MATERNAL SCREENING for FOETAL ABNORMALITY Assessment Assessment
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
First Trimester Anomaly Scan Using Virtual Reality (VR FETUS Study): Study Protocol for a Randomized Clinical Trial C
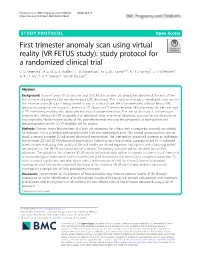
Pietersma et al. BMC Pregnancy and Childbirth (2020) 20:515 https://doi.org/10.1186/s12884-020-03180-8 STUDY PROTOCOL Open Access First trimester anomaly scan using virtual reality (VR FETUS study): study protocol for a randomized clinical trial C. S. Pietersma1, A. G. M. G. J. Mulders1, L. M. Moolenaar1, M. G. M. Hunink2,3,4, A. H. J. Koning5, S. P. Willemsen6, A. T. J. I. Go1, E. A. P. Steegers1 and M. Rousian1* Abstract Background: In recent years it has become clear that fetal anomalies can already be detected at the end of the first trimester of pregnancy by two-dimensional (2D) ultrasound. This is why increasingly in developed countries the first trimester anomaly scan is being offered as part of standard care. We have developed a Virtual Reality (VR) approach to improve the diagnostic abilities of 2D ultrasound. Three-dimensional (3D) ultrasound datasets are used in VR assessment, enabling real depth perception and unique interaction. The aim of this study is to investigate whether first trimester 3D VR ultrasound is of additional value in terms of diagnostic accuracy for the detection of fetal anomalies. Health-related quality of life, cost-effectiveness and also the perspective of both patient and ultrasonographer on the 3D VR modality will be studied. Methods: Women in the first trimester of a high risk pregnancy for a fetus with a congenital anomaly are eligible for inclusion. This is a randomized controlled trial with two intervention arms. The control group receives ‘care as usual’: a second trimester 2D advanced ultrasound examination. The intervention group will undergo an additional first trimester 2D and 3D VR ultrasound examination. -

GMEC) Strategic Clinical Networks Reduced Fetal Movement (RFM
Greater Manchester & Eastern Cheshire (GMEC) Strategic Clinical Networks Reduced Fetal Movement (RFM) in Pregnancy Guidelines March 2019 Version 1.3a GMEC RFM Guideline FINAL V1.3a 130619 Issue Date 15/02/2019 Version V1.3a Status Final Review Date Page 1 of 19 Document Control Ownership Role Department Contact Project Clinical Lead Manchester Academic Health [email protected] Science Centre, Division of Developmental Biology and Medicine Faculty of Biology, Medicine and Health, The University of Manchester. Project Manager GMEC SCN [email protected] Project Officer GMEC SCN [email protected] Endorsement Process Date of Presented for ratification at GMEC SCN Maternity Steering Group on:15th February ratification 2019 Application All Staff Circulation Issue Date: March 2019 Circulated by [email protected] Review Review Date: March 2021 Responsibility of: GMEC Maternity SCN Date placed on March 2019 the Intranet: Acknowledgements On behalf of the Greater Manchester and Eastern Cheshire and Strategic Clinical Networks, I would like to take this opportunity to thank the contributors for their enthusiasm, motivation and dedication in the development of these guidelines. Miss Karen Bancroft Maternity Clinical Lead for the Greater Manchester & Eastern Cheshire SCN GMEC RFM Guideline FINAL V1.3a 130619 Issue Date 15/02/2019 Version V1.3a Status Final Review Date Page 2 of 19 Contents 1 What is this Guideline for and Who should use it? ......................................................................... 4 2 What -

Efficacy of Genetic Testing in Cases of Ambiguous Genitalia
