Isolation and Identification of Geosmithia Argillacea from A
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

De Novo Genome Assembly of Geosmithia Morbida, the Causal Agent of Thousand Cankers Disease
De novo genome assembly of Geosmithia morbida, the causal agent of thousand cankers disease Taruna A. Schuelke1, Anthony Westbrook2, Kirk Broders3, Keith Woeste4 and Matthew D. MacManes1 1 Department of Molecular, Cellular, & Biomedical Sciences, University of New Hampshire, Durham, New Hampshire, United States 2 Department of Computer Science, University of New Hampshire, Durham, New Hampshire, United States 3 Department of Bioagricultural Sciences and Pest Management, Colorado State University, Fort Collins, Colorado, United States 4 Hardwood Tree Improvement and Regeneration Center, USDA Forest Service, West Lafayette, Indiana, United States ABSTRACT Geosmithia morbida is a filamentous ascomycete that causes thousand cankers disease in the eastern black walnut tree. This pathogen is commonly found in the western U.S.; however, recently the disease was also detected in several eastern states where the black walnut lumber industry is concentrated. G. morbida is one of two known phytopathogens within the genus Geosmithia, and it is vectored into the host tree via the walnut twig beetle. We present the first de novo draft genome of G. morbida. It is 26.5 Mbp in length and contains less than 1% repetitive elements. The genome possesses an estimated 6,273 genes, 277 of which are predicted to encode proteins with unknown functions. Approximately 31.5% of the proteins in G. morbida are homologous to proteins involved in pathogenicity, and 5.6% of the proteins contain signal peptides that indicate these proteins are secreted. Several studies have investigated the evolution of pathogenicity in pathogens of agricultural crops; forest fungal pathogens are often neglected because research Submitted 21 January 2016 efforts are focused on food crops. -

Eastern Black Walnut (Juglans Nigra L.) Originating from Native Range Varies in Their Response to Inoculation with Geosmithia Morbida
ffgc-04-627911 March 3, 2021 Time: 17:19 # 1 ORIGINAL RESEARCH published: 09 March 2021 doi: 10.3389/ffgc.2021.627911 Eastern Black Walnut (Juglans nigra L.) Originating From Native Range Varies in Their Response to Inoculation With Geosmithia morbida Rachael A. Sitz1,2*, Emily K. Luna2, Jorge Ibarra Caballero2, Ned A. Tisserat2, Whitney S. Cranshaw2, James R. McKenna3, Joshua Stolz4 and Jane E. Stewart2* 1 Davey Resource Group, Inc., Urban & Community Forestry Services, Atascadero, CA, United States, 2 Colorado State University, Department of Agricultural Biology, Fort Collins, CO, United States, 3 USDA Forest Service Hardwood Tree Improvement and Regeneration Center, West Lafayette, IN, United States, 4 Colorado State Forest Service Nursery, Fort Collins, CO, United States Edited by: Mariangela N. Fotelli, Thousand cankers disease (TCD) is caused by the walnut twig beetle (Pityophthorus Hellenic Agricultural Organization, Greece juglandis) vectoring the fungal canker pathogen Geosmithia morbida, which can result Reviewed by: in severe dieback and eventual death to species of walnut (Juglans spp.) and wingnut Jackson Audley, (Pterocarya spp.). This disease is most devastating to the highly valued species J. nigra USDA Forest Service, United States (black walnut). This species is primarily grown and harvested for timber production in Pierluigi (Enrico) Bonello, The Ohio State University, the Central Hardwood Region of the United States, which comprises part of its native United States range. Management options for TCD are limited; therefore, finding resistant genotypes *Correspondence: is needed. Initial studies on black walnut susceptibility to G. morbida documented Rachael A. Sitz [email protected] some genetic variation and suggested potential resistance. -

