Lewisham and Greenwich Nhs Trust Trust Strategy, 2021
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

HMCS Estate by Region & Estates
Her Majesty’s Courts Service Estate by Region and Area London Region (Civil and Family) London Region (Crime) v Barnet Enfield v Edmonton L Barnet Wood Green L Romford Harrow Hendon Haringey G3 Waltham Forest Havering L v v v Snaresbrook v G3 v Highbury Corner Ilford G3 Redbridge Clerkenwell & Shoreditch Brent v Thames Willesden L Berwick upon Tweed v v L (Gee Street) Bow v Barking Uxbridge PRFD L L v Uxbridge L v RCJ Stratford v West London Central London S v L L RCJ Mayor's & City of London Ealing Marylebone IL&CFP Central Criminal Court v L Acton v v G2 vCity of London v v Middlesex Guildhall v IL&CFP Woolwich v G3 GSouthwark Woolwich Brentford Brentford 3 L Isleworth Horseferry Rd.v G3 vTower Bridge G3 v L Lambeth G v v Blackfriars G3 L 3 West London Inner London Sessions House Wandsworth Richmond Upon Thames South Western v v L v v Camberwell Green Greenwich Bexley Hounslow South West Balham v v Alnwick v Wimbledon Kingston Upon Thames North West Region Kingston Upon Thames v Bromley v Bromley L L G3 v v Croydon Croydon L Sutton G3 v v Morpeth L Bedlington v Gosforth v Hexham Newcastle upon Tyne v Blaydonv I1 v Lv North Shields Carlisle GatesheadLv LvSouth Shields I1 v Chester Le Street LvSunderland ConsettLv v vHoughton Le Spring Durham Peterlee G3 Lv Bishop Auckland v Symbol Legend Lv Hartlepool Workington Penrith Newton Aycliffe Lv v Lv v North East Region G Crown Court Darlington Whitehaven Lv Teesside First, Second, Third Guisborough G1 G2 G3 Lv I1 v v Whitby I Combined Court Centre v I1 First, I 2 Second, I 3 Third Kendal Lv -

London Borough of Lewisham Catford Retail and Economic Impact Assessment Final Report for Consultation
Peter Brett Associates LLP 16 Brewhouse Yard London EC1V 4LJ t: 020 7566 8600 London Borough of Lewisham Catford Retail and Economic Impact Assessment Final Report for Consultation Final Report for Consultation January 2013 Peter Brett Associates LLP disclaims any responsibility to the Client and others in respect of any matters outside the scope of this report. This report has been prepared with reasonable skill, care and diligence within the terms of the Contract with the Client and generally in accordance with the appropriate ACE Agreement and taking account of the manpower, resources, investigations and testing devoted to it by agreement with the Client. This report is confidential to the Client and Peter Brett Associates LLP accepts no responsibility of whatsoever nature to third parties to whom this report or any part thereof is made known. Any such party relies upon the report at their own risk. © Peter Brett Associates LLP 2013 Job Number 27149-001 CONTENTS EXECUTIVE SUMMARY ..................................................................................................... i-iv 1 INTRODUCTION .................................................................................................................... 1 Terms of reference ................................................................................................................. 1 Challenges for Catford ........................................................................................................... 3 Structure of report ................................................................................................................. -

Buses from North Greenwich Bus Station
Buses from North Greenwich bus station Route finder Day buses including 24-hour services Stratford 108 188 Bus Station Bus route Towards Bus stops Russell Square 108 Lewisham B for British Museum Stratford High Street Stratford D Carpenters Road HOLBORN STRATFORD 129 Greenwich C Holborn Bow River Thames 132 Bexleyheath C Bromley High Street 161 Chislehurst A Aldwych 188 Russell Square C for Covent Garden Bromley-by-Bow and London Transport Museum 422 Bexleyheath B River Thames Coventry Cross Estate The O2 472 Thamesmead A Thames Path North CUTTER LANE Greenwich 486 Bexleyheath B Waterloo Bridge Blackwall Tunnel Pier Emirates East india Dock Road for IMAX Cinema, London Eye Penrose Way Royal Docks and Southbank Centre BLACKWALL TUNNEL Peninsula Waterloo Square Pier Walk E North Mitre Passage Greenwich St George’s Circus D B for Imperial War Museum U River Thames M S I S L T C L A E T B A N I Elephant & Castle F ON N Y 472 I U A W M Y E E Thamesmead LL A Bricklayers Arms W A S Emirates Air Line G H T Town Centre A D N B P Tunnel Y U A P E U R Emirates DM A A S E R W K Avenue K S S Greenwich Tower Bridge Road S T A ID Thamesmead I Y E D Peninsula Crossway Druid Street E THAMESMEAD Bermondsey Thamesmead Millennium Way Boiler House Canada Water Boord Street Thamesmead Millennium Greenwich Peninsula Bentham Road Surrey Quays Shopping Centre John Harris Way Village Odeon Cinema Millennium Primary School Sainsbury’s at Central Way Surrey Quays Blackwall Lane Greenwich Peninsula Greenwich Deptford Evelyn Street 129 Cutty Sark WOOLWICH Woolwich -

