Supplemental Application: Towing Workers’ Compensation to Be Completed with ACORD 130 Application
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Why Electric Vehicles?
Electric Vehicle Adoption A simple way to have a huge impact on our environment Why Electric Vehicles? Electric Vehicles (EV’s) are our best option to transition away from Internal Combustion Engine (ICE) vehicles and make a huge impact on our environment (28.9 percent of 2017 greenhouse gas emissions were from transportation in the U.S.) ● No tailpipe emissions from them ● Extremely inexpensive to operate and maintain ● So much fun to drive! Quick and quiet ● Easy to charge ● Range is increasing and price is decreasing BEV vs. PHEV vs. Hybrid ● BEV = Battery Electric Vehicle ○ Just batteries and an electric motor! ● PHEV = Plug-in Hybrid Electric Vehicle ○ Like a BEV and ICE car combined ○ Plugs in ○ Typical electric range of ~55kms ● Hybrid ○ Does not plug in ○ Electric motor only runs at low speeds How Far Do They Go? ● EV’s have range from 70kms to 500kms+ ● Range depends how you drive and the environment you are in ● Popular Canadian EV brands: Company Brand Range Price Price per KM Nissan Leaf 242 $42,000 $174 Nissan Leaf E+ 363 $44,300 $122 Hyundai Kona 415 $45,600 $110 Hyundai Ioniq 249 $37,900 $152 Kia Niro 385 $44,995 $117 Kia Soul 179 $35,900 $201 Tesla Model 3 SR + 386 $56,990 $148 Tesla Model 3 LR 499 $70,490 $141 VW E-Golf 201 $36,300 $181 Chevy Bolt 383 $43,200 $113 How Long to Charge? ● “Level 1” 110v standard outlet “trickle charging” = ~7kms per hour of charging ● “Level 2” 240v “dryer” outlet or hard-wired = 35-45kms per hour ● “Level 3” DC Fast charging = 100-1,600kms per hour What If You Run Out Of Charge?!?! ● You get a ton of warnings on your head-up display ● You can run out of gas too, didn’t you know? ● Electricity is EVERYWHERE, but gas stations aren’t! But really, ● you’d have to get towed on a flatbed tow truck ● 110v charging isn’t very convenient ● Tell your Municipality to add more level 2 chargers and your province to add more level 3 chargers! Where Can I Charge? #1 - At home! Primarly Lvl2 station in Saanich, etc. -

Vehicle Type Codes
VEHICLE TYPE CODES Specialized Vehicles Passenger Vehicles 41 - Ambulance 01 - Passenger Car, Station 42 - Dune Buggy Wagon, Jeep 43 - Fire Truck 02 - Motorcycle 44 - Fork Lift 03 - Motor Driven 45 - Hwy. Construction Equip. Cycle/Scooter 46 - Implement of Husbandry 04 - Bicycle 47 - Motor Home 05 - Motorized Bicycle 48 - Police Car 06 - All Terrain Vehicle 49 - Police Motorcycle 07 - Sport Utility Vehicle 50 - Mobile Equipment 08 - Mini-vans 51 - Farm Labor Vehicle (Certified) 55 - Two-Axle Tow Truck Buses 56 - Three-Axle Tow Truck 09 - Paratransit 57 - Farm Labor Vehicle 10 - Tour Bus (Non-Certified) 11 - Other Commercial 58 - Farm Labor Transporter 12 - Non-Commercial Bus 59 - Motor Home > 40 Feet 13 - School Bus Public Type I 14 - School Bus Public Type II Trailers 15 - School Bus Private Type I 28 - Semi Tank Trailer 16 - School Bus Private Type II 29 - Pull Tank Trailer 17 - School Bus Contractual Type I 30 - Two Tank Trailer 18 - School Bus Contractual Type II 31 - Semi 19 - General Public Paratransit 32 - Pull Vehicle 33 - Two Trailers (Includes Semi 20 - Public Transit Authority & Pull) 63 - Youth Bus 34 - Boat 64 - School Pupil Activity Bus Type I 35 - Utility 65 - School Pupil Activity Bus Type II 36 - Trailer Coach 37 - Extralegal Permit Load Trucks/Truck Tractors 38 - Pole, Pipe, or Logging Dolly 21 - Two Axle Tank Truck 39 - Three Trailers 22 - Pickups & Panels 40 - Federally Legal Semi 23 - Pickup w/Camper 52 - Federally Legal Double 24 - Three Axle Tank Truck Combo Over 75 Feet 25 - Truck Tractor 53 - Fifth Wheel Travel Trailer 26 - Two Axle Truck 54 - Container Chassis 27 - Three or More Axle Truck ANNEX C 3-C-1 HPM 110.5 Miscellaneous Hazardous Material 60 - Pedestrian 71 - Passenger Car, Station 61 - Second or Additional Wagon, Jeep Enforcement Action(s) 72 - Pickups and Panels 62 - Passengers 73 - Pickup and Camper 94 - Go-ped, ZIP Electric 75 - Truck Tractor scooter, Motoboard 76 - Two-Axle Truck 95 - Misc. -