Method for Isolating and Maintaining Cultures of Geosmithia from Juglans Nigra
Method for Isolating and Maintaining Cultures of Geosmithia from Juglans nigra. Ned Tisserat Bioagricultural Sciences and Pest Management Colorado State University Geosmithia is relatively easy to isolate from walnut cankers of all sizes. However, you need to make sure the submitter supplies you with the proper sample. Galleries and cankers are much more abundant in branches greater than 1 inch diameter and rarely occur in small diameter twigs at the ends of branches. Thus, the name walnut twig beetle is somewhat misleading in the case of black walnut. Samples should be collected from branches showing dieback or wilting. Although beetle galleries will be numerous in dead branches, the cankers will be difficult to delineate because the walnut bark oxidizes and turns brown at death. Cankers caused by Geosmithia usually are 3 – 6 inches in length and surround the beetle galleries. They rapidly coalesce to cause large irregular areas of phloem necrosis. The beetle galleries, and cankers often are more numerous on the bottom side of branches and the west side of the trunk. Young cankers may not extend all the way to the cambium, so be careful not to cut under the cankers and remove them. Eventually cankers will extend to the cambium. In all cases, the cankers will be covered by outer bark, even in advanced stages of the disease. Thus, you will not see the typical open-faced, target cankers we associate with diseases like butternut and Nectria canker. After selecting a sample, remove the outer bark. The bark surface may be disinfested with ethanol but this isn’t essential. -

Phylogenetic Position of Geosmithia Spp. (Hypocreales) Living in Juniperus Spp
Article Phylogenetic Position of Geosmithia spp. (Hypocreales) Living in Juniperus spp. Forests (Cupressaceae) with Bark Beetles of Phloeosinus spp. (Scolytinae) from the Northeast of Mexico Hernández-García Juan Alfredo 1,2,3 , Cuellar-Rodríguez Gerardo 1 , Aguirre-Ojeda Nallely Guadalupe 1, Villa-Tanaca Lourdes 2 , Hernández-Rodríguez César 2 and Armendáriz-Toledano Francisco 3,* 1 Departamento de Silvicultura, Facultad de Ciencias Forestales, Universidad Autónoma de Nuevo León, Carretera Nacional No. 85, Km. 145, Linares, Nuevo León C.P. 67700, Mexico; [email protected] (H.-G.J.A.); [email protected] (C.-R.G.); [email protected] (A.-O.N.G.) 2 Departamento de Microbiología, Escuela Nacional de Ciencias Biológicas, Instituto Politécnico Nacional, Ciudad de Mexico C.P. 11340, Mexico; [email protected] (V.-T.L.); [email protected] (H.-R.C.) 3 Colección Nacional de Insectos, Departamento de Zoología, Instituto de Biología, Universidad Nacional Autónoma de México, Cto. Zona Deportiva S/N, Ciudad Universitaria. CDMX, Mexico C.P. 04510, Mexico * Correspondence: [email protected]; Tel.: +55-56-22-92-50 (ext. 47833) Received: 11 September 2020; Accepted: 22 October 2020; Published: 28 October 2020 Abstract: Geosmithia members are mitosporic filamentous fungi commonly recorded and isolated from bark beetles of the Scolytinae subfamily and their respective host’s species. This genus includes 18 species formally described and 38 phylogenetic species recorded in several localities from Africa, Asia, Australia, Europe, and North and South America, where they exhibit frequent associations with phloeophagous and wood-boring bark beetles. Among phloephagous bark beetle species, specifically, in members of the genus Phloeosinus Chapuis, almost 10% of Geosmithia strains have been isolated. -

June 24, 2019 Detection of Geosmithia Morbida on Numerous
Plant Health Progress ¿ 2019 ¿ 00:1–7 https://doi.org/10.1094/PHP-02-19-0016-RS Research Detection of Geosmithia morbida on Numerous Insect Species in Q:1 Four Eastern States Melanie Moore,1,† Jennifer Juzwik,1 Fredric Miller,2 Leah Roberts,3 and Matthew D. Ginzel4 1 USDA Forest Service, Northern Research Station, St. Paul, MN 55108 2 Department of Horticulture, Joliet Junior College, Joliet, IL 60431 3 6209 Wynbrook Way, Raleigh, NC 27612 4 Department of Entomology, Purdue University, West Lafayette, IN 47907 Accepted for publication 30 May 2019. Abstract Thousand cankers disease is caused by the coalescence of nu- beetles, bark beetles, and other weevils was conducted in four merous Geosmithia morbida cankers on branches and stems of eastern states, and captured beetles were assayed to detect G. Juglans species, leading to branch dieback and eventual tree morbida using both culture and PCR-based methods. A new death. The fungus sporulates in galleries of the walnut twig beetle primer pair (GmF3/GmR13), based on the b-tubulin region, was (Pityophthorus juglandis), allowing for acquisition of pathogen designed for G. morbida DNA detection. The pathogen was de- propagules and its subsequent transmission to other branches or tected on 18 insect species using molecular methods, and live trees following adult emergence. Recently, G. morbida has been cultures were isolated from two species. This is the first report of isolated from Xylosandrus crassiusculus and Xyleborinus saxesenii the pathogen in Illinois and Minnesota. collected in Ohio and Stenomimus pallidus collected in Indiana. These beetles are known to colonize diseased Juglans nigra in Keywords: diagnostics, trees, thousand cankers disease, Juglans, Q:2 these states. -

