THERANOSTICS: Regulatory Considerations for Product Development
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Table 2.Iii.1. Fissionable Isotopes1
FISSIONABLE ISOTOPES Charles P. Blair Last revised: 2012 “While several isotopes are theoretically fissionable, RANNSAD defines fissionable isotopes as either uranium-233 or 235; plutonium 238, 239, 240, 241, or 242, or Americium-241. See, Ackerman, Asal, Bale, Blair and Rethemeyer, Anatomizing Radiological and Nuclear Non-State Adversaries: Identifying the Adversary, p. 99-101, footnote #10, TABLE 2.III.1. FISSIONABLE ISOTOPES1 Isotope Availability Possible Fission Bare Critical Weapon-types mass2 Uranium-233 MEDIUM: DOE reportedly stores Gun-type or implosion-type 15 kg more than one metric ton of U- 233.3 Uranium-235 HIGH: As of 2007, 1700 metric Gun-type or implosion-type 50 kg tons of HEU existed globally, in both civilian and military stocks.4 Plutonium- HIGH: A separated global stock of Implosion 10 kg 238 plutonium, both civilian and military, of over 500 tons.5 Implosion 10 kg Plutonium- Produced in military and civilian 239 reactor fuels. Typically, reactor Plutonium- grade plutonium (RGP) consists Implosion 40 kg 240 of roughly 60 percent plutonium- Plutonium- 239, 25 percent plutonium-240, Implosion 10-13 kg nine percent plutonium-241, five 241 percent plutonium-242 and one Plutonium- percent plutonium-2386 (these Implosion 89 -100 kg 242 percentages are influenced by how long the fuel is irradiated in the reactor).7 1 This table is drawn, in part, from Charles P. Blair, “Jihadists and Nuclear Weapons,” in Gary A. Ackerman and Jeremy Tamsett, ed., Jihadists and Weapons of Mass Destruction: A Growing Threat (New York: Taylor and Francis, 2009), pp. 196-197. See also, David Albright N 2 “Bare critical mass” refers to the absence of an initiator or a reflector. -

Security of Supply of Medical Radioisotopes - a Clinical View Dr Beverley Ellis Consultant Radiopharmacist
Security of Supply of Medical Radioisotopes - a clinical view Dr Beverley Ellis Consultant Radiopharmacist Nuclear Medicine Centre Manchester University NHS Foundation Trust Nuclear Medicine § Approx 35 million clinical radionuclide imaging procedures worldwide § Globally 2nd most common imaging technique after CT (higher than MR) 20 million in USA 9 million in Europe 3 million in Japan 3 million in rest of the world Approx 700, 000 nuclear medicine procedures per year in UK Myocardial Perfusion - Ischaemia Stress Stress SA Rest Stress VLA Rest Stress HLA Rest Rest Tc-99m Bone Scans Normal Metastases Mo-99/Tc-99m Generator Supply Tc-99m Radiopharmaceutical Production Mo-99 Shortages Design of Clinical Services to Reduce Tc-99m Use § Optimisation of generator management – Efficiency savings – Delivery and extraction schedules – Patient scheduling § Improved communication – Customers – Suppliers § Improved software – gamma cameras – Produce comparable quality images using less radioactivity Global Situation § OECD/Nuclear Energy Agency (NEA) – Set up High Level Group (HLG-MR) in 2009 – Security of supply of Mo-99 and Tc-99m – Established 6 principles e.g. full cost recovery and outage reserve capacity – Issued a series of publications Global Situation § AIPES (Association of Imaging Producers & Equipment supplies) (Now called Nuclear Medicine Europe) – Support coordination of research reactor schedules Global Situation § Increased Mo-99 Production Capacity – Mo-99 suppliers – acquire additional capacity to cover shortfalls (Outage -

The Supply of Medical Isotopes
The Supply of Medical Isotopes AN ECONOMIC DIAGNOSIS AND POSSIBLE SOLUTIONS The Supply of Medical Isotopes AN ECONOMIC DIAGNOSIS AND POSSIBLE SOLUTIONS The Supply of Medical Isotopes AN ECONOMIC DIAGNOSIS AND POSSIBLE SOLUTIONS This work is published under the responsibility of the Secretary-General of the OECD. The opinions expressed and arguments employed herein do not necessarily reflect the official views of OECD member countries. This document, as well as any data and any map included herein, are without prejudice to the status of or sovereignty over any territory, to the delimitation of international frontiers and boundaries