Application for Return to Ohio Wesleyan
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2020-21 Men's Soccer Records
2020-21 Men’s Soccer Records 2020-21 CONTENTS WHY BATTLING BISHOPS? Why Battling Bishops? // 1 The nickname “The Battling Bishops” dates to 1925; before then Ohio Wesleyan University’s 2019 NCAC Standings and Statistics // 2 teams were simply known as “The Red and Black,” Previous NCAC Leaders // 3 or sometimes as “The Methodists.” Ohio Wesleyan is affiliated with the United Methodist Church, Previous NCAC Special Awards // 4 and long has produced many of its bishops. By April, 1925, according to that issue of the NCAC Records // 5 Alumni Magazine, the present name had finally About the NCAC // 6 been derived. “Ohio sports writers have been at OWU Men’s Soccer a loss,” the magazine reported. “There are count- Bishop Soccer Year-by-Year // 7 less colleges throughout the country claiming red NCAA Tournament History // 8-10 and black as their colors, and 14 Methodist col- leges in Ohio alone.” Pi Delta Epsilon journalism Conference Championships // 11 fraternity therefore sponsored a contest, and the winning nickname, “The Battling Bishops,” was Stu Parry Award // 11 “placed before the sports writers of the state as All-Time Series Records // 12-13 the teams’ official title.” Senior Harold Thomas of Lima submitted the winning entry. Ohio Soccer Pioneers // 14 The new nickname must have provided in- All-Time Results // 15-28 spiration. The 1925 football team, under George Gauthier, “The Little Giant,” went 7-1-1. Its only Bishop Records // 29-30 loss came to Ohio State by a 10-3 score, and it tied Syracuse, 3-3, en route to winning the Ohio Confer- Bishop Stat Leaders 1955-2019 // 31-32 ence championship. -

2015-16 Tennis Founded in 1842, Ohio Wesleyan Ohio Wesleyan Employs 146 Full- Is a National University with a Major Time Faculty
2015-16 Tennis Founded in 1842, Ohio Wesleyan Ohio Wesleyan employs 146 full- is a national university with a major time faculty. Nearly 100 percent of international presence. Accredited by Ohio Wesleyan in Brief the tenure-track faculty hold a Ph.D. the North Central Association of Col- or equivalent or are completing work leges and Schools, OWU is a member of LOCATION >> Delaware, Ohio 43015 toward the degree. The student-faculty the Great Lakes Colleges Association, a ratio is 11:1. consortium of 13 leading independent FOUNDED >> 1842 Ohio Wesleyan currently enrolls institutions in Indiana, Michigan, and about 1750 students, almost equally ENROLLMENT 1675 Ohio. >> men and women, from nearly every Ohio Wesleyan has been named state and more than 40 countries. The NICKNAME Battling Bishops to the President’s Higher Education >> multicultural enrollment total of ap- Community Service Honor Roll — the COLORS >> Red and Black proximately 16 percent includes U.S. highest federal recognition a school can multicultural students and interna- achieve for service learning and civic PRESIDENT >> Dr. Rock Jones tional students. engagement — for 6 consecutive years. Diversity, creativity, leadership, Ohio Wesleyan confers the Bach- HOME COURTS >> Luttinger Family and service are emphasized through- elor of Arts, Bachelor of Fine Arts, and Tennis Center out the co-curriculum. Students are Bachelor of Music degrees. The Univer- active in nearly 100 clubs and orga- sity also offers combined-degree (3-2) AFFILIATION >> NCAA Division III nizations, as well as departmental programs in engineering, interdisci- student boards, academic honoraries, CONFERENCE North Coast Athletic plinary and applied science, medical >> music and theatre productions, frater- technology, optometry, and physical nities and sororities, and an extensive WEBSITE www.owu.edu therapy. -

The Wooster Voice
The College of Wooster Open Works The oV ice: 1951-1960 "The oV ice" Student Newspaper Collection 12-6-1957 The oW oster Voice (Wooster, OH), 1957-12-06 Wooster Voice Editors Follow this and additional works at: https://openworks.wooster.edu/voice1951-1960 Recommended Citation Editors, Wooster Voice, "The oosW ter Voice (Wooster, OH), 1957-12-06" (1957). The Voice: 1951-1960. 159. https://openworks.wooster.edu/voice1951-1960/159 This Book is brought to you for free and open access by the "The oV ice" Student Newspaper Collection at Open Works, a service of The oC llege of Wooster Libraries. It has been accepted for inclusion in The oV ice: 1951-1960 by an authorized administrator of Open Works. For more information, please contact [email protected]. Wooster Voice Published by the Students of the College of Wooster Volume LXXII Wooster, Ohio, Friday, December 6, 1957 Number 10 Creates Senate 1 $ - Scot Faculty Scatters For Wooster Day; Required Church Annual Celebration Honors Rededication Study Committee by Cindy Barrett The compulsory church rule is, Wooster Day, December 11, will find many of our for some students, a real probl- em in that it is seen as one faculty members scattered across the nation, addressing cause of the present tension be- many of our approximately 55 Alumni organizations. tween students and the admin- Commemorating the rededication of the college in 1902, istration. For others it means just one year after the college was destroyed by fire, only the slightly troublesome Wooster Day has come to be the high task of writing "Westminster: point toward eight times" on a card once a which the alumni office works : semester. -