(Ulmus Minor) in Geneva, Switzerland
Folia Forestalia Polonica, Series A – Forestry, 2016, Vol. 58 (2), 96–102 SHORT COMMUNICATION DOI: 10.1515/ffp-2016-0011 First report of Geosmithia langdonii and Geosmithia spp. isolated from a decaying elm (Ulmus minor) in Geneva, Switzerland Martine Hänzi, Bastien Cochard, Romain Chablais, Julien Crovadore, François Lefort University of Applied Sciences and Arts Western Switzerland, Geneva Institute for Technology Architecture and Landscape, Institute Land Nature and Environment, Plants and Pathogens Group, 50 route de Presinge, 1254 Jussy, Switzerland, e-mail: [email protected] ABSTRACT The mortality of a young elm Ulmus minor in 2014 in Geneva prompted a search for the microorganisms potentially involved. Symptoms included foliar chlorosis and wilting followed by defoliation of branches. Wood symptoms included a brown streaking of sap wood and brown stains in trunk and branches. The comparison of the resulting ITS rDNA sequences to the NCBI Nucleotide database allowed to identify 10 different organisms. The genus Geo smithia represented 48% of the isolates belonging to three species: Geosmithia langdonii (7 isolates) and 2 unknown morphologically and genetically different Geosmithia sp. 1 and sp. 2 (4 isolates). Geosmithia species are very little known ascomycetes, which have been recently shown to be opportunistic pathogens on broadleaved trees and coni- fers, living as saprobes in galleries of many bark beetle species. In the case described here, Geosmithia langdonii, and the unknown Geosmithia species were found in symptomatic wood while bark beetle galleries were found in close regions of the symptomatic wood. Geosmithia langdonii was the major fungus retrieved from the symptomatic wood and could have contributed, along with other identified fungal species, to a pathogenic complex producing symptoms similar to the ones of the Dutch Elm Disease and led to the dieback of this elm tree. -

Phylogeny and Nomenclature of the Genus Talaromyces and Taxa Accommodated in Penicillium Subgenus Biverticillium
available online at www.studiesinmycology.org StudieS in Mycology 70: 159–183. 2011. doi:10.3114/sim.2011.70.04 Phylogeny and nomenclature of the genus Talaromyces and taxa accommodated in Penicillium subgenus Biverticillium R.A. Samson1, N. Yilmaz1,6, J. Houbraken1,6, H. Spierenburg1, K.A. Seifert2, S.W. Peterson3, J. Varga4 and J.C. Frisvad5 1CBS-KNAW Fungal Biodiversity Centre, Uppsalalaan 8, 3584 CT Utrecht, The Netherlands; 2Biodiversity (Mycology), Eastern Cereal and Oilseed Research Centre, Agriculture & Agri-Food Canada, 960 Carling Ave., Ottawa, Ontario, K1A 0C6, Canada, 3Bacterial Foodborne Pathogens and Mycology Research Unit, National Center for Agricultural Utilization Research, 1815 N. University Street, Peoria, IL 61604, U.S.A., 4Department of Microbiology, Faculty of Science and Informatics, University of Szeged, H-6726 Szeged, Közép fasor 52, Hungary, 5Department of Systems Biology, Building 221, Technical University of Denmark, DK-2800, Kgs. Lyngby, Denmark; 6Microbiology, Department of Biology, Utrecht University, Padualaan 8, 3584 CH Utrecht, The Netherlands. *Correspondence: R.A. Samson, [email protected] Abstract: The taxonomic history of anamorphic species attributed to Penicillium subgenus Biverticillium is reviewed, along with evidence supporting their relationship with teleomorphic species classified inTalaromyces. To supplement previous conclusions based on ITS, SSU and/or LSU sequencing that Talaromyces and subgenus Biverticillium comprise a monophyletic group that is distinct from Penicillium at the generic level, the phylogenetic relationships of these two groups with other genera of Trichocomaceae was further studied by sequencing a part of the RPB1 (RNA polymerase II largest subunit) gene. Talaromyces species and most species of Penicillium subgenus Biverticillium sensu Pitt reside in a monophyletic clade distant from species of other subgenera of Penicillium. -