and to the name of any territory, city or area. Please cite this publication as: OECD/NEA (2019), The Supply of Medical Isotopes: An Economic Diagnosis and Possible Solutions, OECD Publishing, Paris, https://doi.org/10.1787/9b326195-en. ISBN 978-92-64-94550-0 (print) ISBN 978-92-64-62509-9 (pdf) The statistical data for Israel are supplied by and under the responsibility of the relevant Israeli authorities. The use of such data by the OECD is without prejudice to the status of the Golan Heights, East Jerusalem and Israeli settlements in the West Bank under the terms of international law. Photo credits: Cover © Yok_onepiece/Shutterstock.com. Corrigenda to OECD publications may be found on line at: www.oecd.org/about/publishing/corrigenda.htm. © OECD 2019 You can copy, download or print OECD content for your own use, and you can include excerpts from OECD publications, databases and multimedia products in your own documents, presentations, blogs, websites and teaching materials, provided that suitable acknowledgement of OECD as source and copyright owner is given. -
Radioisotope Power: a Key Technology for Deep Space Exploration
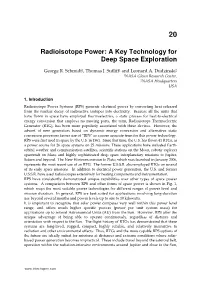
20 Radioisotope Power: A Key Technology for Deep Space Exploration George R. Schmidt1, Thomas J. Sutliff1 and Leonard A. Dudzinski2 1NASA Glenn Research Center, 2NASA Headquarters USA 1. Introduction Radioisotope Power Systems (RPS) generate electrical power by converting heat released from the nuclear decay of radioactive isotopes into electricity. Because all the units that have flown in space have employed thermoelectrics, a static process for heat-to-electrical energy conversion that employs no moving parts, the term, Radioisotope Thermoelectric Generator (RTG), has been more popularly associated with these devices. However, the advent of new generators based on dynamic energy conversion and alternative static conversion processes favors use of “RPS” as a more accurate term for this power technology. RPS were first used in space by the U.S. in 1961. Since that time, the U.S. has flown 41 RTGs, as a power source for 26 space systems on 25 missions. These applications have included Earth- orbital weather and communication satellites, scientific stations on the Moon, robotic explorer spacecraft on Mars, and highly sophisticated deep space interplanetary missions to Jupiter, Saturn and beyond. The New Horizons mission to Pluto, which was launched in January 2006, represents the most recent use of an RTG. The former U.S.S.R. also employed RTGs on several of its early space missions. In addition to electrical power generation, the U.S. and former U.S.S.R. have used radioisotopes extensively for heating components and instrumentation. RPS have consistently demonstrated unique capabilities over other types of space power systems. A comparison between RPS and other forms of space power is shown in Fig. -

Space Isotopic Power Systems
Space isotopiC power systems With the technology sound and growing, and units already built for missions ranging from 120 days to 5 years, the designer can and should plan appropriate space application of isotopic systems BY CAPT. R. T. CARPENTER, USAF U.S. Atomic Energy Commission A new space power system technology technology, and aerospace nuclear Concurrently, the terrestrial appli -isotopic power-has developed to safety technology contributed by the cations-the Snap-7 programs-sus the point where it can and should be program and used as a foundation for tained the isotopic power development considered by the space-vehicle de follow-on space isotopic power-system program and promoted the fission signer for use in many types of mis developments. product separations and processing sions. Because of this sound technical capability that exists within the Com The' Atomic Energy Commission's basis, the Commission's space-oriented mission today! The interest among isotopic space power program dates isotopic power development program terrestrial power users-the Navy, back to several years before Sputnik has made a steady, although some Weather Bureau, and Coast Guard I, but the program suffered a severe times slow, comeback through a series was sufficiently strong to sup:port this setback in 1959 when the Snap-1A of events since 1959, so that today a . fuels production program, whe:r:eas the generator development program was program technically comparable to interest in Snap-1A had been inade cancelled.' This pioneer program was Snap-1A could once more be under quate. At the same time, significant not completed because it may have taken with a high probability of suc quantities of the long-lived alpha been tt;lO ambitious for its day. -
