Traditional Male Circumcision Among Young People
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
North America Other Continents
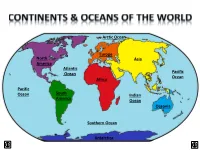
Arctic Ocean Europe North Asia America Atlantic Ocean Pacific Ocean Africa Pacific Ocean South Indian America Ocean Oceania Southern Ocean Antarctica LAND & WATER • The surface of the Earth is covered by approximately 71% water and 29% land. • It contains 7 continents and 5 oceans. Land Water EARTH’S HEMISPHERES • The planet Earth can be divided into four different sections or hemispheres. The Equator is an imaginary horizontal line (latitude) that divides the earth into the Northern and Southern hemispheres, while the Prime Meridian is the imaginary vertical line (longitude) that divides the earth into the Eastern and Western hemispheres. • North America, Earth’s 3rd largest continent, includes 23 countries. It contains Bermuda, Canada, Mexico, the United States of America, all Caribbean and Central America countries, as well as Greenland, which is the world’s largest island. North West East LOCATION South • The continent of North America is located in both the Northern and Western hemispheres. It is surrounded by the Arctic Ocean in the north, by the Atlantic Ocean in the east, and by the Pacific Ocean in the west. • It measures 24,256,000 sq. km and takes up a little more than 16% of the land on Earth. North America 16% Other Continents 84% • North America has an approximate population of almost 529 million people, which is about 8% of the World’s total population. 92% 8% North America Other Continents • The Atlantic Ocean is the second largest of Earth’s Oceans. It covers about 15% of the Earth’s total surface area and approximately 21% of its water surface area. -
From Operation Serval to Barkhane
same year, Hollande sent French troops to From Operation Serval the Central African Republic (CAR) to curb ethno-religious warfare. During a visit to to Barkhane three African nations in the summer of 2014, the French president announced Understanding France’s Operation Barkhane, a reorganization of Increased Involvement in troops in the region into a counter-terrorism Africa in the Context of force of 3,000 soldiers. In light of this, what is one to make Françafrique and Post- of Hollande’s promise to break with colonialism tradition concerning France’s African policy? To what extent has he actively Carmen Cuesta Roca pursued the fulfillment of this promise, and does continued French involvement in Africa constitute success or failure in this rançois Hollande did not enter office regard? France has a complex relationship amid expectations that he would with Africa, and these ties cannot be easily become a foreign policy president. F cut. This paper does not seek to provide a His 2012 presidential campaign carefully critique of President Hollande’s policy focused on domestic issues. Much like toward France’s former African colonies. Nicolas Sarkozy and many of his Rather, it uses the current president’s predecessors, Hollande had declared, “I will decisions and behavior to explain why break away from Françafrique by proposing a France will not be able to distance itself relationship based on equality, trust, and 1 from its former colonies anytime soon. solidarity.” After his election on May 6, It is first necessary to outline a brief 2012, Hollande took steps to fulfill this history of France’s involvement in Africa, promise. -

Africa 1952-1953
SUMMARY OF RECENT ECONOMIC DEVELOPMENTS IN AFRICA 1952-53 Supplement to World Economic Report UNITED NATIONS UMMARY OF C T ECONOMIC EVE OPME TS IN AF ICA 1952-53 Supplement World Economic Report UNITED NATIONS DEPARTMENT OF ECONOMIC AFFAIRS New York, 1954 E/2582 ST/ECA/26 May 1954 UNITED NATIONS PUBLICATION Sal es No.: 1951\..11. C. 3 Price: $U.S. $0.80; 6/- stg.; Sw.fr. 3.00 (or equivalent in other currencies) FOREWDRD This report is issued as a supplement to the World Economic Report, 1952-53, and has been prepared in response to resolution 367 B (XIII) of the Economic and Social Council. It presents a brief analysis of economic trends in Africa, not including Egypt but including the outlying islands in the Indian and Atlantic Oceans, on the basis of currently available statistics of trade, production and development plans covering mainly the year 1952 and the first half of 1953, Thus it carries forward the periodic surveys presented in previous years in accordance with resolution 266 (X) and 367 B (XIII), the most recent being lIRecent trends in trade, production and economic development plansll appearing as part II of lIAspects of Economic Development in Africall issued in April 1953 as a supplement to the World Economic Report, 1951-52, The present report, like the previous ones, was prepared in the Division of Economic Stability and Development of the United Nations Department of Economic Affairs. EXPLANATION OF SYMBOLS The following symbols have been used in the tables throughout the report: Three dots ( ... ) indicate that data -