EMERGENCY ROADSIDE ASSISTANCE – Specific for Electric Vehicles
EMERGENCY ROADSIDE ASSISTANCE – Specific for Electric Vehicles Submission from GELCOservices Pty. Ltd. Saturday, 4 August 2018 Submission Background: A need has been identified by the Emergency Roadside Assistance (ERA) industry globally, for a portable and cost effective way to charge a depleted Battery Electric Vehicle (BEV/EV) at roadside throughout various countries in Europe. EV Sales in Europe are by far the highest per capita of any continents in the world and as a result the EV driving and operating experience is quite mature when compared to Australia. The EV population is rapidly growing and with this growth comes the problem of how to offer an effective and highly efficient ERA attendance by a mobile facility to quickly deliver a small charge to then enable the EV to drive to a destination charge station for further charge levels. Currently the only ERA practice is for a tow to home or other location for recharge which may present considerable driver inconvenience. The experience and innovative design of the mobile EV “self-recovery” system as developed in Adelaide now means that as the Australian envisaged uptake of BEV increases the ERA service providers will have access to a proven and fully supported Mobile Electric vehicle Service equipment offer to enhance their customers confidence when driving their EV. A South Australian company – GELCOservices - has launched in conjunction with Club Logistics Services, a recently developed totally portable Electric Vehicle (EV) recharge system designed to enable a stranded EV driver who has a depleted high voltage battery to receive a charge at roadside for a short period of time and thus allowing the EV to “self-recover” from a roadside breakdown flat battery incident. -

TR Body Styles-Category Codes
T & R BODY STYLES / CATEGORY CODES Revised 09/21/2018 Passenger Code Mobile Homes Code Ambulance AM Special SP Modular Building MB Convertible CV Station Wagon * SW includes SW Mobile Home MH body style for a Sport Utility Vehicle (SUV). Convertible 2 Dr 2DCV Station Wagon 2 Dr 2DSW Office Trailer OT Convertible 3 Dr 3DCV Station Wagon 3 Dr 3DSW Park Model Trailer PT Convertible 4 Dr 4DCV Station Wagon 4 Dr 4DSW Trailers Code Convertible 5 Dr 5DCV Station Wagon 5 Dr 5DSW Van Trailer VNTL Coupe CP Van 1/2 Ton 12VN Dump Trailer DPTL Dune Buggy DBUG Van 3/4 Ton 34VN Livestock Trailer LS Hardtop HT Trucks Code Logging Trailer LP Hardtop 2 Dr 2DHT Armored Truck AR Travel Trailer TV Hardtop 3 Dr 3DHT Auto Carrier AC Utility Trailer UT Hardtop 4 Dr 4DHT Beverage Rack BR Tank Trailer TNTL Hardtop 5 Dr 5DHT Bus BS Motorcycles Code Hatchback HB Cab & Chassis CB All Terrain Cycle ATC Hatchback 2 Dr 2DHB Concrete or Transit Mixer CM All Terrain Vehicle ATV Hatchback 3 Dr 3DHB Crane CR Golf Cart GC Hatchback 4 Dr 4DHB Drilling Truck DRTK MC with Unique Modifications MCSP Hatchback 5 Dr 5DHB Dump Truck DP Moped MP Hearse HR Fire Truck FT Motorcycle MC Jeep JP Flatbed or Platform FB Neighborhood Electric Vehicle NEV Liftback LB Garbage or Refuse GG Wheel Chair/ Motorcycle Vehicle WCMC Liftback 2 Dr 2DLB Glass Rack GR Liftback 3 Dr 3DLB Grain GN Liftback 4 Dr 4DLB Hopper HO Liftback 5 Dr 5DLB Lunch Wagon LW Limousine LM Open Seed Truck OS Motorized Home MHA Panel PN Motorized Home MHB Pickup 1 Ton 1TPU Motorized Home MHC Refrigerated Van RF Pickup PU -

