St Pancras International 23 September 2009
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Improved Spiral Geometry for High Speed Rail
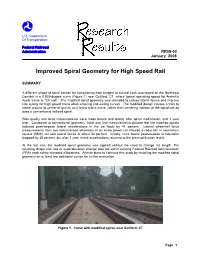
U.S. Department Of Transportation Federal Railroad Administration RR08-02 January 2008 Improved Spiral Geometry for High Speed Rail SUMMARY A different shape of spiral section for transitioning from tangent to curved track was tested on the Northeast Corridor in a 0.925-degree curve (Figure 1) near Guilford, CT, where typical operating speed for Amtrak's Acela trains is 125 mph. The modified spiral geometry was intended to reduce lateral forces and improve ride quality for high speed trains when entering and exiting curves. The modified design causes a train to rotate around its center of gravity as it leans into a curve, rather than centering rotation at the top-of-rail as does a conventional railroad spiral. Ride quality and force measurements were made before and shortly after spiral modification, and 1 year later. Compared to conventional geometry, initial and final measurements showed that the modified spirals reduced peak-to-peak lateral accelerations in the car body by 41 percent. Lateral wheel-rail force measurements from two instrumented wheelsets of an Acela power car showed a reduction in root-mean- square (RMS) net axle lateral forces of about 33 percent. Initially, truck lateral peak-to-peak acceleration dropped by 38 percent, but after 1 year, these accelerations returned to the pre-modification levels. At the test site, the modified spiral geometry was applied without the need to change rail length. The resulting shape and rate of superelevation change also fall within existing Federal Railroad Administration (FRA) track safety standard allowances. Amtrak plans to continue this study by installing the modified spiral geometry on at least two additional curves for further evaluation. -

3 Power Supply
3 Power supply Table of contents Article 44 Installation, etc. of Contact Lines, etc. .........................................................................2 Article 45 Approach or Crossing of Overhead Contact Lines, etc................................................ 10 Article 46 Insulation Division of Contact Lines............................................................................ 12 Article 47 Prevention of Problems under Overbridges, etc........................................................... 13 Article 48 Installation of Return Current Rails ........................................................................... 13 Article 49 Lightning protection..................................................................................................... 13 Article 51 Facilities at substations................................................................................................. 14 Article 52 Installation of electrical equipment and switchboards ................................................. 15 Article 53 Protection of electrical equipment................................................................................ 16 Article 54 Insulation of electric lines ............................................................................................ 16 Article 55 Grounding of Electrical Equipment ............................................................................. 18 Article 99 Inspection and monitoring of the contact lines on the main line.................................. 19 Article 101 Records........................................................................................................................ -

M-7 Long Island Railroad .Montreal EMU .Gallery Car Electric Multiple Unit -M- ~ New York, Usj
APPENDIX 6 . M-7 Long Island Railroad .Montreal EMU .Gallery Car Electric Multiple Unit -M- ~ New York, Usj Under joint agreement to the Metropolitan Transportation Authority / Long Island Rail Road (LIRR) and the Metro-North Railroad (MNR), Bombardier Transportation is providing Electric Multiple Unit (EMU) M- 7 commuter cars to LIRR to begin replacement of its Metropolitan M-I commuter car fleet. Chartered in 1834, the Long The units are equipped with The interior of the LIRR' Island Rail Road is the largest Bombardier's renowned stainless "Car of the Future" was designel Commuter Rail system in North steel carbodies for long life and with the input of the passenger America. low maintenance, and asynchro- and employees and includes a] nous AC motors featuring state- ADA compliant toilet, cellula Bombardier's new Electric of-the-art IGBT {isolated gate bipo- telephone and wide, single-lea Multiple Units, its first railcar lar transistors) inverters. Use of sliding doors for ease of entry an contract for the LIRR, will service outboard-bearing bolsterless fab- exit. the Long Island commuter lines, ricated bogies offers considerable constituting 80% of the system. weight savings over cast bogies. ~ BOMBARDIER BOMBARD" TRANSPORTATION 'V Electric Multiple Unit -M- 7 POWERCAR WITH TOILET ---10' 6' B END FEND I 3,200 mi , -: -" 0 C==- ~=0 :- CJCJ ~~[] CJCJCJCJCJCJ [] I D b 01 " ~) -1::1 1211-1/2 t~J ~~W ~~IL...I ~w -A'-'1~~~- I ~~ 309~mmt ~ 1 I~ 11 m 2205~16~m-! 591..1.6" mm --I I 1- -- 59°6" ° 4°8-1/2. , ~ 16,~:,60~m ~-- -;cl 10435mm ~ .-1 -

