-acre site. Catering for a full Holiday Park Ph: 1300 725 915 range of accommodation options, from the basic tent sites, a variety of RV’s including large motorhomes, and fully self-contained accommodation. 4 Goondiwindi 20 Hungerford Street, Goondiwindi Enjoy 10 spacious parkland acres. Secure, clean & tidy. Hand feed our ducks & possums at our attractive billabong. Saturday pancake breakfast. Personalised Tourist Park Ph: 07 4671 2566 & friendly. Wireless internet. This park is a part of the Top Tourist Parks Network, an Australia-wide network of holiday parks and accommodation. 3 Goondiwindi Boundary Road, Goondiwindi Great stop to pull up, with so much space. Very clean/spotless amenities, new power boxes and sullage recently installed, private dump point onsite. Most Showgrounds Ph: 0437 809 415 sites are grassed and there is plenty of room for drive through and large rigs. -
Rural Registrar Incentive, Reimbursement and Support Policy
RURAL REGISTRAR INCENTIVE, REIMBURSEMENT AND SUPPORT POLICY Purpose This Policy describes the incentives, eligible reimbursements and supports offered by General Practice Training Queensland (GPTQ) to Registrars undertaking training in a rural General Practice setting. Scope This Policy applies to GP Registrars enrolled in Australian General Practice Training with General Practice Training Queensland who undertake training in a rural training practice commencing GPT/PRRT1 in 2021. Policy Background GPTQ provides specific financial support to its GP Registrars while undertaking a placement in a rural general practice setting within the GPTQ training region. The GPTQ Rural Registrar Incentive, Reimbursement and Support Policy considers the rurality of training places, the distance of the practice from a large referral centre and data collected from the Australian Government Health Workforce Locator. Eligible payment amounts under the GPTQ policy can be found in Appendix 2. GPTQ training practices are grouped geographically within the training footprint. Rural and Remote training affords registrars the opportunity to improve access for rural Australians to quality medical services as well as addressing workforce maldistribution concerns for rural and remote communities. GP Registrars who confirm rural practice employment will be eligible for the GPTQ Rural Registrar Incentive and Support Payments and may also be eligible for additional financial support through added GPTQ support and Australian Government initiatives such as the Workforce Incentive Program. The GPTQ Rural Incentive Policy has been designed to support registrars to relocate to the more rural and remote locations within the training region. GPTQ strongly encourages registrars undertaking rural placements to integrate into their community by residing and working in the area. -
Part 3 Strategic Framework 3.1 Preliminary
Part 3 Strategic framework 3.1 Preliminary (1) The strategic framework sets the policy direction for the planning scheme and forms the basis for ensuring appropriate development occurs within the planning scheme area for the life of the planning scheme. (2) Mapping for the strategic framework is included in Schedule 2 (Mapping). (3) For the purpose of describing the policy direction for the planning scheme, the strategic framework is structured in the following way: (a) the strategic intent; (b) the following seven (7) themes that collectively represent the policy intent of the scheme: (i) settlement pattern (ii) natural environment (iii) natural resources (iv) community identity and regional landscape character (v) economic development (vi) access, mobility and transport (vii) infrastructure and services (c) the strategic outcome(s) sought for development in the planning scheme area for each theme (d) the element(s) that refine and further describe the strategic outcome(s) (e) the specific outcomes sought for each, or a number of, elements (f) the land use strategies for achieving these outcomes. Editor’s note—Not all elements have land use strategies. (4) Although each theme has its own section, the strategic framework in its entirety represents the policy intent for the planning scheme. Part 3 Goondiwindi Region Planning Scheme (Version 2) Part 3–1 3.2 Strategic intent 3.2.1 Background and context 3.2.2 The history of Goondiwindi The Goondiwindi Region local government Region area (‘Goondiwindi Region’ or ‘the Region’) is The Goondiwindi Region contains a rich and located in the south-west Darling Downs. The varied cultural landscape that is of particular administrative centre of Goondiwindi Region, significance to the local Indigenous the town of Goondiwindi, is located communities who cared for their country and approximately 223 kilometres south-west of practiced sustainable natural resource Toowoomba and 348 kilometres south-west of management for many thousands of years.