Countering Terrorism in East Africa: the U.S
Countering Terrorism in East Africa: The U.S. Response Lauren Ploch Analyst in African Affairs November 3, 2010 Congressional Research Service 7-5700 www.crs.gov R41473 CRS Report for Congress Prepared for Members and Committees of Congress Countering Terrorism in East Africa: The U.S. Response Summary The United States government has implemented a range of programs to counter violent extremist threats in East Africa in response to Al Qaeda’s bombing of the U.S. embassies in Tanzania and Kenya in 1998 and subsequent transnational terrorist activity in the region. These programs include regional and bilateral efforts, both military and civilian. The programs seek to build regional intelligence, military, law enforcement, and judicial capacities; strengthen aviation, port, and border security; stem the flow of terrorist financing; and counter the spread of extremist ideologies. Current U.S.-led regional counterterrorism efforts include the State Department’s East Africa Regional Strategic Initiative (EARSI) and the U.S. military’s Combined Joint Task Force – Horn of Africa (CJTF-HOA), part of U.S. Africa Command (AFRICOM). The United States has also provided significant assistance in support of the African Union’s (AU) peace operations in Somalia, where the country’s nascent security forces and AU peacekeepers face a complex insurgency waged by, among others, Al Shabaab, a local group linked to Al Qaeda that often resorts to terrorist tactics. The State Department reports that both Al Qaeda and Al Shabaab pose serious terrorist threats to the United States and U.S. interests in the region. Evidence of linkages between Al Shabaab and Al Qaeda in the Arabian Peninsula, across the Gulf of Aden in Yemen, highlight another regional dimension of the threat posed by violent extremists in the area. -

Female Genital Cutting
DHS Comparative Reports 7 Female Genital Cutting in the Demographic and Health Surveys: A Critical and Comparative Analysis MEASURE DHS+ assists countries worldwide in the collection and use of data to monitor and evaluate population, health, and nutrition programs. Funded by the U.S. Agency for International Development (USAID), MEASURE DHS+ is implemented by ORC Macro in Calverton, Maryland. The main objectives of the MEASURE DHS+ project are: 1) to provide decisionmakers in survey countries with information useful for informed policy choices, 2) to expand the international population and health database, 3) to advance survey methodology, and 4) to develop in participating countries the skills and resources necessary to conduct high-quality demographic and health surveys. Information about the MEASURE DHS+ project or the status of MEASURE DHS+ surveys is available on the Internet at http://www.measuredhs.com or by contacting: ORC Macro 11785 Beltsville Drive, Suite 300 Calverton, MD 20705 USA Telephone: 301-572-0200 Fax: 301-572-0999 E-mail: [email protected] DHS Comparative Reports No. 7 Female Genital Cutting in the Demographic and Health Surveys: A Critical and Comparative Analysis P. Stanley Yoder Noureddine Abderrahim Arlinda Zhuzhuni ORC Macro Calverton, Maryland, USA September 2004 This publication was made possible through support provided by the U.S. Agency for International Development under the terms of Contract No. HRN-C-00-97-00019- 00. The opinions expressed herein are those of the authors and do not necessarily reflect the views of the U.S. Agency for International Development. Editor: Sidney Moore Series design: Katherine Senzee Document production: Justine Faulkenburg Recommended citation: Yoder, P. -

The North Caucasus: the Challenges of Integration (III), Governance, Elections, Rule of Law
The North Caucasus: The Challenges of Integration (III), Governance, Elections, Rule of Law Europe Report N°226 | 6 September 2013 International Crisis Group Headquarters Avenue Louise 149 1050 Brussels, Belgium Tel: +32 2 502 90 38 Fax: +32 2 502 50 38 [email protected] Table of Contents Executive Summary ................................................................................................................... i Recommendations..................................................................................................................... iii I. Introduction ..................................................................................................................... 1 II. Russia between Decentralisation and the “Vertical of Power” ....................................... 3 A. Federative Relations Today ....................................................................................... 4 B. Local Government ...................................................................................................... 6 C. Funding and budgets ................................................................................................. 6 III. Elections ........................................................................................................................... 9 A. State Duma Elections 2011 ........................................................................................ 9 B. Presidential Elections 2012 ...................................................................................... -