Deptford Church Street & Greenwich Pumping Station
DEPTFORD CHURCH STREET & GREENWICH PUMPING STATION ONLINE COMMUNITY LIAISON WORKING GROUP 13 July 2021 STAFF Chair: Mehboob Khan Tideway • Darren Kehoe, Project Manager Greenwich • Anil Dhillon, Project Manager Deptford • Natasha Rudat • Emily Black CVB – main works contractor • Audric Rivaud, Deptford Church Street Site Manager • Anna Fish– Deptford Church Street, Environmental Advisor • Robert Margariti-Smith, Greenwich, Tunnel & Site Manager • Rebecca Oyibo • Joe Selwood AGENDA Deptford Update • Works update • Looking ahead • Noise and vibration Greenwich Update • Works update • Looking ahead • Noise and vibration Community Investment Community Feedback / Questions DEPTFORD CHURCH STREET WHAT WE’RE BUILDING DEPTFORD WORKS UPDATE SHAFT & CULVERT Shaft • Vortex pipe installed and secondary lining complete • Tunnel Boring Machine crossing complete • Vortex generator works on-going Culvert • Excavation complete • Base slab and walls complete • Opening to shaft complete DEPTFORD WORKS UPDATE COMBINED SEWER OVERFLOW (CSO) CSO Phase 1: Interception Chamber • Internal walls and roof complete • Mechanical, Electrical, Instrumentation, Controls, Automation (MEICA) equipment installation on-going CSO Phase 2: Sewer connection • Protection works of Deptford Green Foul Sewer complete • Secant piling works complete • Capping beam and excavation to Deptford Storm Relief Sewer on-going time hours: Monday to Friday: 22:00 to 08:00 DEPTFORD 12 MONTHS LOOK AHEAD WHAT TO EXPECT AT DEPTFORD CSO: connection to existing sewer Mitigations • This work will take place over a 10 hour shift – the time of the shift • Method of works chosen to limit noise will be dependent on the tidal restrictions in the Deptford Storm Relief Sewer’ generation such as sawing concrete into • Lights to illuminate works and walkways after dark blocks easily transportable off site. -

WOOLWICH and ELTHAM SUNDAY FOOTBALL ALLIANCE Founded 2006
WOOLWICH AND ELTHAM SUNDAY FOOTBALL ALLIANCE Founded 2006 APPLICATION FORM INFORMATION 2016-2017 INCORPORATING THE PLUMSTEAD CHALLENGE CUP THIS ALLIANCE WAS FORMED BY THE WOOLWICH AND DISTRICT SUNDAY FOOTBALL LEAGUE (FORMED 1891) AND THE ELTHAM AND DISTRICT SUNDAY FOOTBALL LEAGUE (FORMED 1959) AFFILIATED TO THE LONDON FOOTBALL ASSOCIATION WOOLWICH AND ELTHAM SUNDAY FOOTBALL ALLIANCE Founded 2006 (INCORPORATING THE PLUMSTEAD CHALLENGE CUP) Unless stated, all correspondence should be addressed to the Hon. League Secretary Hon. Chairman Mr Shayne Hoadley 07985 807174 [email protected] Hon. Deputy Chairman Dear Applicant, Mr Dave Fone 07957 376392 [email protected] APPLICATION FOR MEMBERSHIP Hon. League Secretary Mr Jason Verrillo 07795 956379 [email protected] We refer to your recent enquiry. Hon. Treasurer Mrs Steph Pinner 07951 219531 In this downloaded document you will find the application “pack” information and [email protected] instructions. Hon. Referees’ & Interim Fixtures Secretary Mr David Hooker Please ensure that where possible, ALL questions are completed. Please note that 07766 541061 [email protected] or we are a Sunday morning football league and therefore our kick off times are [email protected] 10:30am apart from Cup Finals and the occasional fixture. Hon. Assistant Referees’ Secretary Mr Stuart Axford 07958 287924 Upon the completion and return of this application form you will be contacted and [email protected] advised to attend an interview with the Management Committee. Details of the date, Hon. Registration Secretary Mrs Kelly Hooker time and location will be provided. 07722 271194 [email protected] Hon. Results Secretary Please ensure you bring with you the £20.00 application fee on the day of interview Ms Lisa Brooks or post it along with this form to the League Secretary. -