CURIUM Element Symbol: Cm Atomic Number: 96
CURIUM Element Symbol: Cm Atomic Number: 96 An initiative of IYC 2011 brought to you by the RACI ROBYN SILK www.raci.org.au CURIUM Element symbol: Cm Atomic number: 96 Curium is a radioactive metallic element of the actinide series, and named after Marie Skłodowska-Curie and her husband Pierre, who are noted for the discovery of Radium. Curium was the first element to be named after a historical person. Curium is a synthetic chemical element, first synthesized in 1944 by Glenn T. Seaborg, Ralph A. James, and Albert Ghiorso at the University of California, Berkeley, and then formally identified by the same research tea at the wartime Metallurgical Laboratory (now Argonne National Laboratory) at the University of Chicago. The discovery of Curium was closely related to the Manhattan Project, and thus results were kept confidential until after the end of World War II. Seaborg finally announced the discovery of Curium (and Americium) in November 1945 on ‘The Quiz Kids!’, a children’s radio show, five days before an official presentation at an American Chemical Society meeting. The first radioactive isotope of Curium discovered was Curium-242, which was made by bombarding alpha particles onto a Plutonium-239 target in a 60-inch cyclotron (University of California, Berkeley). Nineteen radioactive isotopes of Curium have now been characterized, ranging in atomic mass from 233 to 252. The most stable radioactive isotopes are Curium- 247 with a half-life of 15.6 million years, Curium-248 (half-life 340,000 years), Curium-250 (half-life of 9000 years), and Curium-245 (half-life of 8500 years). -

Curium Is the First North American Manufacturer Offering Exclusively 100% LEU Generators
FOR IMMEDIATE RELEASE January 16, 2018 Curium Is the First North American Manufacturer Offering Exclusively 100% LEU Generators (St. Louis - January 16, 2018) — Curium, a leading nuclear medicine solutions provider, announced today that the company is the first North American manufacturer to meet the deadline established by the American Medical Isotopes Production Act of 2012. This legislation effectively mandates the full conversion away from highly enriched uranium (HEU) as soon as possible and no later than January 2020. Curium’s multi-year project to transition its molybdenum-99 (Mo-99) processing facility from HEU to low enriched uranium (LEU) was completed in late-2017. This project makes Curium the only North American Technetium Tc 99m Generator manufacturer able to supply its customers exclusively with 100 percent LEU Tc 99m generators. Mo-99 is the parent isotope of Tc 99m, which is used in 30 to 40 million nuclear medicine procedures worldwide every year1. Curium is the world’s largest supplier of Tc 99m generators and the largest user of Mo- 99 in the world. “This milestone helps satisfy the goals set forth by the Department of Energy’s (DOE) National Nuclear Security Administration (NNSA) and confirms our support for the NNSA project to eliminate the use of weapons-grade uranium in the production of medical isotopes. We are eager to see others follow our lead and comply with the government’s call for full conversion as soon possible” says Curium North American CEO, Dan Brague. This project is the culmination of more than seven years of work, requiring close collaboration with Curium’s irradiation partners: the Dutch High Flux Reactor, the Polish MARIA reactor, and BR2 in Belgium, as well as, the DOE and NNSA. -

Background, Status and Issues Related to the Regulation of Advanced Spent Nuclear Fuel Recycle Facilities