Turboliner Modernization Project Delays
ALAN G. HEVESI 110 STATE STREET COMPTROLLER ALBANY, NEW YORK 12236 STATE OF NEW YORK OFFICE OF THE STATE COMPTROLLER June 12, 2003 Mr. Joseph H. Boardman Commissioner Department of Transportation State Office Building Campus – Building #5 Albany, NY 12232 Re: Turboliner Modernization Project Project Delays Report 2002-S-52 Dear Mr. Boardman: Pursuant to the State Comptroller’s authority as set forth in Article V, Section 1 of the State Constitution, and Article II, Section 8 of the State Finance Law, we have audited the progress made by the Department of Transportation on the Turboliner Modernization Project (Project) for the period October 1, 1998 through October 31, 2002. This report is the first in a series of reports we plan to issue addressing activities related to the Project. Other reports will address such topics as Project monitoring and controls over contract payments. A. Background The Department of Transportation (Department) oversees the transportation systems in New York State. In one of these systems, rail transportation between New York City and Buffalo (the Empire Corridor) is provided to passengers by the National Railroad Passenger Corporation, also known as Amtrak. To improve passenger rail transportation in the Empire Corridor, the Department is implementing the High Speed Rail Improvement Program. The Department and Amtrak have entered into a contract to support the objectives of the high-speed rail program. While this program was formally announced to the public in September 1998, some of the activities relevant to the program were initiated prior to the announcement. One of these activities was the Project, in which seven existing Amtrak trainsets were to be remanufactured so that they would be capable of traveling at 125 miles per hour, and meet current Federal safety and accessibility standards. -

Design Data on Suspension Systems of Selected Rail Passenger Cars RR 5931R 5021
Design Data on Suspension U.S. Department Systems of Selected Rail of Transportation Federal Railroad Passenger Cars Administration Office of Research and Development Washington, DC 20590 ~ail Vehicles & lonents NOTICE This document is disseminated under the sponsorship of the Department of Transportation in the interest of information exchange. The United States Government assumes no liability for its contents or use thereof. NOTICE The United States Government does not endorse products or manufacturers. Trade or manufacturers' names appear herein solely because they are considered essential to the objective of this report. Form Approved REPORT DOCUMENTATION PAGE OMS No. 0704-0188 " Public reporting bulden for this collection of infonnation is estimated to average 1 hourper response. including the time for naviewing instructions. sean:hin9 existing data sources. gathering and maintaining the data needed. and completing and naviewing the collection of information. send comments regarding this bulden estimate or any other aspect of this collection of information. including suggestions for reducing this bulden. to WashingICn Headquarters services Dinactorata for Information Operations and Reports, 1215 Jefferson Davis Highway. SUite 1204, Arlington. VA 22202-4302. and to the Office of Management and Budget, Paperworlc Reduction Project (07~188). Washington. DC 20503. 1. AGENCY USE ONLY (Leave blank) 2. REPORT DATE 3. REPORT TYPE AND OATES COVE~EO July 1996 Final Report ~ober1993-December1994 4. TITLE AND SUBnTLE S. FUNDING NUMBERS Design Data on Suspension Systems of Selected Rail Passenger Cars RR 5931R 5021 6. AUTHORS Alan J. Bing. Shaun R. Berry and Hal B. Henderson 7. PERFORMING ORGANIZAnON NAME(S) AND ADDRESS(ES) 8. PERFORMING ORGANlZAnON Arthur D. -

Catenary 전기적 특성 Electrical Characteristics of Catenary
Catenary 전기적 특성 Electrical Characteristics of Catenary 데버랜전고팔* 노영환** 김윤호*** Devarajan Gopal Lho, Young Hwan Kim, Yoon Ho ------------------------------------------------------------------------------------ ABSTRACT In this paper, the basic requirements of catenary in railroad traction is explained. Three different types of catenary suspension systems for different terrains, environments and high speed / low speed trains are presented. The essential requirements of catenary such as reliability, cost effectiveness, maintenance and ruggedness requirements are discussed. The catenary materials and safety problems associated in it are dealt. ------------------------------------------------------------------------------------ 1. Introduction: There is a wide variety of electric traction systems around the world, which have been built according to the type of railway, its location and the technology available at the time of the installation. Many installations seen today were first built up to 100 years ago, some when electric traction was barely out its diapers, so to speak, and this has had a great influence on what is seen today. In the last 20 years there has been a gigantic acceleration in railway traction development. This has run in parallel with the development of power electronics and microprocessors/ microcomputers. What have been the accepted norms for the industry for, sometimes, 80 years, have suddenly been thrown out and replaced by fundamental changes in design, manufacture and operation. Many of these developments are highly technical and complex. To begin with, the electric railway needs a power supply that the trains can access at all times. It must be safe, economical and user friendly. It can use either DC (direct current) or AC (alternating current), the former being, for many years, simpler for railway traction purposes, the latter being better over long distances and cheaper to install but, until recently, more complicated to control at train level. -

