City and County of Honolulu
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

City Council
COMMITTEE ON ZONING AND PLANNING CITY COUNCIL Voting Members: CITY AND COUNTY OF HONOLULU Brandon J.C Elefante, Chair HONOLULU, HAWAII 96813 - 3 0 7 7 Esther Kia‘āina, Vice Chair Radiant Cordero Calvin K.Y. Say AGENDA REGULAR MEETING CITY COUNCIL CHAMBER THURSDAY, MAY 20, 2021 9:00 A.M. PUBLIC PARTICIPATION AND TESTIMONY Pursuant to the Nineteenth Proclamation issued by Governor David Ige on April 9, 2021, relating to the COVID-19 pandemic, in order to allow public participation in a manner consistent with social distancing practices the following procedures are in effect for the meeting: VIEWING THE MEETING AND RESTRICTIONS ON ENTRY Members of the public will not be allowed into the meeting room, but may view the meeting on a live broadcast. The meeting will be viewable: (1) by internet live streaming through www.honolulucitycouncil.com and (2) by televised live broadcast on Olelo TV Channel 54. After the meeting, the meeting will be viewable on demand at http://www.honolulucitycouncil.tv/. Copies of older meeting videos may be requested by calling the City Clerk’s Office at 768-5822; charges may apply. Some Councilmembers and presenters may be participating in the meeting by interactive conference technology from remote locations. ORAL TESTIMONY Oral testimony will be permitted on all items on the agenda, subject to the following restrictions: 1. Persons may submit oral testimony remotely through the Webex video conferencing platform. To participate, persons should visit www.webex.com, click “Join,” enter meeting number 187 251 3691 and complete the registration process. Registrants will receive an email that contains links and information on joining the meeting by either phone or video conference. -

Hawaiian Historical Society
UNIVERSITY OF HAWAII LIBRARY PAPERS OF THE HAWAIIAN HISTORICAL SOCIETY NUMBER 17 PAPERS READ BEFORE THE SOCIETY SEPTEMBER 30, 1930 PAPERS OF THE HAWAIIAN HISTORICAL SOCIETY NUMBER 17 PAPERS READ BEFORE THE SOCIETY , SEPTEMBER 30, 1930 Printed by The Printshop Co., Ltd. 1930 CONTENTS Page Proceedings of the Hawaiian Historical Society Meeting, September 30, 1930 _.. 5 Historical Notes- 7 By Albert Pierce Taylor, Secretary Reminiscences of the Court of Kamehameha IV and Queen Emma 17 By Col. Curtis Piehu Iaukea former Chamberlain to King Kalakaua The Adoption of the Hawaiian Alphabet 28 By Col. Thomas Marshall Spaulding, U.S.A. The Burial Caves- of Pahukaina 34 By Emma Ahuena Davis on Taylor Annexation Scheme of 1854 That Failed: Chapter Eighteen —Life of Admiral Theodoras Bailey, U.S.N ,.. 39 By Francis R. Stoddard «f (Read by Albert Pierce Taylor) - • . • Kauai Archeology 53 By Wendell C. Bennett Read before Kauai Historical Society, May 20, 1929 Burial of King Keawe '.. 63 By John P. G. Stokes PROCEEDINGS OF THE HAWAIIAN HISTORICAL SOCIETY MEETING SEPTEMBER 30, 1930 Meeting of the Society was called for this date, at 7:30 P. M., in the Library of Hawaii, to hear several Papers which were prepared by members on varied historical phases relating to the Hawaiian Islands. Bishop H. B. Restarick, president, in the chair; A. P. Taylor, secretary and several of the trustees, more members than usual in attendance, and many visitors present, the assembly room being filled to capacity. Bishop Restarick announced that the names of Harold W. Bradley, of Pomona, Calif., engaged in historical research in Honolulu until recently, and Bishop S. -