EFFICACY OF GENETIC TESTING IN CASES OF AMBIGUOUS GENITALIA DETECTED ON PRENATAL! ULTRASOUND ! ! ! by! EVELYN ROSE! CRAWFORD ! ! Submitted in partial fulfillment of !the requirements for the degree of Master of! Science ! ! ! Thesis Advisor: Larisa! Baumanis, MS ! ! Genetic Counseling! Department !of Genetics CASE WESTERN RESERVE! UNIVERSITY ! ! ! ! ! ! ! August, 2014 ! ! CASE WESTERN RESERVE! UNIVERSITY SCHOOL OF GRADUATE! STUDIES We hereby approve! the thesis of: Evelyn Rose! Crawford candidate for the degree of !Master of Science degree.* ! ! Larisa Baumanis, MS (Committee Chair) ! Anne Matthews, RN, PhD ! Noam Lazebnik, MD ! Aditi Parikh, MD ! Sara Debanne, PhD ! ! ! ! Date of Defense June 20, 2014 ! ! ! ! ! *We also certify that written approval has been obtained for any proprietary material contained therein !2 ! ! ! TABLE OF CONTENTS List of Tables 4 List of Figures 5 Acknowledgements 6 Abstract 7 Introduction 8 Purpose of Study & Specific Aims 10 Background 11 Detection of Ambiguous Genitalia on Prenatal Ultrasound 11 Current use of Genetic testing in determining a specific diagnosis 13 The Importance of Prenatal Diagnosis in Cases of Ambiguous Genitalia 18 Significance for genetic counselors 19 Conclusions 20 Methodology 22 Systematic Review of the Literature 22 Chart Review 27 Algorithm & Analysis 29 Results 31 Analysis 52 Discussion 55 Appendix I: First Review Matrix Organization and summary of literature review articles 62 Appendix II: Second Review Matrix Organization and summary of case studies from the literature review 78 Appendix III: Third Review Matrix Organization and summary of chart review cases 94 References 102 !3 LIST OF TABLES ! !Table 1: Keyword Combinations for Literature Search 22 !Table 2: Example First Review Matrix 25 !Table 3: Example Second Review Matrix 25 !Table 4: Protocol Key 26 !Table 5: Example Third Review Matrix 29 Table 6: Imaging characteristics to differentiate cloacal exstrophy, bladder !exstrophy and cloacal malformation (Calvo-Garcia et al. -
ANC Level 1 2Nd Edition.Pdf
Pregnancy & Childbirth Management Guidelines Level- 1 A Guide for Nurses, Midwives and Doctors Second Edition DEPARTMENT OF WOMAN &CHILD HEALTH DIRECTORATE GENERAL OF PRIMARY HEALTH CARE MINISTRY OF HEALTH SULTANATE OF OMAN 2016 ML- 60 Pregnancy & Childbirth Management Guidelines Level- 1 A Guide for Nurses, Midwives and Doctors Second Edition 2016 I II ACKNOWLEDGEMENT Acknowledgement with gratitude to all contributors & Reviewers for their effort in updating this guideline manual: Contributors from Woman & Child Health Department: • Dr. Jamila Al-Abri, Senior Specialist, Dept. of Woman & Child Health • Dr. Fatima Al Hinai, Senior Specialist, Director of Woman & Child Health Dept. • Dr. Nawal Al Rashdi, Senior Specialist, Dept. of Woman & Child Health • Dr. Salwa Jabbar Alshahabi, Specialist, Dept. of Woman & Child Health • Dr. Omaima Abdel Wahab, Senior Medical Officer, Dept. of Woman & Child Health. Contributors from Primary Health Care Institutions: • Dr. Nabila Al Wahaibi, Senior Consultant (FAMCO), Wadi Kabeer Health Centre. • Dr. Ahdab Abdul Hafeez, Specialist, Muscat Health Centre. • Dr. Imrana Masoud, Senior Medical Officer, Al Seeb Health Centre. Contributors from National Diabetic & Endocrine Centre & NCD department • Dr. Noor Al Busaidi, Senior Consultant, Director of National Diabetic & Endocrine Centre (NDEC) • Dr. Hilal Al Musailhi, Senior Consultant Adult Endocrinology, (NDEC). • Dr. Deepa Manoharan , Medical Officer, (NDEC). • Dr. Nada Hareb Al Sumri, Senior Specialist, Non Communicable Disease Dept • Dr. Suleiman Al Shereigi, Senior Specialist in Public Health Administration,(NDEC) Reviewers from Secondary & Tertiary Heath Care : • Dr. Tamima Al Dughaishi, Senior Consultant Obstetrics & Gynecology, SQUH • Dr. Bernadette Punnoose, Senior Consultant Obstetrics & Gynecology, Royal Hospital • Dr. Badrya Al Fahdi, Senior Consultant Obstetrics & Gynecology, Royal Hospital • Dr. Sumaya Al Amri, Senior Specialist Obstetrics & Gynecology, Royal Hospital • Dr. -

Undergoing Prenatal Screening for Down's Syndrome