Working Together to Tackle Poverty in Lewisham
Working together to tackle poverty in Lewisham The final report of the Lewisham Poverty Commission October 2017 Contents Foreword 3 1. Introducing the Poverty Commission: a realistic but ambitious approach 4 The Commission 4 Focusing on poverty 4 The role of Lewisham Council in tackling poverty 5 Action at a local level 5 Working together to tackle poverty 5 2. Poverty in Lewisham 6 Lewisham and its people 6 The impacts of poverty 6 Quantifying poverty in Lewisham 8 The difficulties in getting well-paid, secure work 10 Children living in poverty 13 The price of unaffordable housing 14 The Commission’s focus 14 3. Supporting residents to access well-paid, secure jobs inside and outside of Lewisham 15 Works, skills and the role of anchor institutions 15 Recommendations 17 4. Tackling child poverty by supporting parents into decent work 20 Child poverty, child care and lone parent unemployment 20 Recommendations 21 5. Improving the local housing market 23 Housing in Lewisham 23 Recommendations 24 6. Strengthening support within communities 27 Increasing community resilience 27 Recommendations 29 7. Working together to tackle poverty: next steps and implementation 31 An immediate response 31 Change across the community 31 Advising national government 31 Staying the course 31 Appendix 1: Listening to Lewisham’s people and its organisations 32 Our approach to consultation and engagement 32 Further data and evidence 33 Summary of comments received from residents 34 2 Foreword Lewisham is a great place to live, with a strong and diverse community. Yet, despite being situated in the heart of London, on the doorsteps of one of the wealthiest cities in the world, tens of thousands of Lewisham residents live in poverty. -

Unit 1 Hope Wharf, 37 Greenwich High Road, London SE10 8LR Long Let Nursery in Greenwich (15 Year Lease with RPI Linked Reviews)
Unit 1 Hope Wharf, 37 Greenwich High Road, London SE10 8LR Long let Nursery in Greenwich (15 year lease with RPI linked reviews) Investment Highlights Offers in excess of £625,000 • Newly constructed nursery let on a new 15 year lease • Situated within a prominent residential development in Greenwich, London • 1,491 sq ft of ground floor accommodation with outdoor space and car parking Income • Let to ‘Twinnie Day Nursery Limited’ for 15 years (without £40,000 break) at a passing rent of £40,000 per annum • 5 yearly rent reviews to the higher of RPI (collar and cap of 2% and 4%) and the open market rent. • Excellent transport links to Central London with nearby stations including Greenwich Station and Deptford Bridge DLR NIY 6.10% Location Situation London Borough of Greenwich has a population of The property is situation on Hope Wharf which is 254,557 residents (2011 census). Greenwich has located on Greenwich High Road in close proximity experienced extensive regeneration over the last 2 to both Greenwich Station and Deptford Bridge decades and attracted a large amount of DLR, both of which provide access to Central investment into the locality, including developments London and Canary Wharf. such as the New Capital Quay and the Greenwich Peninsula. Transport Links Distance Greenwich is strategically located to the south east Deptford Bridge DLR 0.2 miles of Central London with excellent transport links via Greenwich Station 0.4 miles Greenwich Station (National Rail) and Deptford A2 120 yards Bridge DLR. The area is best known for the National Maritime There’s a variety of restaurants, bars, shops and Museum, Royal Observatory, Cutty Sark and the markets nearby, including the well known Cutty O2 Arena, which attract over a million tourist each Sark and Greenwich Market which is just over a 15 year. -