Kamehameha Highway North Scale: 1"=40'
STATE COUNTY ROW ROW STOP PRIVATE ROAD END CITY AND COUNTY HIGHWAY STOP MATCH LINE A KAMEHAMEHA HIGHWAY NORTH SCALE: 1"=40' LIHIKAI DR KAMEHAMEHA HWY STOP 25 M. P. H. PARKING ANY TIME MATCH LINE A MATCH LINE B GRAPHIC SCALE PARKING 40 0 40 80 ANY TIME SCALE IN FEET 25 REVISION DATE BRIEF DESCRIPTION BY APPROVED M. P. H. DEPARTMENT OF TRANSPORTATION SERVICES PARKING CITY AND COUNTY OF HONOLULU ANY TIME 25 M. P. H. COMPLETE STREETS PLANNING REHABILITATION OF STREETS UNITS 73A, 73B, AND 73C OAHU, HAWAII Expiration Date: 4/30/20 KAMEHAMEHA HIGHWAY - 1 THIS WORK WAS PREPARED BY ME OR UNDER MY SUPERVISION AND CONSTRUCTION OF THIS PROJECT WILL ENGINEER: LN/JS DATE: October 2019 BE UNDER MY OBSERVATION. DRAFTSMAN: - SCALE: AS NOTED KAMEHAMEHA HIGHWAY CHK BY: LN REF: - NORTH SCALE: 1"=40' C-003 BELT COLLINS HAWAII, LLC Thu, 10 Sep 2020 - 8:50am M:\DTS Complete Streets\2017710300\04 Graphics\CAD\Sheets - Kaneohe\C-003 KAMEHAMEHA HIGHWAY Kahekili Hwy to Kaneohe Bay 1.dwg SHEET 3 OF 000 SHEETS FILE POCKET FOLDER NO. DR HWY LAENANI KAMEHAMEHA STOP MATCH LINE B MATCH LINE C SPEED HUMP PARKING PARKING ANY AHEAD TIME ANY TIME SPEED SPEED LIMIT HUMP 30 AHEAD SPEED HUMP KAMEHAMEHA HIGHWAY NORTH SCALE: 1"=40' GRAPHIC SCALE 40 0 40 80 SCALE IN FEET MATCH LINE C MATCH LINE D 25 REVISION DATE BRIEF DESCRIPTION BY APPROVED M. P. H. DEPARTMENT OF TRANSPORTATION SERVICES CITY AND COUNTY OF HONOLULU COMPLETE STREETS PLANNING REHABILITATION OF STREETS UNITS 73A, 73B, AND 73C OAHU, HAWAII Expiration Date: 4/30/20 KAMEHAMEHA HIGHWAY - 2 THIS WORK WAS PREPARED BY ME OR UNDER MY SUPERVISION AND CONSTRUCTION OF THIS PROJECT WILL ENGINEER: LN/JS DATE: October 2019 BE UNDER MY OBSERVATION. -

KALAUAO STREAM BRIDGE HAER No. HI-117
KALAUAO STREAM BRIDGE HAER No. HI-117 (Kalauao Stream Eastbound Bridge & Kalauao Stream Westbound Bridge) Kamehameha Highway and Kalauao Stream Aiea Honolulu County Hawaii PHOTOGRAPHS WRITTEN HISTORICAL AND DESCRIPTIVE DATA HISTORIC AMERICAN ENGINEERING RECORD U.S. Department of the Interior National Park Service Oakland, California HISTORIC AMERICAN ENGINEERING RECORD KALAUAO STREAM BRIDGE (Kalauao Stream Eastbound Bridge & Kalauao Stream Westbound Bridge) HAER No. HI-117 Location: Kamehameha Highway and Kalauao Stream Aiea City and County of Honolulu, Hawaii U.S.G.S. Topographic map, Waipahu Quadrangle 1998 (7.5 minute series) Universal Transverse Mercator Coordinates NAD 83: 04.609850.2364650 Present Owner: State of Hawaii Present Use: Vehicular Bridge Significance: The Kalauao Stream Bridge is a significant resource in the history of Oahu's road transportation system. It is significant at the local level for its association with the development of this section of Kamehameha Highway, and the adjacent Aiea and Pearl City settlements, which grew into suburbs from their initial establishment as a sugarcane plantation and a train-stop “city,” respectively. Historian: Dee Ruzicka Mason Architects, Inc. 119 Merchant Street Suite 501 Honolulu, HI 96813 Project Information: This report is part of the documentation for properties identified as adversely affected by the Honolulu Rail Transit Project (HRTP) in the City and County of Honolulu. This documentation was required under Stipulation V.C. (1, 2) of the Honolulu High-Capacity Transit Corridor Project (HHCTCP) Programmatic Agreement (PA), which was signed by the U.S. Department of Transportation’s Federal Transit Administration, the Hawaii State Historic Preservation Officer, the United States Navy, and the Advisory Council on Historic Preservation. -

