Epigenetic Therapy with Panobinostat Combined with Bicalutamide Rechallenge in Castration- Resistant Prostate Cancer Anna C
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

CASODEX (Bicalutamide)
HIGHLIGHTS OF PRESCRIBING INFORMATION • Gynecomastia and breast pain have been reported during treatment with These highlights do not include all the information needed to use CASODEX 150 mg when used as a single agent. (5.3) CASODEX® safely and effectively. See full prescribing information for • CASODEX is used in combination with an LHRH agonist. LHRH CASODEX. agonists have been shown to cause a reduction in glucose tolerance in CASODEX® (bicalutamide) tablet, for oral use males. Consideration should be given to monitoring blood glucose in Initial U.S. Approval: 1995 patients receiving CASODEX in combination with LHRH agonists. (5.4) -------------------------- RECENT MAJOR CHANGES -------------------------- • Monitoring Prostate Specific Antigen (PSA) is recommended. Evaluate Warnings and Precautions (5.2) 10/2017 for clinical progression if PSA increases. (5.5) --------------------------- INDICATIONS AND USAGE -------------------------- ------------------------------ ADVERSE REACTIONS ----------------------------- • CASODEX 50 mg is an androgen receptor inhibitor indicated for use in Adverse reactions that occurred in more than 10% of patients receiving combination therapy with a luteinizing hormone-releasing hormone CASODEX plus an LHRH-A were: hot flashes, pain (including general, back, (LHRH) analog for the treatment of Stage D2 metastatic carcinoma of pelvic and abdominal), asthenia, constipation, infection, nausea, peripheral the prostate. (1) edema, dyspnea, diarrhea, hematuria, nocturia, and anemia. (6.1) • CASODEX 150 mg daily is not approved for use alone or with other treatments. (1) To report SUSPECTED ADVERSE REACTIONS, contact AstraZeneca Pharmaceuticals LP at 1-800-236-9933 or FDA at 1-800-FDA-1088 or ---------------------- DOSAGE AND ADMINISTRATION ---------------------- www.fda.gov/medwatch The recommended dose for CASODEX therapy in combination with an LHRH analog is one 50 mg tablet once daily (morning or evening). -

COVID-19—The Potential Beneficial Therapeutic Effects of Spironolactone During SARS-Cov-2 Infection
pharmaceuticals Review COVID-19—The Potential Beneficial Therapeutic Effects of Spironolactone during SARS-CoV-2 Infection Katarzyna Kotfis 1,* , Kacper Lechowicz 1 , Sylwester Drozd˙ zal˙ 2 , Paulina Nied´zwiedzka-Rystwej 3 , Tomasz K. Wojdacz 4, Ewelina Grywalska 5 , Jowita Biernawska 6, Magda Wi´sniewska 7 and Miłosz Parczewski 8 1 Department of Anesthesiology, Intensive Therapy and Acute Intoxications, Pomeranian Medical University in Szczecin, 70-111 Szczecin, Poland; [email protected] 2 Department of Pharmacokinetics and Monitored Therapy, Pomeranian Medical University, 70-111 Szczecin, Poland; [email protected] 3 Institute of Biology, University of Szczecin, 71-412 Szczecin, Poland; [email protected] 4 Independent Clinical Epigenetics Laboratory, Pomeranian Medical University, 71-252 Szczecin, Poland; [email protected] 5 Department of Clinical Immunology and Immunotherapy, Medical University of Lublin, 20-093 Lublin, Poland; [email protected] 6 Department of Anesthesiology and Intensive Therapy, Pomeranian Medical University in Szczecin, 71-252 Szczecin, Poland; [email protected] 7 Clinical Department of Nephrology, Transplantology and Internal Medicine, Pomeranian Medical University, 70-111 Szczecin, Poland; [email protected] 8 Department of Infectious, Tropical Diseases and Immune Deficiency, Pomeranian Medical University in Szczecin, 71-455 Szczecin, Poland; [email protected] * Correspondence: katarzyna.kotfi[email protected]; Tel.: +48-91-466-11-44 Abstract: In March 2020, coronavirus disease 2019 (COVID-19) caused by SARS-CoV-2 was declared Citation: Kotfis, K.; Lechowicz, K.; a global pandemic by the World Health Organization (WHO). The clinical course of the disease is Drozd˙ zal,˙ S.; Nied´zwiedzka-Rystwej, unpredictable but may lead to severe acute respiratory infection (SARI) and pneumonia leading to P.; Wojdacz, T.K.; Grywalska, E.; acute respiratory distress syndrome (ARDS). -