Vehicle Registration Category and Body Type Examples
Vehicle Registration Category and Body Type Examples Registration Category Description Body Type Body Type Comments Ambulance Heavy Ambulance GVM over 4.5 tonnes Ambulance GVM up to and including 4.5 tonnes Bus GVM up to and including 4.5 tonnes Minibus GVM up to and including 4.5 tonnes Panel Van GVM up to and including 4.5 tonnes Wagon GVM up to and including 4.5 tonnes Articulated Truck Dual Purpose Truck GVM over 4.5 tonnes Prime Mover GVM over 4.5 tonnes Truck Cab'N'Chassis GVM over 4.5 tonnes Bus Minibus GVM from 4.01 tonnes up to & including 4.5 tonnes Stretch Limousine GVM from 4.01 tonnes up to & including 4.5 tonnes Wagon GVM from 4.01 tonnes up to & including 4.5 tonnes Articulated Bus GVM over 4.5 tonnes Bus GVM over 4.5 tonnes Truck Bus GVM over 4.5 tonnes Campervan/Motorhome Campervan GVM from 4.01 tonnes up to & including 4.5 tonnes Minibus GVM from 4.01 tonnes up to & including 4.5 tonnes Bus GVM over 4.5 tonnes Truk Based Motorhome GVM over 4.5 tonnes Conditional Registration Artc Water Trk E/D Restricted to 1-3 area zones Backhoe Loader Restricted to 1-3 area zones Bale Wagon Restricted to 1-3 area zones Bike Off Road Restricted to 1-3 area zones Break Pusher Restricted to 1-3 area zones Bunker Rake Restricted to 1-3 area zones Cane Plant Loader Restricted to 1-3 area zones Cane Planter Track Restricted to 1-3 area zones Chip Spreader Wheel Restricted to 1-3 area zones Compactor L/Fil Soil Restricted to 1-3 area zones Dozer Crawler/Loader Restricted to 1-3 area zones Drill\Driv Rig Track Restricted to 1-3 area zones -

Title Manual Vehicle Services Bureau
Title Manual Vehicle Services Bureau 302 N Roberts, Helena, MT 59620-1431 Phone (406) 444-3661 Fax (406) 444-0166 [email protected] Table of Contents Break/Bond Titles [Rev. 12/23/19] ...................................................................................................................... 4 Bonded Antique and Vintage Vehicle Title ............................................................................ 4 Bonded Out-of-State Title [Rev. 7/24/13] ........................................................................... 4 Campers – Slide In............................................................................................................................................... 4 Certificates of Title [Rev. 02/01/2021]Transferring Ownership [Rev. 03/31/2021 ] ......................................... 5 Cancellation of Title .......................................................................................................... 5 Ownership Documents Accepted for an Original Montana Title [Rev. 02/01/2021] .................... 5 Affidavits [Rev. 12/7/20] .................................................................................................. 5 Canadian and Other Foreign Vehicles [Rev. 12/23/19] .......................................................... 7 Divorces .......................................................................................................................... 9 Donated Vehicle .............................................................................................................. -