The Ethics Commission Meeting
8/10/2018 WELCOME TO THE ETHICS COMMISSION MEETING Please sign in at the testimony table. As a courtesy, please silence your cell phone. Date: August15,2018 Time: 11:30a.m. Place: Kapālama Hale 925 Dillingham Boulevard 1st Floor Conference Room 1 ORDER OF BUSINESS I. Call to Order, Public Notice, Quorum Honolulu Ethics Commission “We Hold the Public’s Trust” 2 1 8/10/2018 II. NEW BUSINESS A. Chair’s Report 1. Announcements, Introductions, Correspondence, and Additional Distribution Honolulu Ethics Commission “We Hold the Public’s Trust” 3 II.A. CHAIR’S REPORT (cont’d) 2. For Action: Approval of Open Session Minutes of July 18, 2018 3. For Action: Approval of Executive Session Minutes of July 18, 2018 [exec/session if needed, HRS §92-5(a)(4)] Honolulu Ethics Commission “We Hold the Public’s Trust” 4 2 8/10/2018 II.B. EXECUTIVE DIRECTOR AND LEGAL COUNSEL’S (EDLC) REPORT 1. Staff Work Reports Summary . Sr. Clerk . Legal Clerk III (TA) . Investigator . Associate Legal Counsel Honolulu Ethics Commission “We Hold the Public’s Trust” 5 II.B.1. STAFF WORK REPORTS – HIGHLIGHTS SENIOR CLERK . Assisting with EC meeting administration, uploading docs to website . Compiled data for FY18 reporting . Processing lobbyist forms . Assisting with legal clerk functions, attending staff and other meetings Honolulu Ethics Commission “We Hold the Public’s Trust” 6 3 8/10/2018 II.B.1. STAFF WORK REPORTS – HIGHLIGHTS LEGAL CLERK III (TA) . Finalizing all-City ethics training (FY16–FY18) . Processing meeting minutes/materials, case intake, UIPA log . Assisting investigations, drafting correspondence; compiling data for FY18 statistics . -