Hormonal Treatment Strategies Tailored to Non-Binary Transgender Individuals
Journal of Clinical Medicine Review Hormonal Treatment Strategies Tailored to Non-Binary Transgender Individuals Carlotta Cocchetti 1, Jiska Ristori 1, Alessia Romani 1, Mario Maggi 2 and Alessandra Daphne Fisher 1,* 1 Andrology, Women’s Endocrinology and Gender Incongruence Unit, Florence University Hospital, 50139 Florence, Italy; [email protected] (C.C); jiska.ristori@unifi.it (J.R.); [email protected] (A.R.) 2 Department of Experimental, Clinical and Biomedical Sciences, Careggi University Hospital, 50139 Florence, Italy; [email protected]fi.it * Correspondence: fi[email protected] Received: 16 April 2020; Accepted: 18 May 2020; Published: 26 May 2020 Abstract: Introduction: To date no standardized hormonal treatment protocols for non-binary transgender individuals have been described in the literature and there is a lack of data regarding their efficacy and safety. Objectives: To suggest possible treatment strategies for non-binary transgender individuals with non-standardized requests and to emphasize the importance of a personalized clinical approach. Methods: A narrative review of pertinent literature on gender-affirming hormonal treatment in transgender persons was performed using PubMed. Results: New hormonal treatment regimens outside those reported in current guidelines should be considered for non-binary transgender individuals, in order to improve psychological well-being and quality of life. In the present review we suggested the use of hormonal and non-hormonal compounds, which—based on their mechanism of action—could be used in these cases depending on clients’ requests. Conclusion: Requests for an individualized hormonal treatment in non-binary transgender individuals represent a future challenge for professionals managing transgender health care. For each case, clinicians should balance the benefits and risks of a personalized non-standardized treatment, actively involving the person in decisions regarding hormonal treatment. -

Feminizing Hormone Therapy
FEMINIZING HORMONE THERAPY Julie Thompson, PA-C Medical Director of Trans Health, Fenway Health April 2020 fenwayhealth.org GOALS AND OBJECTIVES 1. Review process of initiating hormone therapy through the informed consent model 2. Provide an overview of feminizing hormone therapy 3. Review realistic expectations and benefits of hormone therapy vs their associated risks 4. Discuss recommendations for monitoring fenwayhealth.org PROTOCOLS AND STANDARDS OF CARE fenwayhealth.org WPATH STANDARDS OF CARE, 2011 The criteria for hormone therapy are as follows: 1. Well-documented, persistent (at least 6mo) gender dysphoria 2. Capacity to make a fully informed decision and to consent for treatment 3. Age of majority in a given country 4. If significant medical or mental health concerns are present, they must be reasonably well controlled fenwayhealth.org INFORMED CONSENT MODEL ▪ Requires healthcare provider to ▪ Effectively communicate benefits, risks and alternatives of treatment to patient ▪ Assess that the patient is able to understand and consent to the treatment ▪ Informed consent model does not preclude mental health care! ▪ Recognizes that prescribing decision ultimately rests with clinical judgment of provider working together with the patient ▪ Recognizes patient autonomy and empowers self-agency ▪ Decreases barriers to medically necessary care fenwayhealth.org INITIAL VISITS ▪ Review history of gender experience and patient’s goals ▪ Document prior hormone use ▪ Assess appropriateness for gender affirming medical treatment ▪ WPATH criteria -

Minutes of PRAC Meeting on 09-12 July 2018
6 September 2018 EMA/PRAC/576790/2018 Inspections, Human Medicines Pharmacovigilance and Committees Division Pharmacovigilance Risk Assessment Committee (PRAC) Minutes of the meeting on 09-12 July 2018 Chair: June Raine – Vice-Chair: Almath Spooner Health and safety information In accordance with the Agency’s health and safety policy, delegates were briefed on health, safety and emergency information and procedures prior to the start of the meeting. Disclaimers Some of the information contained in the minutes is considered commercially confidential or sensitive and therefore not disclosed. With regard to intended therapeutic indications or procedure scope listed against products, it must be noted that these may not reflect the full wording proposed by applicants and may also change during the course of the review. Additional details on some of these procedures will be published in the PRAC meeting highlights once the procedures are finalised. Of note, the minutes are a working document primarily designed for PRAC members and the work the Committee undertakes. Note on access to documents Some documents mentioned in the minutes cannot be released at present following a request for access to documents within the framework of Regulation (EC) No 1049/2001 as they are subject to on- going procedures for which a final decision has not yet been adopted. They will become public when adopted or considered public according to the principles stated in the Agency policy on access to documents (EMA/127362/2006, Rev. 1). 30 Churchill Place ● Canary Wharf ● London E14 5EU ● United Kingdom Telephone +44 (0)20 3660 6000 Facsimile +44 (0)20 3660 5555 Send a question via our website www.ema.europa.eu/contact An agency of the European Union © European Medicines Agency, 2018. -