Sau1305-Automotive Chassis Design
SCHOOL OF MECHANICAL ENGINEERING DEPARTMENT OF AUTOMOBILE ENGINEERING SAU1305 -AUTOMOTIVE CHASSIS DESIGN 1 UNIT 1 - INTRODUCTION TO ERGONOMICS 2 UNIT 1 1. Introduction: The word “Ergonomics” originated from two Greek words “Ergon” means “work” and“Nomos” means“natural laws” International Ergonomics Association (IEA) defined Ergonomics (or human factors) as the scientific discipline concerned with the understanding of interactions among humans and other elements of a system, and the profession that applies theory, principles, data and methods to design in order to optimize human well-being and overall system performance. An ergonomist is an individual whose knowledge and skills concern the analysis of human-system interaction and the design of the system in order to optimize human well-being and overall system performance (IEA, 2000). Fig: 1 vehicle package layout Ergonomics: Ergonomics is concerned with the health of the people and the productivity of the system. It is to get proper fit between people and their technological tools and environments. It takes account of the user's capabilities and limitations in seeking to ensure that tasks, equipment, information and the environment suit each user. Simply expressed we can say that Ergonomics is fitting the task to the person rather than fitting the person to the task. Domains of Specialization: According to international Ergonomics Association (IEA) ergonomics can be broadly classified into: • Physical Ergonomics • Cognitive Ergonomics 3 • Organizational Ergonomics Physical Ergonomics: It is concerned with human anatomical, anthropometric, physiological and biomechanical characteristics as they related to physical activity. Relevant topics may include working postures, material handling, repetitive movements, work related musculoskeletal disorders, workplace layout, health and safety. -
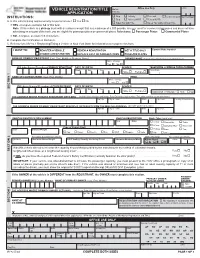
Vehicle Registration/Title Application
Office Use Only Class VEHICLE REGISTRATION/TITLE Batch APPLICATION File No. o Orig o Activity o Renewal o INSTRUCTIONS: Lease Buyout Three of Name o Dup o Activity W/RR o Renew W/RR A. Is this vehicle being registered only for personal use? o Yes o No o Sales Tax with Title o Sales Tax Only without Title If YES - Complete sections 1-4 of this form. Note: If this vehicle is a pick-up truck with an unladen weight that is a maximum of 6,000 pounds, is never used for commercial purposes and does not have advertising on any part of the truck, you are eligible for passenger plates or commercial plates. Select one: o Passenger Plates o Commercial Plates If NO - Complete sections 1-5 of this form. B. Complete the Certification in Section 6. C. Refer to form MV-82.1 Registering/Titling a Vehicle in New York State for information to complete this form. I WANT TO: REGISTER A VEHICLE RENEW A REGISTRATION GET A TITLE ONLY Current Plate Number CHANGE A REGISTRATION REPLACE LOST OR DAMAGED ITEMS TRANSFER PLATES NAME OF PRIMARY REGISTRANT (Last, First, Middle or Business Name) FORMER NAME (If name was changed you must present proof) Name Change Yes o No o NYS driver license ID number of PRIMARY REGISTRANT DATE OF BIRTH GENDER TELEPHONE or MOBILE PHONE NUMBER Month Day Year Area Code o o Male Female ( ) NAME OF CO-REGISTRANT (Last, First, Middle) EMAIL Name Change Yes o No o NYS driver license ID number of CO-REGISTRANT DATE OF BIRTH GENDER SECTION 1 Month Day Year Male o Female o ADDRESS CHANGE? o YES o NO THE ADDRESS WHERE PRIMARY REGISTRANT GETS MAIL (Include Street Number and Name, Rural Delivery or box number. -

Developing Markets for Zero-Emission Vehicles in Goods Movement a Research Report from the National Center March 2018 for Sustainable Transportation
Developing Markets for Zero-Emission Vehicles in Goods Movement A Research Report from the National Center March 2018 for Sustainable Transportation Genevieve Giuliano, University of Southern California Lee White, University of Southern California Sue Dexter, University of Southern California About the National Center for Sustainable Transportation The National Center for Sustainable Transportation is a consortium of leading universities committed to advancing an environmentally sustainable transportation system through cutting- edge research, direct policy engagement, and education of our future leaders. Consortium members include: University of California, Davis; University of California, Riverside; University of Southern California; California State University, Long Beach; Georgia Institute of Technology; and University of Vermont. More information can be found at: ncst.ucdavis.edu. Disclaimer The contents of this report reflect the views of the authors, who are responsible for the facts and the accuracy of the information presented herein. This document is disseminated under the sponsorship of the United States Department of Transportation’s University Transportation Centers program, in the interest of information exchange. The U.S. Government and the State of California assumes no liability for the contents or use thereof. Nor does the content necessarily reflect the official views or policies of the U.S. Government and the State of California. This report does not constitute a standard, specification, or regulation. This report does not constitute an endorsement by the California Department of Transportation (Caltrans) of any product described herein. Acknowledgments This study was funded by a grant from the National Center for Sustainable Transportation (NCST), supported by USDOT and Caltrans through the University Transportation Centers program. -
Non-Preference Towing Contract
DESCHUTES COUNTY SHERIFF’S OFFICE REQUEST FOR APPLICATION AND BID PACKET The Deschutes County Sheriff’s Office is accepting applications and bid packets from tow companies to be placed on the Sheriff’s Office non-preference tow list. The application and bid packet is available at our website, https://sheriff.deschutes.org/community/public-notices/, or a packet can be picked up at the main office in Bend. Please contact Lieutenant Joe DeLuca to schedule pick up a packet or if you have questions at 541-312-6020. DUE DATE: SEPTEMBER 30, 2020 at 5:00 PM To be considered, your application and bid packet must be received by the Sheriff’s Office on or before the due date listed above. You may email your application packet to [email protected] attention Jennifer Hill, mail the packet or drop it off at the Sheriff’s main office: Deschutes County Sheriff’s Office Attn: Jennifer Hill 63333 Highway 20 Bend, OR 97703 AN INCOMPLETE PACKET MAY DISQUALIFY THE APPLICANT TOW COMPANY FROM THE PROCESS. Any and all packets may be rejected for good cause upon a finding that it is in the public interest to do so. The evaluation of the packets will take into consideration the applicant’s: • Application and bid • Experience • Qualifications • Costs for service • Ability to meet the listed towing and storage requirements If selected for a contract, tow companies must comply with requirements listed in the sample contract. Contract exhibits may change during contract negotiations. Required Documentation 1. Complete Application for Towing (Form A). 2. Form B, Criminal Records/Driving History Check for each owner, driver, and anyone associated with the company 3. -