Ad E& MAY 2 6 1967
FEBRUARY, 1966 254 &Ad e& MAY 2 6 1967 Amstrong, Richard,presents census report 145; Minister of Public Abbott, Dr. Agatin 173 Instruction 22k; 227, 233, 235, 236, Abortion 205 23 7 About A Remarkable Stranger, Story 7 Arnlstrong, Mrs. Richard 227 Adms, Capt . Alexander, loyal supporter Armstrong, Sam, son of Richard 224 of Kamehameha I 95; 96, 136 Ashford, Volney ,threatens Kalakaua 44 Adans, E.P., auctioneer 84 Ashford and Ashford 26 Adams, Romanzo, 59, 62, 110, 111, ll3, Asiatic cholera 113 Ilk, 144, 146, 148, 149, 204, 26 ---Askold, Russian corvette 105, 109 Adams Gardens 95 Astor, John Jacob 194, 195 Adams Lane 95 Astoria, fur trading post 195, 196 Adobe, use of 130 Atherton, F.C, 142 ---mc-Advertiser 84, 85 Attorney General file 38 Agriculture, Dept. of 61 Auction of Court House on Queen Street kguiar, Ernest Fa 156 85 Aiu, Maiki 173 Auhea, Chiefess-Premier 132, 133 illmeda, Mrs. Frank 169, 172 Auld, Andrew 223 Alapai-nui, Chief of Hawaii 126 Austin, James We 29 klapai Street 233 Automobile, first in islands 47 Alapa Regiment 171 ---Albert, barkentine 211 kle,xander, Xary 7 Alexander, W.D., disputes Adams 1 claim Bailey, Edward 169; oil paintings by 2s originator of flag 96 170: 171 Alexander, Rev. W.P., estimates birth mile: House, Wailuku 169, 170, 171 and death rates 110; 203 Bailey paintings 170, 171 Alexander Liholiho SEE: Kamehameha IV Baker, Ray Jerome ,photographer 80, 87, 7 rn Aliiolani Hale 1, 41 opens 84 1 (J- Allen, E.H., U.S. Consul 223, 228 Baker, T.J. -
State of Hawaii Projects
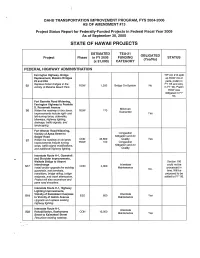
OAHU TRANSPORTATION IMPROVEMENT PROGRAM, FYS 2004-2006 AS OF AMENDMENT #13 Project Status Report for Federally-Funded Projects in Federal Fiscal Year 2005 As of September 30, 2005 STATE OF HAWAII PROJECTS ESTIMATED TEA-21 OBLIGATED Project Phase in FY 2005 FUNDING STATUS (Yes/No) (x $1,000) CATEGORY FEDERAL HIGHWAY ADMINISTRATION Farrington Highway, Bridge Tl P Am #13 split Replacement, Makaha Bridges up ROW into2 #3 and #3A parts, prelim in Replace timber bridges in the FY '05 and Acq. 52 ROW 1,300 Bridge On-System No vicinity of Makaha Beach Park. in FY '06. Prelim ROW was obligated in FY '04. Fort Barrette Road Widening, Farrington Highway to Franklin D. Roosevelt Avenue Minimum S6 Widen the roadway to four lanes. ROW 170 Guarantee Improvements include right- and Yes lefHuming lanes, sidewalks, bikeways, highway lighting, drainage, traffic signals, and landscaping. Fort Weaver Road Widening, Vicinity of Aawa Street to Congestion Geiger Road Mitigation and Air CON 45,800 Quality Yes S7 Widen the roadway to six lanes. Improvements include turning ROW 100 Congestion lanes, traffic signal modifications, Mitigation and Air and additional highway lighting. Quality Interstate Route HM1, Guardrail and Shoulder Improvements, Waikele Bridge to Airport Section 106 Interchange Interstate could not be S17 CON 4,300 Install and/or upgrade the existing Maintenance processed in No. guardrails, end terminals, time. Will be transitions, bridge railing, bridge proposed to be endposts, and crash attenuators, added to FY '06. Project will also reconstruct and pave road shoulders. Interstate Route H~1, Highway Lighting Improvements, Vicinity of Kaimakani Overpass Interstate S18 ESD 600 Yes to Vicinity of Gulick Avenue Maintenance Upgrade and replace existing highway lighting. -

Night Drop Savings Bank
Night Drop Savings Bank Oahu Ala Moana Center Branch Kaneohe Branch Town Center of Mililani Branch UH Campus Branch 1450 Ala Moana Boulevard 45-1144 Kamehameha Highway 95-1249 Meheula Parkway Hemenway Hall Suite 1255 Suite 100 Suite 126 2445 Campus Road Honolulu, HI 96814-4613 Kaneohe, HI 96744-3272 Mililani, HI 96789-1787 Honolulu, HI 96822-2216 (808) 973-4864 (808) 233-4570 (808) 623-2878 (808) 973-6211 Ewa Branch Kapiolani Branch Nanakuli Wahiawa Branch Laulani Village Shopping Center 1600 Kapiolani Boulevard Sack N Save Branch 649 California Avenue 91-1101 Keaunui Drive Suite 205 87-2070 Farrington Highway Wahiawa, HI 96786-1941 Ewa Beach, HI 96706-6340 Honolulu, HI 96814-3897 Suite G (808) 622-4179 (808) 685-4618 (808) 946-2802 Waianae, HI 96792-3733 (808) 673-6600 Waianae Branch Haleiwa Branch Kapolei Branch Waianae Mall Haleiwa Shopping Plaza 888 Wakea Street Pearl City Branch 86-120 Farrington Highway 66-197 Kamehameha Highway Kapolei, HI 96707 Pearl City Shopping Center Building 1 Suite A (808) 674-2288 850 Kamehameha Highway Waianae, HI 96792-3065 Haleiwa, HI 96712-1400 Suite 164 (808) 673-2606 (808) 637-5042 Main Branch Pearl City, HI 96782-2657 1001 Bishop Street (808) 455-4138 Waikiki Branch Hawaii Kai Branch Honolulu, HI 96813-3400 Waikiki Trade Center Hawaii Kai Towne Center (808) 523-6844 Pearlridge Branch 2255 Kuhio Avenue 333 Keahole Street 98-200 Kamehameha Highway Suite 105 Honolulu, HI 96825-3406 Makiki Branch 1st Floor Honolulu, HI 96815-2681 (808) 395-2308 1209 Piikoi Street Aiea, HI 96701-4395 (808) 923-1102 Honolulu, -