Thousand Cankers Disease of Walnut (Geosmithia Morbida)
Published by Utah State University Extension and Utah Plant Pest Diagnostic Laboratory PLP-015pr August 2011 Thousand Cankers Disease of Walnut (Geosmithia morbida) Claudia Nischwitz, Extension Plant Pathologist • Marion Murray, IPM Project Leader What you should know • Thousand cankers disease is caused by the fungus Geosmithia morbida. • It is transmitted by the walnut twig beetle (Pityoph- thorus juglandis). • Once symptoms are visible, trees can die within 2 to 3 years. INTRODUCTION Thousand cankers is a newly recognized disease of walnuts, caused by a fungus (Geosmithia morbida) Fig. 1. Walnut twig beetle (Pityophthorus juglandis)1 that is spread by the walnut twig beetle (Pityophthorus juglandis, Fig. 1). The beetle is endemic to the native range of Arizona walnut (Arizona, New Mexico, and Chihuahua, Mexico), and was first identified in Utah in 1988. Widespread mortality of black walnut in the early 2000s in Colorado and Utah led to the discovery of the pathogen-vector complex. The name of the disease comes from the numerous necrotic lesions (cankers, Figs. 4a and b) found on the cambium of infected trees (Tisserat et al. 2009). The fungus kills black walnut trees (Fig. 2) often within 3 years of the development of the first symptoms (Cranshaw and Tisserat 2008). HOSTS Fig. 2. 400-year old black walnut killed in northern Utah Black walnut (Juglans nigra) and black walnut hybrids are very susceptible to Geosmithia. California walnuts (J. hindsii, J. californica) and Persian walnuts (J. regia) are slightly susceptible. Cankers do not seem to form on Arizona walnuts (J. major) (Cranshaw and Tisserat 2008). SYMPTOMS It may take several years of insect and fungal attack before symptoms are visible, starting with yellowing leaves and thinning tree crown. -
Pest Alert – Walnut Twig Beetle And
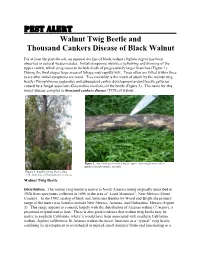
Pest Alert Walnut Twig Beetle and Thousand Cankers Disease of Black Walnut For at least the past decade, an unusual decline of black walnut (Juglans nigra) has been observed in several western states. Initial symptoms involve a yellowing and thinning of the upper crown, which progresses to include death of progressively larger branches (Figure 1). During the final stages large areas of foliage may rapidly wilt. Trees often are killed within three years after initial symptoms are noted. Tree mortality is the result of attack by the walnut twig beetle (Pityophthorus juglandis) and subsequent canker development around beetle galleries caused by a fungal associate (Geosmithia morbida) of the beetle (Figure 2). The name for this insect-disease complex is thousand cankers disease (TCD) of walnut. Figure 2. Outer bark peeled from a log to expose coalescing branch cankers produced by Geosmithia morbida. Figure 1. Rapidly wilting black walnut in the final stage of thousand cankers disease. Walnut Twig Beetle Distribution. The walnut twig beetle is native to North America being originally described in 1928 from specimens collected in 1896 in the area of “Lone Mountain”, New Mexico (Grant County). In the 1992 catalog of Bark and Ambrosia Beetles by Wood and Bright the primary range of the insect was listed to include New Mexico, Arizona, and Chihuahua, Mexico (Figure 3). This range appears to coincide largely with the distribution of Arizona walnut (J. major), a presumed original native host. There is also good evidence that walnut twig beetle may be native to southern California, where it would have been associated with southern California walnut, Juglans californica. -

Thousand Cankers Disease: Virulence of Geosmithia Morbida Isolates and Potential Alternative Vectors of the Fungus
University of Tennessee, Knoxville TRACE: Tennessee Research and Creative Exchange Masters Theses Graduate School 5-2018 Thousand Cankers Disease: Virulence of Geosmithia morbida isolates and potential alternative vectors of the fungus Karandeep Singh Chahal University of Tennessee, [email protected] Follow this and additional works at: https://trace.tennessee.edu/utk_gradthes Recommended Citation Chahal, Karandeep Singh, "Thousand Cankers Disease: Virulence of Geosmithia morbida isolates and potential alternative vectors of the fungus. " Master's Thesis, University of Tennessee, 2018. https://trace.tennessee.edu/utk_gradthes/5065 This Thesis is brought to you for free and open access by the Graduate School at TRACE: Tennessee Research and Creative Exchange. It has been accepted for inclusion in Masters Theses by an authorized administrator of TRACE: Tennessee Research and Creative Exchange. For more information, please contact [email protected]. To the Graduate Council: I am submitting herewith a thesis written by Karandeep Singh Chahal entitled "Thousand Cankers Disease: Virulence of Geosmithia morbida isolates and potential alternative vectors of the fungus." I have examined the final electronic copy of this thesis for form and content and recommend that it be accepted in partial fulfillment of the equirr ements for the degree of Master of Science, with a major in Entomology and Plant Pathology. Mark T. Windham, Major Professor We have read this thesis and recommend its acceptance: Jerome F. Grant, Denita Hadziabdic, William E. Klingeman -