European Journal of Human Genetics (2007) 15, 563–569 & 2007 Nature Publishing Group All rights reserved 1018-4813/07 $30.00 www.nature.com/ejhg ARTICLE Undergoing prenatal screening for Down’s syndrome: presentation of choice and information in Europe and Asia Sue Hall1, Lyn Chitty2, Elizabeth Dormandy1, Amelia Hollywood1, Hajo IJ Wildschut3, Albert Fortuny4, Bianca Masturzo5,Ji´ı Sˇantavy´6, Madhulika Kabra7, Runmei Ma8 and Theresa M Marteau*,1 1King’s College London, Institute of Psychiatry, Department of Psychology (at Guy’s), Health Psychology Section, London, UK; 2Clinical & Molecular Genetics, Institute of Child Health and UCLH, London, UK; 3Department of Obstetrics and Gynecology, Erasmus University Medical Centre, Rotterdam, The Netherlands; 4Department of Obstetrics & Gynaecology, Prenatal diagnosis Unit, Hospital Clinic, University of Barcelona, Barcelona, Spain; 5Department of Obstetrics and Gynaecology, Prenatal Diagnosis Unit, Sant’Anna Hospital, Turin, Italy; 6Department of Medical Genetics & Fetal Medicine, University Hospital, Olomouc, Czech Republic; 7Genetics Subdivision, Department of Pediatrics, All India Institute of Medical Sciences, New Delhi, India; 8Department of Obstetrics and Gynaecology, 1st Affiliated Hospital of Kunming Medical College, Yunnan, China To date, studies assessing whether the information given to people about screening tests facilitates informed choices have focussed mainly on the UK, US and Australia. The extent to which written information given in other countries facilitates informed choices is not known. The aim of this study is to describe the presentation of choice and information about Down’s syndrome in written information about prenatal screening given to pregnant women in five European and two Asian countries. Leaflets were obtained from clinicians in UK, Netherlands, Spain, Italy, Czech Republic, China and India. -
Pathology and Pregnancy Congratulations As Everyone Will Tell You, Having a Baby Is One of Life’S Most Amazing and Enriching Experiences
Pathology and Pregnancy Congratulations As everyone will tell you, having a baby is one of life’s most amazing and enriching experiences. Whether this is your first pregnancy or you’ve done it all before, pathology tests will play a vital role in your care and progress. Every pregnancy is different. As your pregnancy progresses and your baby develops, you can expect to have some relevant tests. This booklet sets out the tests and gives you information about what they tell us. Some will be a matter of routine and others may be suggested if your doctor or midwife thinks they are necessary. Some will be done regularly every few weeks, others only at certain times when your baby is at a particular developmental milestone. It’s our job to perform your tests. You are most likely to meet us through our caring and friendly blood collectors. Behind them, back in the lab, are our pathologists and scientists, the medical experts who do the testing and interpret the results. They help your doctor make the important decisions. All of us at Sullivan Nicolaides Pathology are part of your healthcare team, and we are with you every step of the way. We wish you a happy pregnancy and a safe delivery 2 TESTS DURING PREGNANCY Not all tests are routine; some may only be performed if indicated. TIMING TESTS First Trimester MOTHER’S HEALTH Pregnancy test Full blood count including haemoglobin and platelet count Blood group and antibody testing Iron studies Blood glucose Vitamin D level Urine test for glucose and protein Pap smear INFECTIOUS DISEASES Rubella (German -

Prenatal Ultrasonography of Craniofacial Abnormalities