NUREG-1909 Background, Status, and Issues Related to the Regulation of Advanced Spent Nuclear Fuel Recycle Facilities ACNW&M White Paper Advisory Committee on Nuclear Waste and Materials NUREG-1909 Background, Status, and Issues Related to the Regulation of Advanced Spent Nuclear Fuel Recycle Facilities ACNW&M White Paper Manuscript Completed: May 2008 Date Published: June 2008 Prepared by A.G. Croff, R.G. Wymer, L.L. Tavlarides, J.H. Flack, H.G. Larson Advisory Committee on Nuclear Waste and Materials THIS PAGE WAS LEFT BLANK INTENTIONALLY ii ABSTRACT In February 2006, the Commission directed the Advisory Committee on Nuclear Waste and Materials (ACNW&M) to remain abreast of developments in the area of spent nuclear fuel reprocessing, and to be ready to provide advice should the need arise. A white paper was prepared in response to that direction and focuses on three major areas: (1) historical approaches to development, design, and operation of spent nuclear fuel recycle facilities, (2) recent advances in spent nuclear fuel recycle technologies, and (3) technical and regulatory issues that will need to be addressed if advanced spent nuclear fuel recycle is to be implemented. This white paper was sent to the Commission by the ACNW&M as an attachment to a letter dated October 11, 2007 (ML072840119). In addition to being useful to the ACNW&M in advising the Commission, the authors believe that the white paper could be useful to a broad audience, including the NRC staff, the U.S. Department of Energy and its contractors, and other organizations interested in understanding the nuclear fuel cycle. -
A Roadmap for Replacing High-Risk Radioactive Sources and Materials
1 Permanent Risk Reduction: A Roadmap for Replacing High-Risk Radioactive Sources and Materials Miles A. Pomper James Martin Center for Nonproliferation Studies The National Academies of Sciences Radioactive Sources: Applications and Alternative Technologies Meeting January 31, 2020 2 Overview • CNS Workshops and Studies • Materials of Security Concern • Uses of Current High-Risk Materials ▫ Medicine ▫ Oil and gas industry • Strategy for Replacing High Activity Sources • Replacement Priority • Encouraging Replacement: Actions • Conclusions 3 CNS Workshops and Studies Since 2008, CNS has led a series of workshops and studies: . Alternatives to High-Risk Radiological Sources: The Case of Cesium Chloride in Blood Irradiation (2014) . Permanent Risk Reduction: A Roadmap for Replacing High-Risk Radioactive Sources and Materials (2015) . Treatment Not Terror: Strategies to Enhance External Beam Cancer Therapy in Developing Countries While Permanently Reducing the Risk of Radiological Terrorism (2016) . Additional material since: for NYC, NTI, and IAEA ICONS, draft language for 2016 NSS 4 Important Current Uses for High-Risk Materials, Existing Alternatives and Challenges, and Suggested Next Steps 5 High-Risk Sources • A task force report by the NRC listed 1. Americium-241 (Am-241) 2. Am-241/Beryllium (Be) 16 radionuclides as those of principal 3. Californium-252 (Cf-252) concern when considering the 4. Cesium-137 (Cs-137) problems they would cause if used in a 5. Cobalt-60 (Co-60) radiological dispersion device (RDD) 6. Curium-244 (Cm-244) • Considered an immediate danger only 7. Gadolinium-153 (Gd-153) when found in large enough amounts 8. Iridium-192 (Ir-192) to threaten life or cause severe 9. -

Meeting Summary
MEETING OF THE ADVISORY COMMITTEE ON THE MEDICAL USES OF ISOTOPES March 16, 2021 MEETING SUMMARY PURPOSE To discuss issues related to the implementation of the medical regulations in Title 10 of the Code of Federal Regulations (10 CFR) Part 35, “Medical Use of Byproduct Material.” OUTCOME The Advisory Committee on the Medical Uses of Isotopes (ACMUI) made recommendations, and the U.S. Nuclear Regulatory Commission (NRC) staff gained a better understanding of the views and opinions of the ACMUI, as well as other stakeholders’ views and opinions. The NRC staff will consider these views in its continuing effort to make 10 CFR Part 35 more useful, practical, and not overly burdensome on licensees, while maintaining public health and safety. Full transcripts and handouts from the ACMUI meeting can be found