The Association Between Female Genital Mutilation (FGM) and the Risk of HIV/AIDS in Kenyan Girls and Women (15-49 Years)
Georgia State University ScholarWorks @ Georgia State University Public Health Theses School of Public Health Spring 5-4-2010 The Association between Female Genital Mutilation (FGM) and the Risk of HIV/AIDS in Kenyan Girls and Women (15-49 Years) Rosemary G. Kinuthia Georgia State University Follow this and additional works at: https://scholarworks.gsu.edu/iph_theses Part of the Public Health Commons Recommended Citation Kinuthia, Rosemary G., "The Association between Female Genital Mutilation (FGM) and the Risk of HIV/ AIDS in Kenyan Girls and Women (15-49 Years)." Thesis, Georgia State University, 2010. https://scholarworks.gsu.edu/iph_theses/98 This Thesis is brought to you for free and open access by the School of Public Health at ScholarWorks @ Georgia State University. It has been accepted for inclusion in Public Health Theses by an authorized administrator of ScholarWorks @ Georgia State University. For more information, please contact [email protected]. Abstract Rosemary Kinuthia The Association between Female Genital Mutilation (FGM) and the Risk of HIV/AIDS in Kenyan Girls and Women (15-49 Years) (Under the direction of Dr. Ike S. Okosun, MS, MPH, PhD, FRSPH and Dr. Richard Rothenberg, MD, MPH, FACP). INTRODUCTION: Kenya like the rest of Sub-Saharan Africa continues to be plagued with high rates of AIDS/HIV. Research has shown that cultural practices have serious implications for the spread of HIV/AIDS, as well as other communicable diseases. One of the practices that have been speculated to have an impact on AIDS/HIV is female genital mutilation (FGM). Despite efforts to eradicate the practice, prevalence of FGM in Kenya remains relatively high. -

Country by Country Reporting
COUNTRY BY COUNTRY REPORTING PUBLICATION REPORT 2018 (REVISED) Anglo American is a leading global mining company We take a responsible approach to the management of taxes, As we strive to deliver attractive and sustainable returns to our with a world class portfolio of mining and processing supporting active and constructive engagement with our stakeholders shareholders, we are acutely aware of the potential value creation we operations and undeveloped resources. We provide to deliver long-term sustainable value. Our approach to tax is based can offer to our diverse range of stakeholders. Through our business on three key pillars: responsibility, compliance and transparency. activities – employing people, paying taxes to, and collecting taxes the metals and minerals to meet the growing consumer We are proud of our open and transparent approach to tax reporting. on behalf of, governments, and procuring from host communities – driven demands of the world’s developed and maturing In addition to our mandatory disclosure obligations, we are committed we make a significant and positive contribution to the jurisdictions in economies. And we do so in a way that not only to furthering our involvement in voluntary compliance initiatives, such which we operate. Beyond our direct mining activities, we create and generates sustainable returns for our shareholders, as the Tax Transparency Code (developed by the Board of Taxation in sustain jobs, build infrastructure, support education and help improve but also strives to make a real and lasting positive Australia), the Responsible Tax Principles (developed by the B Team), healthcare for employees and local communities. By re-imagining contribution to society. -
Chirac and ‘La Franc¸Afrique’: No Longer a Family Affair Tony Chafer
Modern & Contemporary France Vol. 13, No. 1, February 2005, pp. 7–23 Chirac and ‘la Franc¸afrique’: No Longer a Family Affair Tony Chafer Since political independence, France has maintained a privileged sphere of influence—the so-called ‘pre´ carre´’—in sub-Saharan Africa, based on a series of family-like ties with its former colonies. The cold war provided a favourable environment for the development of this special relationship, as the USA saw the French presence in this part of the world as useful for the containment of Communism. However, following the end of the cold war, France has had to adapt to a new international policy environment that is more competitive and less conducive to the maintenance of such family-like ties. This article charts the evolution of Franco-African relations in an era of globalisation, as French governments have undertaken a hesitant process of policy adaptation since the mid-1990s. Unlike decolonisation in Indochina and Algeria, the transfer of power in Black Africa was largely peaceful; as a result, there was no rupture of relations with the former colonial power. On the contrary, the years after independence were marked by an intensification of the links with France. Official rhetoric often referred to the great Franco-African family and the term ‘la Franc¸afrique’ testified to a symbiotic relationship in which ‘Africa is experienced in French representations as a natural extension where the Francophone world and Francophilia merge’ (Bourmaud, 2000). In fact, a wide variety of terms have been coined to describe -