Four-Year Course Planning Chart
Ohio Wesleyan University 4-year Planner Student Name _________________________________ Transfer Unit Credit ______________ Majors/Minors __________________________________________________________________ Fall Spring Summer Course Units Course Units Course Units F R E S H M A N Total Units: Total Units: Total Units: S O P H O M O R E Total Units: Total Units: Total Units: J U N I O R Total Units: Total Units: Total Units: S E N I O R Total Units: Total Units: Total Units: This is a tentative plan based on your status as of ______________. Please check with your advisor about scheduling courses and become familiar with competence, distribution, and major/minor requirements. It is your responsibility to meet with your advisor on a regular basis during your years at OWU. Please remember: "Students are ultimately responsible for their own academic program and for meeting the degree requirements" (OWU Catalog). (OVER) CHECKLIST OF ACADEMIC REQUIREMENTS Consult the OWU Catalog for Official Requirements. University Requirements for a BA Degree are: 1. Competence in (or exemption from) English, Foreign Language, Writing, Diversity, and Quantitative Skills; 2. 10 units in the distribution areas I, II, III, and IV [seven units in some majors**]; 3. 34 units of credit total; 31 as full-unit credits or combined 0.5 modulars in the same discipline; 4 15 upper-level units, numbered 250 and above; 5. 16 units taken during 4 semesters in residence at (or under the auspices of) OWU; 6. Completion of any unfinished work (PR, NR, I) or removal of any U in writing; 7. A 2.00 cumulative average for all work taken (excluding C/NE); 8. -

2004/05 Catalog Ohio Wesleyan University Contents
2004/05 Catalog Ohio Wesleyan University Contents Contents While this Catalog presents the best information available at the time of publication, all information contained herein, including statements of fees, course offerings, admission policy, and graduation requirements, is subject to change without notice or obligation. Calendar ......................................................................................................inside back cover The University ......................................................................................................................4 Introduction ......................................................................................................................4 Statement of Aims ............................................................................................................5 Intellectual Freedom and Responsibility ..........................................................................6 Statement on Student Rights ............................................................................................7 The Affirmative Action Plan.............................................................................................8 Policy on Sexual Harassment ...........................................................................................8 Policy on Voluntary Sexual Relationships between Faculty/Staff and Students ..............9 Traditions ........................................................................................................................12 Academic -

Colleges & Universities
Bishop Watterson High School Students Have Been Accepted at These Colleges and Universities Art Institute of Chicago Fordham University Adrian College University of Cincinnati Franciscan University of Steubenville University of Akron Cincinnati Art Institute Franklin and Marshall College University of Alabama The Citadel Franklin University Albion College Claremont McKenna College Furman University Albertus Magnus College Clemson University Gannon University Allegheny College Cleveland Inst. Of Art George Mason University Alma College Cleveland State University George Washington University American Academy of Dramatic Arts Coastal Carolina University Georgetown University American University College of Charleston Georgia Southern University Amherst College University of Colorado at Boulder Georgia Institute of Technology Anderson University (IN) Colorado College University of Georgia Antioch College Colorado State University Gettysburg College Arizona State University Colorado School of Mines Goshen College University of Arizona Columbia College (Chicago) Grinnell College (IA) University of Arkansas Columbia University Hampshire College (MA) Art Academy of Cincinnati Columbus College of Art & Design Hamilton College The Art Institute of California-Hollywood Columbus State Community College Hampton University Ashland University Converse College (SC) Hanover College (IN) Assumption College Cornell University Hamilton College Augustana College Creighton University Harvard University Aurora University University of the Cumberlands Haverford -
Transferring Your F-1 SEVIS Record To
Ohio Wesleyan University INTERNATIONAL STUDENT International Student Services SEVIS 214 Hamilton-Williams Campus Center TRANSFER-OUT 61 South Sandusky Street FORM Delaware, OH 43015 If you are currently attending Ohio Wesleyan University as an international student in F-1 visa status and are planning to transfer to another school in the USA, you must formally notify us of your intent to transfer. Your SEVIS record will not be “transferred-out” until this completed form is received by International Student Services at Ohio Wesleyan University. You should complete this form only after you have been formally notified of your admission to the school and that the school will issue to you a new I-20 form. Part I – Your Personal Information: Your complete name: ______________________________________________________________ Your OWU ID number: _______________ Your SEVIS ID number: _______________________ Part II – Information About the School to Which You Intend to Transfer: Name of school to which you intend to transfer as it appears in SEVIS: _________________________________________________________________________________ School’s SEVIS ID: ________________________________________________________________ Location of school: ________________________________________________________________ Part III -- Instruction to OWU to Transfer My SEVIS Record: I instruct Ohio Wesleyan University transfer my SEVIS record to the above school on the date listed below. I also give Ohio Wesleyan University permission to release any information about myself to the above school as required to facilitate this transfer. I understand that it is my responsibility to maintain my immigration status and insure the accuracy of the above information. I also understand that it may take up to four weeks to process this transfer. I request that my SEVIS record be transferred on this date: _______________________________. -