Mary Ney Chief Executive the Royal Borough of Greenwich Woolwich Town Hall 16 April 2014 Wellington Street Woolwich London
Mary Ney Chief Executive The Royal Borough of Greenwich Woolwich Town Hall 16 April 2014 Wellington Street Woolwich London. SE18 6PW Via email [email protected] Dear Ms Ney, THE LOCAL GOVERNMENT ACT 1986 NOTICE UNDER SECTION 4A(5) I enclose a written notice to your authority of a proposed direction which the Secretary of State for Communities and Local Government is minded to give to your authority under section 4A of the Local Government Act 1986. Yours sincerely, Paul Rowsell Paul Rowsell Tel 0303 44 42005 Deputy Director – Democracy Email [email protected] Department for Communities and Local Government 3/J1, Eland House Bressenden Place London SW1E 5DU THE LOCAL GOVERNMENT ACT 1986 NOTICE UNDER SECTION 4A(5) The Secretary of State hereby gives the local authority known as the Royal Borough of Greenwich notice of a direction that he proposes to give to the authority under section 4A of the 1986 Act. Having regard to the information available to him about the local authority’s publicity, the Secretary of State proposes to direct the Royal Borough of Greenwich to comply by no later than 1 May 2014 with all of the provisions of the Recommended Code of Practice on Local Authority Publicity issued under section 4 of the Local Government Act 1986 on 31 March 2011 having been approved by a resolution of each House of Parliament. The Royal Borough of Greenwich may make written representations to the Secretary of State about the proposed direction within the period of 14 days beginning with the day on which this notice is given to it. -
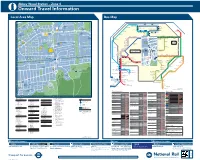
Abbey Wood Station – Zone 4 I Onward Travel Information Local Area Map Bus Map
Abbey Wood Station – Zone 4 i Onward Travel Information Local Area Map Bus Map 45 1 HARTSLOCK DRIVE TICKFORD CLOSE Y 1 GROVEBURY ROAD OAD 16 A ALK 25 River Thames 59 W AMPLEFORTH R AMPLEFORTH ROAD 16 Southmere Central Way S T. K A Crossway R 1 B I N S E Y W STANBROOK ROAD TAVY BRIDGE Linton Mead Primary School Hoveton Road O Village A B B E Y W 12 Footbridge T H E R I N E S N SEACOURT ROAD M E R E R O A D M I C H A E L’ S CLOSE A S T. AY ST. MARTINS CLOSE 1 127 SEWELL ROAD 1 15 Abbey 177 229 401 B11 MOUNTJOYCLOSE M Southmere Wood Park ROAD Steps Pumping GrGroroovoveburyryy RRoaadd Willow Bank Thamesmead Primary School Crossway Station W 1 Town Centre River Thames PANFIE 15 Central Way ANDW Nickelby Close 165 ST. HELENS ROAD CLO 113 O 99 18 Watersmeet Place 51 S ELL D R I V E Bentham Road E GODSTOW ROAD R S O U T H M E R E L D R O A 140 100 Crossway R Gallions Reach Health Centre 1 25 48 Emmanuel Baptist Manordene Road 79 STANBROOK ROAD 111 Abbey Wood A D Surgery 33 Church Bentham Road THAMESMEAD H Lakeside Crossway 165 1 Health Centre Footbridge Hawksmoor School 180 20 Lister Walk Abbey Y GODSTOW ROAD Footbridge N1 Belvedere BUR AY Central Way Wood Park OVE GROVEBURY ROAD Footbridge Y A R N T O N W Y GR ROAD A Industrial Area 242 Footbridge R Grasshaven Way Y A R N T O N W AY N 149 8 T Bentham Road Thamesmead 38 O EYNSHAM DRIVE Games N Southwood Road Bentham Road Crossway Crossway Court 109 W Poplar Place Curlew Close PANFIELD ROAD Limestone A Carlyle Road 73 Pet Aid Centre W O LV E R C O T E R O A D Y 78 7 21 Community 36 Bentham Road -
South East London Green Chain Plus Area Framework in 2007, Substantial Progress Has Been Made in the Development of the Open Space Network in the Area
All South East London Green London Chain Plus Green Area Framework Grid 6 Contents 1 Foreword and Introduction 2 All London Green Grid Vision and Methodology 3 ALGG Framework Plan 4 ALGG Area Frameworks 5 ALGG Governance 6 Area Strategy 8 Area Description 9 Strategic Context 10 Vision 12 Objectives 14 Opportunities 16 Project Identification 18 Project Update 20 Clusters 22 Projects Map 24 Rolling Projects List 28 Phase Two Early Delivery 30 Project Details 50 Forward Strategy 52 Gap Analysis 53 Recommendations 56 Appendices 56 Baseline Description 58 ALGG SPG Chapter 5 GGA06 Links 60 Group Membership Note: This area framework should be read in tandem with All London Green Grid SPG Chapter 5 for GGA06 which contains statements in respect of Area Description, Strategic Corridors, Links and Opportunities. The ALGG SPG document is guidance that is supplementary to London Plan policies. While it does not have the same formal development plan status as these policies, it has been formally adopted by the Mayor as supplementary guidance under his powers under the Greater London Authority Act 1999 (as amended). Adoption followed a period of public consultation, and a summary of the comments received and the responses of the Mayor to those comments is available on the Greater London Authority website. It will therefore be a material consideration in drawing up development plan documents and in taking planning decisions. The All London Green Grid SPG was developed in parallel with the area frameworks it can be found at the following link: http://www. london.gov.uk/publication/all-london-green-grid-spg . -