Solubility of Bicalutamide, Megestrol Acetate, Prednisolone
Article pubs.acs.org/jced Solubility of Bicalutamide, Megestrol Acetate, Prednisolone, Beclomethasone Dipropionate, and Clarithromycin in Subcritical Water at Different Temperatures from 383.15 to 443.15 K † ⊥ ‡ † ⊥ † † † Yuan Pu, , Fuhong Cai, Dan Wang,*, , Yinhua Li, Xiaoyuan Chen, Amadou G. Maimouna, † † † ⊥ † § Zhengxiang Wu, Xiaofei Wen, Jian-Feng Chen, , and Neil R. Foster , † Beijing Advanced Innovation Center for Soft Matter Science and Engineering, State Key Laboratory of Organic−Inorganic Composites, Beijing University of Chemical Technology, Beijing 100029, China ‡ College of Mechanical and Electrical Engineering, Hainan University, Haikou 570228, China § Department of Chemical Engineering, Curtin University, Perth, Western Australia 6102, Australia ⊥ Research Center of the Ministry of Education for High Gravity Engineering and Technology, Beijing University of Chemical Technology, Beijing 100029, China ABSTRACT: The solubility of bicalutamide, megestrol acetate, prednisolone, beclomethasone dipropionate, and clarithromycin in subcritical water (SBCW) at the temperature range from 383.15 to 443.15 K and constant pressure of 5.5 MPa were measured using a modified solvent−antisolvent method combined with SBCW technology. The chemical structures of these five kinds of solutes were stable after processed in SBCW at up to 443.15 K, which was demonstrated by Fourier transformed infrared analysis. The solubility of selected solutes increased exponentially as the temperature of the SBCW increased from 383.15 to 443.15 K. The obtained -

Long Term Hormone Treatment
Long Term Hormone Treatment Your hospital doctor has recommended that you have treatment using hormones. Please follow the following guidelines: Collect your tablets and first injection from the hospital pharmacy. Make an appointment at your GP surgery to have the first injection, called *Zoladex or Decapeptyl, for 2 weeks after you have started taking the tablets. Take the tablets, for 4 weeks in total, 2 weeks before the first injection continuing for 2 weeks after the first injection, and then stop – this will be Bicalutamide, 1 tablet each day or Cyproterone acetate (CPA) 1 tablet 3 times a day. You should also take the Bicalutamide or Cyproterone Acetate tablet on the day of your first injection. Arrange to have the second Zoladex injection at your GP surgery 4 weeks after the first injection. Subsequent injections can be given at 12 week intervals using the long acting Zoladex or Decapeptyl injection. Continue all your other medications unless the hospital doctor or your GP advises otherwise. If you are unsure about the tablets or injections either ask your GP for advice or telephone the specialist nurses, Jane Thacker, on 01284 712735 or Oncology CNS on 01284 713212 (or 01284 713000 bleep 874) for guidance. Please have a PSA (Prostate Specific Antigen) blood test done at your GP surgery a Source: Oncology Reference No: 5161-4 Issue date: 17/01/18 Review date: 17/01/20 Page 1 of 2 week before each visit to the hospital urology or oncology clinic. Week 1 Bicalutamide or CPA Week 2 Bicalutamide or CPA First Injection Week 3 Bicalutamide or CPA Week 4 Bicalutamide or CPA Week 6 Injection every 12 weeks *Zoladex is the trade name for Goserelin If you would like any information regarding access to the West Suffolk Hospital and its facilities please visit the disabledgo website link below: http://www.disabledgo.com/organisations/west-suffolk-nhs-foundation-trust/main © West Suffolk NHS Foundation Trust Paddock House, Eye 0333 321 8604 Bluebird Lodge, Ipswich . -