Member Colleges & Universities
Bringing Colleges & Students Together SAGESholars® Member Colleges & Universities It Is Our Privilege To Partner With 427 Private Colleges & Universities April 2nd, 2021 Alabama Emmanuel College Huntington University Maryland Institute College of Art Faulkner University Morris Brown Indiana Institute of Technology Mount St. Mary’s University Stillman College Oglethorpe University Indiana Wesleyan University Stevenson University Arizona Point University Manchester University Washington Adventist University Benedictine University at Mesa Reinhardt University Marian University Massachusetts Embry-Riddle Aeronautical Savannah College of Art & Design Oakland City University Anna Maria College University - AZ Shorter University Saint Mary’s College Bentley University Grand Canyon University Toccoa Falls College Saint Mary-of-the-Woods College Clark University Prescott College Wesleyan College Taylor University Dean College Arkansas Young Harris College Trine University Eastern Nazarene College Harding University Hawaii University of Evansville Endicott College Lyon College Chaminade University of Honolulu University of Indianapolis Gordon College Ouachita Baptist University Idaho Valparaiso University Lasell University University of the Ozarks Northwest Nazarene University Wabash College Nichols College California Illinois Iowa Northeast Maritime Institute Alliant International University Benedictine University Briar Cliff University Springfield College Azusa Pacific University Blackburn College Buena Vista University Suffolk University California -
2008 Five Colleges of Ohio ABOUT the JUROR 2008, with 51 Works by 46 Students Selected 2008 Five Colleges of Ohio for the Exhibition
ABOUT THE FIVE COLLEGES OF OHIO ACKNOWLEDGMENTS JURIED STUDENT BIENNIAL It is with great anticipation and enthusiasm The Five Colleges of Ohio, Inc., is a that the staff of The College of Wooster Art consortium of five liberal arts colleges in Museum looks forward to The Five Colleges JUROR’S STATEMENT Ohio: Denison University, Granville; of Ohio Juried Student Biennial. Kenyon College, Gambier; Oberlin College, There are several reasons for this Oberlin; Ohio Wesleyan University, anticipation, with two being the energy and The Five Colleges of Ohio Juried Student Delaware; and The College of Wooster, complexity of concept that we see in the Biennial entries impressed me with Wooster. work of these young artists. The other is that some very strong traditional imagery The Five Colleges of Ohio was Doug McGlumphy, preparator at The College and methods, particularly in portraiture, incorporated in 1995, although discussions of Wooster Art Museum, developed the idea while also offering a spicy soupçon of about the creation of a consortial library for this multi-campus juried exhibition. Having contemporary engagements such as the system began several years earlier. According experienced a similar exhibition opportunity as graphic novel format, idiosyncratic spatial to the organization’s statement of purpose: an undergraduate at Washington and Jefferson structures and psychological/fantasy College in Washington, PA, Doug thought that The Five Colleges of Ohio narrative. The range of three-dimensional the Five Colleges consortium could provide consortium was founded in order media included ambitious and apparently the organizing principle for a juried exhibition well-crafted works. I say apparently, to foster closer cooperation and understanding, coordinate operating at Wooster. -