Tow Truck Exemption
Note: New York City businesses must comply with all relevant federal, state, and City laws and rules. All laws and rules of the City of New York, including the Consumer Protection Law and Rules, are available through the Public Access Portal, which businesses can access by visiting www.nyc.gov/consumers. For convenience, sections of the relevant New York City Law and Rules are included as a handout in this packet. The Law and Rules are current as of May 2014. Please note that businesses are responsible for knowing and complying with the most current laws, including any City Council amendments. The Department of Consumer Affairs (DCA) is not responsible for errors or omissions in the handout provided in this packet. The information is not legal advice. You can only obtain legal advice from a lawyer. NEW YORK CITY ADMINISTRATIVE CODE TITLE 20: CONSUMER AFFAIRS CHAPTER 2: LICENSES SUBCHAPTER 31: TOWING VEHICLES § 20-495 Definitions. For purposes of this subchapter, the following terms shall have the following meanings: a. "Disabled vehicle" shall mean any vehicle for which towing is necessary because of a vehicular accident or for which towing is necessary because of the vehicle's inability to proceed under its own motive power due to reasons other than a vehicular accident. b. "Evidence vehicle" shall mean any vehicle which is suspected of having been used as a means of committing a crime or employed in aid or furtherance of a crime or held, used or sold in violation of law or which may be required to be held or produced as evidence in a criminal investigation or proceeding. -

2011 Ford F550 4X4 Diesel 6.7L Jerr-Dan Rollback Tow Truck Only 57K Miles
njtruckking.com King of Cars and 856-381-6621 Trucks 1229 Broadway Westville, New Jersey 08093 2011 FORD F550 4X4 DIESEL 6.7L JERR-DAN ROLLBACK TOW TRUCK ONLY 57K MILES View this car on our website at njtruckking.com/6915177/ebrochure Our Price $49,900 Specifications: Year: 2011 VIN: 1FDUF5HT1BEA87386 Make: FORD F550 4X4 DIESEL Model/Trim: 6.7L JERR-DAN ROLLBACK TOW TRUCK ONLY 57K MILES Condition: Pre-Owned Body: Pickup Truck Exterior: White Engine: 6.7L OHV 32-VALVE V8 POWER STROKE DIESEL ENGINE Interior: Gray Mileage: 57,630 Drivetrain: 4 Wheel Drive 4X4 DIESEL ROLLBACK 2011 FORD F-550 ROLLBACK 6.7L POWERSTROKE TURBO DIESEL AUTOMATIC TRANSMISSION 1-OWNER ! ( ONLY 57,630 ORIGINAL / ACTUAL MILES ) POWER OPTIONS ALCOA'S NEW FRONT TIRES METICULOUSLY MAINTAINED OWNER/OPERATOR TRUCK JERR-DAN 96"X19' ALUMINUM BED REMOVABLE RAILS WHEELIFT DUAL TOOLBOX'S DUAL CONTROLS RUNS AND DRIVES LIKE NEW AND TIGHT! RUNS AND DRIVES LIKE NEW AND TIGHT! THIS TRUCK IS IN EXCELLENT CONDITION ! ONLY 57K MILES!! WHY BUY NEW! SAVE THOUSANDS AND THOUSANDS!! WILL NOT LAST ! BEST OF THE BEST $49,900 CALL / TEXT ROB 856-381-6621 WITH ANY QUESTIONS 2011 FORD F550 4X4 DIESEL 6.7L JERR-DAN ROLLBACK TOW TRUCK ONLY 57K MILES King of Cars and Trucks - 856-381-6621 - View this car on our website at njtruckking.com/6915177/ebrochure Our Location : 2011 FORD F550 4X4 DIESEL 6.7L JERR-DAN ROLLBACK TOW TRUCK ONLY 57K MILES King of Cars and Trucks - 856-381-6621 - View this car on our website at njtruckking.com/6915177/ebrochure Installed Options Interior - Color-coordinated vinyl