Prenatal ultrasonography of craniofacial abnormalities Annisa Shui Lam Mak, Kwok Yin Leung Department of Obstetrics and Gynaecology, Queen Elizabeth Hospital, Hong Kong SAR, China REVIEW ARTICLE https://doi.org/10.14366/usg.18031 pISSN: 2288-5919 • eISSN: 2288-5943 Ultrasonography 2019;38:13-24 Craniofacial abnormalities are common. It is important to examine the fetal face and skull during prenatal ultrasound examinations because abnormalities of these structures may indicate the presence of other, more subtle anomalies, syndromes, chromosomal abnormalities, or even rarer conditions, such as infections or metabolic disorders. The prenatal diagnosis of craniofacial abnormalities remains difficult, especially in the first trimester. A systematic approach to the fetal Received: May 29, 2018 skull and face can increase the detection rate. When an abnormality is found, it is important Revised: June 30, 2018 to perform a detailed scan to determine its severity and search for additional abnormalities. Accepted: July 3, 2018 Correspondence to: The use of 3-/4-dimensional ultrasound may be useful in the assessment of cleft palate and Kwok Yin Leung, MBBS, MD, FRCOG, craniosynostosis. Fetal magnetic resonance imaging can facilitate the evaluation of the palate, Cert HKCOG (MFM), Department of micrognathia, cranial sutures, brain, and other fetal structures. Invasive prenatal diagnostic Obstetrics and Gynaecology, Queen Elizabeth Hospital, Gascoigne Road, techniques are indicated to exclude chromosomal abnormalities. Molecular analysis for some Kowloon, Hong Kong SAR, China syndromes is feasible if the family history is suggestive. Tel. +852-3506 6398 Fax. +852-2384 5834 E-mail: [email protected] Keywords: Craniofacial; Prenatal; Ultrasound; Three-dimensional ultrasonography; Fetal structural abnormalities This is an Open Access article distributed under the Introduction terms of the Creative Commons Attribution Non- Commercial License (http://creativecommons.org/ licenses/by-nc/3.0/) which permits unrestricted non- Craniofacial abnormalities are common. -

BMFMS: Pregnancy Outcome NHS Education Board for Scotland Tendering a Project
Poster presentations (range 10–33 days, mean 19 days, p.0.05). The rate at which the were: Maternal Postnatal Attachment Questionnaire (MPAQ), side-lying group achieved three, four or five feeds per day Neonatal Perception Inventory (NPI), Parental Stress Index Short was, however, more rapid than the rate seen in the semi-upright Form (PSI-SF), Beck Anxiety Inventory (BAI), Beck Depression Arch Dis Child Fetal Neonatal Ed: first published as on 10 June 2008. Downloaded from group. Inventory (BDI) and Gordon-Personal Profile Inventory (GPP-I) Side-lying was well accepted by both parents and nursing staff. (time 1 only). This pilot study will inform the design of further necessary research Results: At time 1, some baseline characteristics between the to examine the potential benefits of this approach to an important intervention and the control group were significantly different with and common problem. regard to gestational age at birth (more preterm in the KMC group), days in intensive care (more days in the KMC group) and mothers’ BDI score (higher in the TC group). All of these were considered as PN.02 A DEVELOPMENT IN SCOTTISH QUALIFICATION AND CREDIT covariates in the statistical analysis. At time 2, KMC mothers were FRAMEWORK LEVEL 10 NEONATAL NURSING EDUCATION IN less rejective (MPAQ) towards their infants (F (1, 42) 9.56; SCOTLAND: INNOVATION AND COLLABORATION p = 0.004) and less preoccupied (NPI) in caring for their infants (F (1, 42) 5.06; p = 0.031) than TC mothers. The parenting stress level 1C Greig, 2SL Alexander, 1M Lobban. 1Napier University, Edinburgh, UK; 2Glasgow Caledonian University, Glasgow, UK changed between times 1 and 2: TC mothers only experienced a significant increase from time 1 (mean 42.77) to time 2 (49.27) (F (1, Two reports recommended a structured career pathway for 22) 7.570; p,0.01). -