Aetna Formulary Exclusions Drug List
Covered and non-covered drugs Drugs not covered – and their covered alternatives 2020 Advanced Control Plan – Aetna Formulary Exclusions Drug List 05.03.525.1B (7/20) Below is a list of medications that will not be covered without a Key prior authorization for medical necessity. If you continue using one of these drugs without prior approval, you may be required UPPERCASE Brand-name medicine to pay the full cost. Ask your doctor to choose one of the generic lowercase italics Generic medicine or brand formulary options listed below. Preferred Options For Excluded Medications1 Excluded drug name(s) Preferred option(s) ABILIFY aripiprazole, clozapine, olanzapine, quetiapine, quetiapine ext-rel, risperidone, ziprasidone, VRAYLAR ABSORICA isotretinoin ACANYA adapalene, benzoyl peroxide, clindamycin gel (except NDC^ 68682046275), clindamycin solution, clindamycin-benzoyl peroxide, erythromycin solution, erythromycin-benzoyl peroxide, tretinoin, EPIDUO, ONEXTON, TAZORAC ACIPHEX, esomeprazole, lansoprazole, omeprazole, pantoprazole, DEXILANT ACIPHEX SPRINKLE ACTICLATE doxycycline hyclate capsule, doxycycline hyclate tablet (except doxycycline hyclate tablet 50 mg [NDC^ 72143021160 only], 75 mg, 150 mg), minocycline, tetracycline ACTOS pioglitazone ACUVAIL bromfenac, diclofenac, ketorolac, PROLENSA acyclovir cream acyclovir (except acyclovir cream), valacyclovir ADCIRCA sildenafil, tadalafil ADZENYS XR-ODT amphetamine-dextroamphetamine mixed salts ext-rel†, dexmethylphenidate ext-rel, dextroamphetamine ext-rel, methylphenidate ext-rel†, MYDAYIS, -

The Role of Highly Selective Androgen Receptor (AR) Targeted
P h a s e I I S t u d y o f I t r a c o n a z o l e i n B i o c h e m i c a l R e l a p s e Version 4.0: October 8, 2014 CC# 125513 CC# 125513: Hedgehog Inhibition as a Non-Castrating Approach to Hormone Sensitive Prostate Cancer: A Phase II Study of Itraconazole in Biochemical Relapse Investigational Agent: Itraconazole IND: IND Exempt (IND 116597) Protocol Version: 4.0 Version Date: October 8, 2014 Principal Investigator: Rahul Aggarwal, M.D., HS Assistant Clinical Professor Division of Hematology/Oncology, Department of Medicine University of California San Francisco 1600 Divisadero St. San Francisco, CA94115 [email protected] UCSF Co-Investigators: Charles J. Ryan, M.D., Eric Small, M.D., Professor of Medicine Professor of Medicine and Urology Lawrence Fong, M.D., Terence Friedlander, M.D., Professor in Residence Assistant Clinical Professor Amy Lin, M.D., Associate Clinical Professor Won Kim, M.D., Assistant Clinical Professor Statistician: Li Zhang, Ph.D, Biostatistics Core RevisionHistory October 8, 2014 Version 4.0 November 18, 2013 Version 3.0 January 28, 2013 Version 2.0 July 16, 2012 Version 1.0 Phase II - Itraconazole Page 1 of 79 P h a s e I I S t u d y o f I t r a c o n a z o l e i n B i o c h e m i c a l R e l a p s e Version 4.0: October 8, 2014 CC# 125513 Protocol Signature Page Protocol No.: 122513 Version # and Date: 4.0 - October 8, 2014 1. -

Feminizing Gender-Affirming Hormone Care the Michigan Medicine Approach
Feminizing Gender-Affirming Hormone Care The Michigan Medicine Approach Our goal is to partner with you to provide the medical care you need in affirming your gender. Our focus is on your lifelong health, safety, and individual medical and transition-related needs. The Michigan Medicine approach is based on the limited but growing medical evidence surrounding gender-affirming hormone care. Based on the available science, we believe mimicking normal physiology will provide you with the best balance of physical and emotional changes and long-term health. This philosophy aligns with current national and international medical guidelines in the care of gender diverse people. We are committed to staying up-to-date with the latest research and medical evidence to ensure you are getting the highest quality care. We know that there are competing approaches to gender-affirming care that are not based on validated scientific evidence. These approaches make scientifically unsubstantiated claims and have unknown short and long-term risks. We are happy to discuss these with you. Below are some answers to questions our patients have asked us about gender- affirming hormone care. We hope the Q&A will help you understand the medical evidence behind our approach to your gender-affirming hormone care, and how it may differ from other approaches, including the approach other well-known clinics in Southeast Michigan. Is there a benefit for monitoring both estrone (E1) and estradiol (E2) levels and aiming for a particular ratio? There are 3 naturally occurring human estrogens: estrone (E1), estradiol (E2), and estriol (E3). Your body naturally balances your estradiol and estrone ratio. -