Directory of Services
Directory of Services Substance Misuse support for Residents of the Royal Borough of Greenwich Opiates and Alcohol support for dependent users CRi Aspire Service Support available: Day programme, one to one support, access to prescribing, 821 Woolwich Road, group work, access to community detox, referrals for residential treatment, key working, psychology support, peer mentoring, workshops, recovery community, Charlton SE7 8JL complimentary therapies and pre detox group. Open access drop in available every Tel: 020 8316 0116 day between 10 am - 12pm Individuals with complex support needs will be referred onto the specialist service at The Beresford Project. Cannabis, cocaine and other drugs - Non dependent users Lifeline BaSIS project Support available: Brief advice and information, motivational interviewing, goal Royal Arsenal Medical Centre setting, healthy living tips, self management techniques, acupuncture, group work. 21 Arsenal Way , Woolwich Brief support available for between one to twelve weeks dependent on need. London SE18 6TE Support for users of Cocaine, MDMA, Cannabis, Ketamine, Legal Highs, Methadrone, other Club Drugs and Alcohol. Open access drop in available 9am and 4:30pm Mon Tel: 020 3696 2640 - Fri and 9.30am - 12.30pm Sat Email: [email protected] Older Drinkers - over 55s Silver Lining Project Community and therapeutic support, key working, one to one support, group work, peer mentoring. Home visits (where appropriate and available). Referrals to other 2-6 Sherard Road, services including CRi Aspire -for community detox and access to residential Eltham, treatment. London SE9 Please call to make a referral or an appointment Tel: 079020 876 983 Email: [email protected] Family and Carer support Specialist family support workers from ADFAM are available within our Aspire ADFAM services. -

Planning Application Design & Access Statement Van-0387
PLANNING APPLICATION DESIGN & ACCESS STATEMENT VAN-0387 53 PERRY VALE, FOREST HILL, LONDON, SE23 2NE SEPTEMBER 2018 1.0 Contents VAN-0387 – 53 Perry Vale, Forest Hill, SE23 2NE, London Borough of Lewisham Design and Access Statement, July 2018 1.0 Contents 1 2.0 Introduction 2 3.0 Site analysis and Current Building 5 4.0 Description of the proposal 7 5.0 Use and Layout 10 6.0 Heritage Statement 12 7.0 Planning History and Policies 15 8.0 Architectural Character and Materials 15 9.0 Landscaping and Trees 19 10.0 Ecology 19 11.0 Extract, Ventilation and Services 20 12.0 Cycle Storage and Refuse 20 13.0 Sustainability and Renewable Energy Technology 21 14.0 Access & Mobility Statement 21 15.0 Transport, Traffic and parking Statement 22 16.0 Acoustics 22 17.0 Flood Risk 22 18.0 Statement of Community Engagement 23 19.0 Conclusion 24 1 2.0 Introduction VAN-0387 – 53 Perry Vale, Forest Hill, SE23 2NE, London Borough of Lewisham Design and Access Statement, July 2018 This application submission is prepared by db architects on behalf of Vanquish Iconic Developments for the site at 53 Perry Vale, Forest Hill, SE23 2NE. Vanquish are a family-run business and have been creating urban industrial interior designed developments for many years now across South East London. "We are a firm believer that property development should be creative, not made with basic materials to fit the standard criteria of a build. This is reflected in our interiors and exteriors of each finished development.