Fetal Medicine August 2010
Advanced Training Skills Module – Fetal Medicine August 2010 Fetal Medicine This module is designed to prepare the future consultant for dealing with congenital abnormalities detected during pregnancy. This includes the organisation and supervision of screening programmes for structural and chromosomal anomalies. Many of these cases need to be managed within a multidisciplinary team which includes clinical geneticists and fetal medicine subspecialists. Apart from a sound knowledge of embryology and fetal physiology, clinicians working in this field must be competent in the prenatal diagnosis of common abnormalities. They also require a sound working knowledge of clinical and laboratory genetics in order that they can investigate and, where appropriate, refer suitable families. Competence in obstetric ultrasound is a prerequisite for advanced skills in prenatal diagnosis and fetal medicine. Trainees must complete the new Intermediate Ultrasound of Fetal Anatomy module prior to entry into the ATSM in Fetal Medicine. Attendance at a suitable Fetal Medicine theoretical course is a compulsory requirement of the module. This must be attended before completion of the ATSM and can have been done not more than three years previously. Specifically, once trained, individuals should: Work well as part of a multidisciplinary team Understand the organization of prenatal screening and diagnostic services at a local and regional level Be clinically competent in the prenatal diagnosis, counselling and management of common fetal abnormalities and markers of chromosomal abnormality. Be clinically competent and certified in first trimester screening for chromosomal abnormality by a combination of nuchal translucency assessment and biochemical marker assays. Be clinically competent at amniocentesis and have a sound knowledge of the principles and techniques of first trimester chorion villus biopsy. -
Prenatal Testing & Information
Prenatal Testing & Information ABOUT DOWN SYNDROME Helpful Resources Introduction Pregnancy can be an exciting time...and one that can produce Every woman and every pregnancy is different. Pediatricians, genetic emotions and many questions. Will my baby be a boy or a girl? Who counselors, family members, friends, spiritual advisers and others will he or she look like the most? Is my baby healthy? To help answer can assist a pregnant woman who received a prenatal diagnosis of Down syndrome. these questions, your doctor or healthcare provider may offer you a variety of testing options during your pregnancy. EARLY INTERVENTION, EDUCATIONAL AND EMOTIONAL SUPPORTS Woodbine House Books on Down Syndrome www.woodbinehouse.com/down-syndrome.29.0.0.2.htm MEDICAL CARE American Academy of Pediatrics, “Health Supervision for Children with Down Syndrome”: http://pediatrics.aappublications.org/ content/128/2/393.full.pdf Anna & John J. Sie Center for Down Syndrome, “Pediatric Guideline Record Tool”: http://www.globaldownsyndrome.org/pediatrics- record-sheet/ NEW & EXPECTANT PARENTS • www.downsyndrometest.org • www.ndsccenter.org/resources/new-and-expectant-parents • www.downsyndromepregnancy.org • Babies with Down Syndrome: A New Parents’ Guide (book is available in English and Spanish) • The Parent’s Guide to Down Syndrome: Advice, Information, Inspiration, and Support for Raising Your Child from Diagnosis through Adulthood IF YOU HAVE QUESTIONS ABOUT YOUR PREGNANCY OR ABOUT DOWN SYNDROME, PLEASE CALL 1-888-960-1670 OR VISIT US AT WWW.DOWNSYNDROMETEST.ORG 1 2 Answering What is a “prenatal test” for Down syndrome? Your Questions GENERALLY THERE ARE TWO types of tests (screening Should I have testing? tests and diagnostic tests) that you can have while you are pregnant to help determine if your baby has Down syndrome or another THE DECISION WHETHER TO HAVE a prenatal chromosome condition. -