Velaro. Top Performance for High Speed. Top Performance for High Speed
siemens.com/mobility Velaro. Top performance for high speed. Top performance for high speed More people. More goods. Fewer resources. There’s no end to the number of challenges facing rail operators today. And pro- viding fast, reliable connections between urban centers across borders calls for a future-ready alternative to the airplane and the automobile. So why not get on board a mature high-perfor- mance connection. One that is setting new standards daily and at high speed: Welcome to Velaro. 2 Expertise ten years ahead of its time day-to-day international service. You can versatile: Completely different variants can High speed – a key factor to economic check out the successes for yourself by be configured from one standard platform. success and quality of life across entire riding on a Velaro in Spain, Russia, or China. It can be customized in terms of capacity, regions. But Velaro‘s more than ten-year Its technology, flexibility, comfort, and comfort, and service. The platform is so technological edge did not come over- cost-effectiveness are sure to impress you. mature that a Velaro can be rapidly inte - night. The revolutionary move away from grated into your operations – today and all-traction equipment concentrated in a Variety with a family connection in the future. A perfect base for increas- power car operating in push-pull mode to Be it a high-class solution for discrimi- ing your market share and an attractive a distributed traction arrangement was nating travelers, a trainset with outstand- concept – confirmed by Eurostar Interna- made by Siemens in the 1990s. -

Head on Generation (HOG) - a Step Towards Energy Efficiency O.P
Head on Generation (HOG) - A step towards energy efficiency O.P. Kesari, EDSE/Co-Ord./RDSO S.K. Deo, SSE/RDSO Abstract Indian Railways imported 22 WAG9 locomotives and 11 WAP5 locomotives from M/s. ABB, Switzerland in 1996-97. Later on Chittaranjan Loco Works (CLW) started the production of WAP-7 locomotive. The WAP-7 is actually a modified version of the WAG 9 freight locomotive with modified gear ratios. A hotel load winding in locomotive transformer of WAP5 and WAP7 locomotives has been provided to cater the hotel load supply to the coaches through hotel load converter. Different power generation schemes are being used on IR to cater hotel load requirements of the mail/express trains. The most common schemes being used presently are Self Generation (SG), where the train has few air conditioned coaches and End on Generation (EOG), where the train has all air conditioned coaches such as Rajdhani, Shatabdi and Duronto trains.Railway Board had issued instructions vide letter No 95/elec(G)/114/13 Pt dtd. 25/10/07 for implementation of HOG scheme by manufacturing of 3 phase electric loco with IGBT technology having minimum 2x500 KVA hotel load converters on loco and one under-slung DA set in SLR for Rajdhani/Shatabdi trains. This paper discusses the challenges faced in the regular operations of the converters fitted in the WAP-7 locomotive with the Shatabdi LHB coaches. This paper also discusses the benefits of the HOG and suggests future course of action. 1. Preamble Indian Railway is manufacturing 3-phase electric locomotives at Chittaranjan locomotive works (CLW) i.e. -