Mini Data Sheet on Geosmithia Morbida and Pityophthorus Juglandis
EPPO, 2015 Mini data sheet on Thousand cankers disease (Geosmithia morbida and Pityophthorus juglandis) Geosmithia morbida and Pityophthorus juglandis were added to the EPPO A2 List in 2015. A full datasheet will be prepared, in the meantime you can view here the data which was previously available from the EPPO Alert List (added to the EPPO Alert List in 2014-deleted in 2015). Thousand cankers disease (Geosmithia morbida and Pityophthorus juglandis) Why: In the USA, widespread branch dieback and mortality of Juglans nigra (black walnut) has been occurring since the mid-1990s. In 2008, this mortality was determined to be the result of a combination of feeding damage by Pityophthorus juglandis (Coleoptera: Scolytidae - walnut twig beetle), and subsequent canker development around beetle galleries caused by a newly described fungal symbiont of the beetle, Geosmithia morbida. As the number of cankers formed on branches and trunks is very high, the disease has been called thousand cankers. In the USA, this disease is now widespread in the Western states causing extensive tree mortality on J. nigra (and to a lesser extent on some other Juglans species), and has also established in several states in the Eastern part of the USA where J. nigra is a native species. At the end of 2013, thousand cankers disease was reported for the first time in Italy on a small number of J. nigra trees. Considering the risk that this disease may present for walnut trees (Juglans spp.) which are widely grown in the EPPO region, the Secretariat decided to add G. morbida and its vector, P. -

Geosmithia Xerotolerans Fungal Planet Description Sheets 369
368 Persoonia – Volume 41, 2018 Geosmithia xerotolerans Fungal Planet description sheets 369 Fungal Planet 845 – 13 December 2018 Geosmithia xerotolerans Rodr.-Andrade, Cano & Stchigel, sp. nov. Etymology. From Greek ξερός-, dry, and Latin -tolerans, tolerance, due 50 % (glucose 50 % / fructose 50 %), 23–24 mm diam, 18–19 to the ability of this fungus to grow on culture media with a low water activity. mm diam and 12–13 mm diam, respectively). In these culture Classification — Incertae sedis, Hypocreales, Sordariomy media the fungal sporulation is abundant. Minimum, optimal cetes. and maximum temperature of growth: 15 °C, 25 °C and 35 °C, respectively. Mycelium composed of hyaline, septate, funiculose hyphae, Typus. SPAIN, Tarragona province, Els Pallaresos, isolated from a dark- 2–3 μm wide. Conidiophores borne on vegetative mycelium, de - ened wall of a house, 19 Apr. 2018, J. Cano & A.M. Stchigel (holotype CBS terminate, erect, septate, penicillate, bi- to terverticillate, mostly H-23734, cultures ex-type FMR 17085 = CBS 144969; BenA, EF1-α, ITS and solitary, sometimes funiculose; stipes hyaline, 25–155 × 2–3 LSU sequences GenBank LS998791, LS998792, LS998789 and LS998790; μm, septate, smooth-walled to verrucose, asymmetrically MycoBank MB827825). branched; primary branch (= rami) cylindrical, 20–40 × 2–3 μm, mostly septate, smooth-walled to verrucose; terminal Notes — Geosmithia xerotolerans was recovered from the branch (= metulae) cylindrical, 7–15 × 2 μm, rarely 1-septate, surface of a darkened house wall taken in Els Pallaresos, Tar- with smooth to verrucose walls, in whorls of 2–3; phialides cy- ragona province, Spain. The genus Geosmithia was erected lindrical, 8–10 × 1.5–2 μm, abruptly tapering at the apex, with to accommodate species previously placed in Penicillium, with smooth to verrucose walls, in whorls of 2–5.