The Identification and Validation of Neural Tube Defects in the General Practice Research Database
THE IDENTIFICATION AND VALIDATION OF NEURAL TUBE DEFECTS IN THE GENERAL PRACTICE RESEARCH DATABASE Scott T. Devine A dissertation submitted to the faculty of the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the School of Public Health (Epidemiology). Chapel Hill 2007 Approved by Advisor: Suzanne West Reader: Elizabeth Andrews Reader: Patricia Tennis Reader: John Thorp Reader: Andrew Olshan © 2007 Scott T Devine ALL RIGHTS RESERVED - ii- ABSTRACT Scott T. Devine The Identification And Validation Of Neural Tube Defects In The General Practice Research Database (Under the direction of Dr. Suzanne West) Background: Our objectives were to develop an algorithm for the identification of pregnancies in the General Practice Research Database (GPRD) that could be used to study birth outcomes and pregnancy and to determine if the GPRD could be used to identify cases of neural tube defects (NTDs). Methods: We constructed a pregnancy identification algorithm to identify pregnancies in 15 to 45 year old women between January 1, 1987 and September 14, 2004. The algorithm was evaluated for accuracy through a series of alternate analyses and reviews of electronic records. We then created electronic case definitions of anencephaly, encephalocele, meningocele and spina bifida and used them to identify potential NTD cases. We validated cases by querying general practitioners (GPs) via questionnaire. Results: We analyzed 98,922,326 records from 980,474 individuals and identified 255,400 women who had a total of 374,878 pregnancies. There were 271,613 full-term live births, 2,106 pre- or post-term births, 1,191 multi-fetus deliveries, 55,614 spontaneous abortions or miscarriages, 43,264 elective terminations, 7 stillbirths in combination with a live birth, and 1,083 stillbirths or fetal deaths. -

Pretest Obstetrics and Gynecology
Obstetrics and Gynecology PreTestTM Self-Assessment and Review Notice Medicine is an ever-changing science. As new research and clinical experience broaden our knowledge, changes in treatment and drug therapy are required. The authors and the publisher of this work have checked with sources believed to be reliable in their efforts to provide information that is complete and generally in accord with the standards accepted at the time of publication. However, in view of the possibility of human error or changes in medical sciences, neither the authors nor the publisher nor any other party who has been involved in the preparation or publication of this work warrants that the information contained herein is in every respect accurate or complete, and they disclaim all responsibility for any errors or omissions or for the results obtained from use of the information contained in this work. Readers are encouraged to confirm the information contained herein with other sources. For example and in particular, readers are advised to check the prod- uct information sheet included in the package of each drug they plan to administer to be certain that the information contained in this work is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. This recommendation is of particular importance in connection with new or infrequently used drugs. Obstetrics and Gynecology PreTestTM Self-Assessment and Review Twelfth Edition Karen M. Schneider, MD Associate Professor Department of Obstetrics, Gynecology, and Reproductive Sciences University of Texas Houston Medical School Houston, Texas Stephen K. Patrick, MD Residency Program Director Obstetrics and Gynecology The Methodist Health System Dallas Dallas, Texas New York Chicago San Francisco Lisbon London Madrid Mexico City Milan New Delhi San Juan Seoul Singapore Sydney Toronto Copyright © 2009 by The McGraw-Hill Companies, Inc.