AFRICA Version Posted at on 17 June 2019 - Ii
Human Papillomavirus and Related Diseases Report AFRICA Version posted at www.hpvcentre.net on 17 June 2019 - ii - Copyright and Permissions ©ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre), 2019. All rights reserved. HPV Information Centre publications can be obtained from the HPV Informa- tion Centre Secretariat, Institut Català d’Oncologia, Avda. Gran Via de l’Hospitalet, 199-203 08908 L’Hospitalet del Llobregat (Barcelona) Spain. E-mail: [email protected]. Requests for per- mission to reproduce or translate HPV Information Centre publications - whether for sale or for non- commercial distribution- should be addressed to the HPV Information Centre Secretariat, at the above address. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part the HPV Information Centre concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers products does not imply that they are endorsed or recommended the HPV Information Centre in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. All reasonable precautions have been taken by the HPV Information Centre to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. -

Male Circumcision: Global Trends and Determinants of Prevalence, Safety and Acceptability IWHO Library Cataloguing-In-Publication Data
Male circumcision Global trends and determinants of prevalence, safety and acceptability UNAIDS Department of Reproductive health and Research 20 AVENUE APPIA World Health Organization CH-1211 GENEVA 27 20 AVENUE APPIA SWITZERLAND CH-1211 GENEVA 27 SWITZERLAND T (+41) 22 791 36 66 F (+41) 22 791 41 87 T (+41) 22 791 2111 F (+41) 22 791 41 71 www.unaids.org ISBN 978 92 4 159616 9 www.who.int/reproductive-health Male circumcision: global trends and determinants of prevalence, safety and acceptability IWHO Library Cataloguing-in-Publication Data Male circumcision: global trends and determinants of prevalence, safety and acceptability. « UNAIDS / 07.29E / JC1320E ». 1. Circumcision, Male - trends. 2.Circumcision, Male - methods. 3.HIV infections - prevention and control. I.World Health Organization. II.UNAIDS. ISBN 978 92 4 159616 9 (WHO) (NLM classification: WJ 790) ISBN 978 92 9 173633 1 (UNAIDS) © World Health Organization and Joint United Nations Programme on HIV/AIDS, 2007 All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatso- ever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. -

East Africa: the Next Hub for Apparel Sourcing?
AUGUST 2015 Retail and Consumer Packaged Goods East Africa: The next hub for apparel sourcing? East African countries—in particular, Ethiopia and Kenya—have the potential to become bigger players in garment manufacturing. But the road ahead won’t be easy. Achim Berg, Saskia Hedrich, and Bill Russo In the past two years, a number of European indeed fallen since 2010—but China remains companies—among them, H&M, Primark, and the undisputed giant of garment manufacturing, Tesco—began sourcing some of their garments with approximately $177 billion in apparel from Ethiopia. The rest of the apparel industry took exports in 2013. notice: since 2013, there has been rising interest in not just Ethiopia but also other East African Among CPOs surveyed, Bangladesh remains at the countries as potential sourcing destinations top of the list of future sourcing destinations, with for apparel. Also contributing to the buzz is the 48 percent of respondents including the country renewal of the African Growth and Opportunity in their top three (Exhibit 1). And 62 percent said Act (AGOA), which gives certain countries in sub- they intend to increase their sourcing value from Saharan Africa duty-free access to the US market. Bangladesh over the next five years. The next two up-and-coming countries are Vietnam and India, What is the true potential of East Africa to grow where, respectively, 59 percent and 54 percent of into a major garment-sourcing hub? To find out, surveyed CPOs plan to increase their sourcing value we visited factories in the region; interviewed in the next five years.