OUH Formulary Approved for Use in Breast Surgery
Oxford University Hospitals NHS Foundation Trust Formulary FORMULARY (Y): the medicine can be used as per its licence. RESTRICTED FORMULARY (R): the medicine can be used as per the agreed restriction. NON-FORMULARY (NF): the medicine is not on the formulary and should not be used unless exceptional approval has been obtained from MMTC. UNLICENSED MEDICINE – RESTRICTED FORMULARY (UNR): the medicine is unlicensed and can be used as per the agreed restriction. SPECIAL MEDICINE – RESTRICTED FORMULARY (SR): the medicine is a “special” (unlicensed) and can be used as per the agreed restriction. EXTEMPORANEOUS PREPARATION – RESTRICTED FORMULARY (EXTR): the extemporaneous preparation (unlicensed) can be prepared and used as per the agreed restriction. UNLICENSED MEDICINE – NON-FORMULARY (UNNF): the medicine is unlicensed and is not on the formulary. It should not be used unless exceptional approval has been obtained from MMTC. SPECIAL MEDICINE – NON-FORMULARY (SNF): the medicine is a “special” (unlicensed) and is not on the formulary. It should not be used unless exceptional approval has been obtained from MMTC. EXTEMPORANEOUS PREPARATION – NON-FORMULARY (EXTNF): the extemporaneous preparation (unlicensed) cannot be prepared and used unless exceptional approval has been obtained from MMTC. CLINICAL TRIALS (C): the medicine is clinical trial material and is not for clinical use. NICE TECHNOLOGY APPRAISAL (NICETA): the medicine has received a positive appraisal from NICE. It will be available on the formulary from the day the Technology Appraisal is published. Prescribers who wish to treat patients who meet NICE criteria, will have access to these medicines from this date. However, these medicines will not be part of routine practice until a NICE TA Implementation Plan has been presented and approved by MMTC (when the drug will be given a Restricted formulary status). -
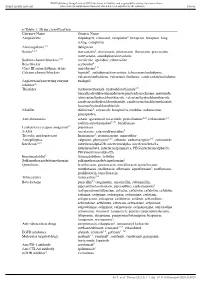
E-Table 1. Drug Classification Category Name Generic Name
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any reliance Supplemental material placed on this supplemental material which has been supplied by the author(s) Thorax e-Table 1. Drug classification Category Name Generic Name Antiplatelets clopidogrel, cilostazol, ticlopidine2, beraprost, beraprost–long acting, complavin Anticoagulants 2,3 dabigatran Statins1,2,3 atorvastatin2, simvastatin, pitavastatin, fluvastatin, pravastatin, rosuvastatin, amlodipine/atorvastatin Sodium channel blockers4,5† mexiletine, aprindine, cibenzoline Beta blocker acebutolol2 Class III antiarrhythmic drugs amiodarone1–6 Calcium channel blockers bepridil1, amlodipine/atorvastatin, telmisartan/amlodipine, valsartan/amlodipine, valsartan/cilnidipine, candesartan/amlodipine Angiotensin/converting enzyme enalapril inhibitor2‡ Thiazides trichlormethiazide, hydrochlorothiazide3,5, benzylhydrochlorothiazide/reserpine/carbazochrome, mefruside, telmisartan/hydrochlorothiazide, valsartan/hydrochlorothiazide, candesartan/hydrochlorothiazide, candesartan/trichlormethiazide, losartan/hydrochlorothiazide NSAIDs diclofenac2, celecoxib, loxoprofen, etodolac, nabumetone, pranoprofen Anti-rheumatics actarit, iguratimod, tofacitinib, penicillamine2–5, leflunomide1,3, sodium aurothiomalate2–6#, bucillamine Leukotriene receptor antagonist2* pranlukast 5-ASA mesalazine, salazosulfapyridine5 Tricyclic antidepressant Imipramine5, cromipramine, maprotiline Antiepileptics valproate, phenytoin2,3,5, ethotoin, carbamazepine2–5, zonisamide Interferon1,2,3