on the NRC’s ACMUI Meetings webpage, located at: https://www.nrc.gov/reading-rm/doc-collections/acmui/meetings/. The meeting attendees are listed in Enclosure 1. RECOMMENDATIONS AND ACTIONS The following provides a summary of the discussions that took place on the topics listed on the ACMUI meeting agenda (Enclosure 2): Dr. Jochem van der Pol of Maastricht University, located in Maastricht, Netherlands, provided an overview of his study on the consequences of radiopharmaceutical extravasation and interventions. Dr. Katie Tapp provided an overview of the NRC staff’s evaluation of patient release considerations associated with temporary brachytherapy devices. The NRC staff is currently developing a draft 10 CFR 35.1000 licensing guidance for the Alpha DaRT and plans to provide to the ACMUI for review in summer 2021. -
Curium and the Transactinides
Curium and the Transactinides Dr Clint Sharrad Centre for Radiochemistry Research School of Chemical Engineering and Analytical Science Research Centre for Radwaste and Decommissioning Dalton Nuclear Institute The University of Manchester [email protected] Marie Curie No involvement in the discovery of curium or the transactinides. Who first discovered Cm? Glenn T. Albert Ralph A. Seaborg Ghiorso James • Nobel prize for Chemistry 1951 • Discovered 10 elements • Discovered 12 elements • Expert in developing radiation detection 1912 - 1999 instrumentation 1915 - 2010 G. T. Seaborg, R. A. James and A. Ghiorso, National Nuclear Energy Series , 1949, 14B , 1554-71. Was anyone else involved in the discovery of curium??? Stanley G. Thompson Submitted Ph.D. thesis entitled “Nuclear and Chemical Properties of Americium and Curium” in 1948 Why Curium? G. T. Seaborg, R. A. James and A. Ghiorso, National Nuclear Energy Series , 1949, 14B , 1554-71. Vasili Samarsky- Johan Why Bykhovets Gadolin Curium? Lanthanides Actinides Marie & Pierre Albert Einstein Enrico Dmitri Alfred Ernest Transactinides Curie Fermi Mendelev Noble Lawrence Cn Copernicium (285) Ernest Glenn T. Niels Bohr Lise Wilhelm Nicolaus Rutherford Seaborg Meitner Roentgen Copernicus 1850 Timeline 1859 – Pierre Curie born 1867 – Maria Skłodowska born 1891 – Maria Skłodowska moves to Paris to study chemistry at the Sarbonne 1895– Maria Skłodowska marries Pierre Curie 1898– Curie’s publish discovery of Po and Ra 1903– Curie’s awarded Nobel prize for physics (with Becquerel) 1906– Death of Pierre Curie 1911 – Marie Curie awarded Nobel prize for chemistry 1912 – Glenn Seaborg born 1915– Albert Ghiorso born 1934– Death of Marie Curie; Seaborg awarded B.Sc. -

FDA-Approved Radiopharmaceuticals
Medication Management FDA-approved radiopharmaceuticals This is a current list of all FDA-approved radiopharmaceuticals. USP <825> requires the use of conventionally manufactured drug products (e.g., NDA, ANDA) for Immediate Use. Nuclear medicine practitioners that receive radiopharmaceuticals that originate from sources other than the manufacturers listed in these tables may be using unapproved copies. Radiopharmaceutical Manufacturer Trade names Approved indications in adults (Pediatric use as noted) 1 Carbon-11 choline Various - Indicated for PET imaging of patients with suspected prostate cancer recurrence based upon elevated blood prostate specific antigen (PSA) levels following initial therapy and non-informative bone scintigraphy, computerized tomography (CT) or magnetic resonance imaging (MRI) to help identify potential sites of prostate cancer recurrence for subsequent histologic confirmation 2 Carbon-14 urea Halyard Health PYtest Detection of gastric urease as an aid in the diagnosis of H.pylori infection in the stomach 3 Copper-64 dotatate Curium Detectnet™ Indicated for use with positron emission tomography (PET) for localization of somatostatin receptor positive neuroendocrine tumors (NETs) in adult patients 4 Fluorine-18 florbetaben Life Molecular Neuraceq™ Indicated for Positron Emission Tomography (PET) imaging of the brain to Imaging estimate β amyloid neuritic plaque density in adult patients with cognitive impairment who are being evaluated for Alzheimer’s disease (AD) or other causes of cognitive decline 5 Fluorine-18