Hot Oot Iron Horse
Hot oot iron horse Downloaded from http://asmedigitalcollection.asme.org/memagazineselect/article-pdf/122/06/46/6382724/me-2000-jun1.pdf by guest on 03 October 2021 Attempts are under way to bring U.S. rail service into the 21 st century. By Henry Baumgartner, Contributing Editor HE ERA OF H IGH-S PEED rail transportation may be and its cousins in Europe, which can have speeds on the decades old in Japan and E urope, but only this order of 200 mph, but w hich require dedica ted ultra T year, with the imminent debut of Amtrak's Acela straight track to be laid expressly for the trains of great Express service, is this innovation due to arrive in the speed. Clearly, there is some catching up yet to be done. United States, or at least the Northeas t Corridor. Even A range of initiatives that may spark further advances in then, the fas test trains, which will go about 150 mph, the U.S. rail system are under way in the United States w ill be no match for the TGV (train Cl gra l1de vitesse) and abroad. Amtrak's new Acela Express is scheduled to go into service this summer in the Northeast Corridor. It is expected to achieve a speed of 150 mph . 46 JUN E 2000 MECHANICAL ENGINEER I NG The lines of development being pursued in the railroad industry fall under two main headings: high-speed ra il, based on tradi tional "steel-on-steel" technologies, and maglev, which is short for magnetic levita tion. -
Recommended Practice for Head End Power Source Characteristics
APTA PR-E-RP-015-99 Edited 3-22-04 14. APTA PR-E-RP-015-99 Recommended Practice for Head End Power Source Characteristics Approved October 28, 1999 APTA PRESS Task Force Authorized January 11, 2000 APTA Commuter Rail Executive Committee Abstract: This recommended practice defines the characteristics necessary on new equipment for head end power (HEP) sources, including diesel-driven alternators, inverters and utility- supplied wayside power. The HEP source is comprised of power source, switchgear, control system (incorporating trainline complete functions) and connections to vehicle HEP trainline(s). Keywords: head end power source, trainline, 480 VAC Copyright © 1999 by The American Public Transportation Association 1666 K Street, N. W. Washington, DC, 20006, USA No part of this publication may be reproduced in any form, in an electronic retrieval system or otherwise, without the prior written permission of The American Public Transportation Association. 14.0 Volume III – Electrical APTA PR-E-RP-015-99 Edited 3-22-04 Participants The American Public Transportation Association greatly appreciates the contributions of the following individual(s), who provided the primary effort in the drafting of the Recommended Practice for Head End Power Source Characteristics. Dick Bruss At the time that this recommended practice was completed, the PRESS Electrical Committee included the following members: Doug Warner, Chair Gilbert L. Bailey Stephen Hilbert Brad Barkman LeRoy D. Jones Ronald Bartels Brian Ley Richard Benjamin Otto Masek Dick Bruss Rich Mazur Daniel L. Davis Chuck Olson James Dietz David Phelps Dave Elliott Craig Prudian Hassan A. Fazli George Scerbo Bert Gagne Ike Tingos Peter Hale Steve Zuiderveen Carl C. -

The Street Railway Journal
7. Vol VIII. MEW YORK fy CHICAGO, JURY. No. The Yonkers (N. Y.) Eleetrie Railway. On the portion of the route equipped with electric apparatus the same rails are in use as when the line was The increase in the earning capacity of a street rail- operated by horses. The construction consists of centre way caused by a change from horse to electric power is bearing tram rails of about thirty-five pounds weight, often considerable, and sometimes changes an annual de- spiked directly to the stringers and held to gauge by tie ficit in the balance sheet to the showingof an annual surplus rods placed at intervals. The return circuit is made of earnings over expenses. An instance of how a line in the by bonding the rails, and also by the use of the Sabold hands of a receiver, and with operating expenses greater return system, previously described in these pages. This than receipts, can be transformed by the adoption consists in driving between the rails at intervals of sixty of electric power into a profitable enterprise is shown in feet a galvanized iron rod, seven feet long, and electrically the case of the Yonkers street railway. The road was connecting these rods to the rail bonds on each side. Al- FIG I.—STREET SCEN E—YON KERS ELECTRIC RAILWAY. purchased from the bondholders about four months ago though there is a deep layer of broken stone under a con- by a syndicate who believed in the economy of electric siderable portion of the track, this method of return compared with animal power for street car propulsion, seems to give good satisfaction, and no trouble has been and at present electric motors are running on two of the experienced with the telephone service, although the lat- three divisions, and the entire line is being equipped as ter also uses a grounded return. -

Moving America March 1991 New Directions, New Opportunities
U. S. Department of T ransportation Federal Railroad Administration Moving America March 1991 New Directions, New Opportunities 11 - Advanced Systems Foreword New intercity high speed rail technologies may become a reality in the United States in the next few years. As a result of the development of these advanced guided ground transportation systems there is a need to reexamine existing safety requirements. It is also necessary to assess the relative safety of these high speed rail systems which may employ differing equipment and operating procedures than those customarily seen in the United States. This responsibility rests with the Federal Railroad Administration, United States Department of Transportation, which is charged with assuring the safety of rail systems in the United States under the Federal Railroad Safety Act. This report, one in a series of reports planned for high-speed rail technologies, presents an initial review of one such technology, the Swedish tilting train known as the X2000. Additional foreign designed and built tilt trains are available and have been considered for possible application in the United States. Two such technologies, the Spanish Talgo Pendular and the Canadian LRC, were previously offered for testing with the developers' sustaining a major portion of the expense, although they were not subsequently used in revenue service as is now being considered for the X2000. A summary of these tests and a comprehensive review of the state of the art in tilt trains is the subject of a subsequent report. Of note here is that as the Federal Railroad Administration, in its safety endeavors, is consciously trying to avoid placing itself in the position of impeding new technology as a result of its safety regulatory responsibilities.