OUT-OF-STATE COLLEGE FAIR —October 2, 2019 6:00-8:00PM
OUT-OF-STATE COLLEGE FAIR —October 2, 2019 6:00-8:00PM MONARCH HIGH SCHOOL, 329 Campus Dr., Louisville, CO 80027 Financial Aid Presentation from 5:15 - 6:00 PM in Auditorium Allegheny College (PA) Cornell College (IA) Kalamazoo College (MI) American University (DC) Cornish College of the Arts (WA) Kansas State University (KS) Arcadia University (PA) Cornish College of the Arts (WA) Kenyon College (OH) Arizona State University (AZ) Creighton University (NE) Knox College (IL) Auburn University (AL) Davidson College (NC) Lake Forest College (IL) Augsburg University (MN) DePaul University (IL) Lawrence University (WI) Augustana University (SD) DePauw University (IN) Lehigh University (PA) Azusa Pacific University (CA) Dickinson College (PA) Lewis & Clark College (OR) Babson College (MA) Doane University (NE) Lewis University (IL) Bard College (NY) Dominican University of California (CA) Linfield College (OR) Bates College (ME) Drake University (IA) Loyola University Chicago (IL) Baylor University (TX) Drexel University (PA) Loyola University New Orleans (LA) Belmont University (TN) Drury University (MO) Luther College (IA) Benedictine College (KS) Duquesne University (PA) Macalester College (MN) Bennington College (VT) Eastern Washington University (WA) Marist College (NY) Binghamton University (NY) Eckerd College (FL) Marquette University (WI) Black Hills State University (SD) Elon University (NC) Maryville University (MO) Boise State University (ID) Embry Riddle Aeronautical University Massachusetts College of Pharmacy Bradley University -
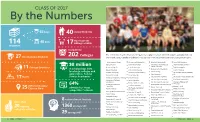
CLASS of 2017 25 $8 Million
CLASS OF 2017 By the Numbers 66 Boys Legacy Students 40 Have Current 48 Girls 114 17 Siblings at WRA STUDENTS Accepted to Colleges The 114 members of the Class of 2017 gained acceptances at 202 different colleges and universities in 27 International Students 202 the United States, Canada and abroad. Their schools of intended matriculation are represented below. The University of Akron University of Colorado (2) New York University (4) Texas A&M University Babson College Connecticut College University of North Carolina Texas Christian University $8 million School of the Arts Foreign Countries Boston College (4) Cornell University Tufts University (2) 11 Northeastern University (2) in scholarships from Boston University Denison University (2) Tulane University Oberlin College local orgs, colleges and Bowdoin College (2) University of Detroit Mercy United States Military Academy Ohio University (2) universities, Federal Bucknell University Drew University States Service Academies Ohio Northern University United States Naval Academy (3) 17 University of California, Irvine (2) Duke University Ohio Wesleyan University Vanderbilt University (2) University of California, Emory University Los Angeles The Ohio State University (6) Virginia Commonwealth Florida Southern College University University of California, Pennsylvania State University (2) 64% Fordham University Santa Cruz Virginia Tech (2) Different Towns/ Purdue University admitted to “most The George Washington 25 Cities in Ohio Carleton College Viterbo University University Rensselaer Polytechnic Institute competitive” schools Carnegie Mellon University (2) Walsh University Hamilton College (2) Rhode Island School of Design Centre College Washington and College of the Holy Cross University of Richmond Jefferson College Champlain College University of Illinois-Chicago Rochester Institute of Washington University in University of Chicago (2) Technology 8 national merit finalists Illinois Institute of Technology St. -

Matriculated to Colleges Outside of Ohio
Five Year Matriculation 2015 - 2019 Institutions with five or more matriculants are listed in bold print. The University of Akron Gannon University Purdue University The University of Alabama The George Washington University Queen’s University Allegheny College Georgetown University Rensselaer Polytechnic Institute American University Georgia Institute of Technology Rhode Island School of Design Amherst College University of Georgia Rhodes College Babson College Gettysburg College University of Richmond Baldwin Wallace University University of Glasgow Roanoke College Bard College Grinnell College Robert Morris University Barnard College Hamilton College University of Rochester Bates College University of Hartford Rochester Institute of Technology Belmont University Harvard College Rollins College Berklee College of Music Haverford College Rose-Hulman Institute of Technology Boston College Heidelberg University Royal Holloway, University of London Boston University High Point University Rutgers University Bowdoin College Hiram College Santa Clara University Bowling Green State University Hobart and William Smith Colleges Sarah Lawrence College Bradley University College of the Holy Cross Savannah College of Art and Design Brandeis University University of Illinois-Chicago Sewanee: The University of the South Brown University University of Illinois Sierra Nevada College Bucknell University Illinois Institute of Technology University of Southern California Butler University Imperial College London Southern Methodist University University