1856 1877 1881 1888 1894 1900 1918 1932 Box 1-1 JOHANN FRIEDRICH HACKFELD
M-307 JOHANNFRIEDRICH HACKFELD (1856- 1932) 1856 Bornin Germany; educated there and served in German Anny. 1877 Came to Hawaii, worked in uncle's business, H. Hackfeld & Company. 1881 Became partnerin company, alongwith Paul Isenberg andH. F. Glade. 1888 Visited in Germany; marriedJulia Berkenbusch; returnedto Hawaii. 1894 H.F. Glade leftcompany; J. F. Hackfeld and Paul Isenberg became sole ownersofH. Hackfeld& Company. 1900 Moved to Germany tolive due to Mrs. Hackfeld's health. Thereafter divided his time betweenGermany and Hawaii. After 1914, he visited Honolulu only threeor fourtimes. 1918 Assets and properties ofH. Hackfeld & Company seized by U.S. Governmentunder Alien PropertyAct. Varioussuits brought againstU. S. Governmentfor restitution. 1932 August 27, J. F. Hackfeld died, Bremen, Germany. Box 1-1 United States AttorneyGeneral Opinion No. 67, February 17, 1941. Executors ofJ. F. Hackfeld'sestate brought suit against the U. S. Governmentfor larger payment than was originallyallowed in restitution forHawaiian sugar properties expropriated in 1918 by Alien Property Act authority. This document is the opinion of Circuit Judge Swan in The U.S. Circuit Court of Appeals forthe Second Circuit, February 17, 1941. M-244 HAEHAW All (BARK) Box 1-1 Shipping articleson a whaling cruise, 1864 - 1865 Hawaiian shipping articles forBark Hae Hawaii, JohnHeppingstone, master, on a whaling cruise, December 19, 1864, until :the fall of 1865". M-305 HAIKUFRUIT AND PACKlNGCOMP ANY 1903 Haiku Fruitand Packing Company incorporated. 1904 Canneryand can making plant installed; initial pack was 1,400 cases. 1911 Bought out Pukalani Dairy and Pineapple Co (founded1907 at Pauwela) 1912 Hawaiian Pineapple Company bought controlof Haiku F & P Company 1918 Controlof Haiku F & P Company bought fromHawaiian Pineapple Company by hui of Maui men, headed by H. -

(HU) January 19, 2009 Interviewer: Brian Niiya
JAPANESE CULTURAL CENTER OF HAWAI‘I ORAL HISTORY INTERVIEW with HARRY URATA (HU) January 19, 2009 Interviewer: Brian Niiya (BN) Notes: Double parentheses ((?)) denote unclear sentences or words. Notes in brackets [ ] are added by the translator for clarification purposes. BN: We’re here at the Japanese Cultural Center on January 19, 2009 with Mr. Harry Urata and we’re going to ask him a life history with him and I guess we’ll start maybe with your parents. Maybe you could tell me their names and what you know about where they were from and what led them to come to Hawaii as far as, based on what you know. HU: Can you speak louder? I have a hard time hearing now. BN: I wonder if you could tell us about your parents—their names and what you know about where they were from and why they came to Hawaii. HU: My father’s name is Fukutaro Urata. My mother and he got married in Kumamoto before they came to Hawaii. That was, I think, I don’t remember exactly when but then they settled in Kukui Street, where I live right now, and they started a vegetable store, small one, very small. Then I was born there but when I was two years old, my father had an accident, car accident, at Nuuanu Pali. I think he was the first victim of Japanese immigrants with a car accident so came out in a big write-up in Hawaii Hochi and Nippu Jiji. I still have the Nippu Jiji one. -

Evolutions of "Paradise": Japanese Tourist Discourse About Hawaii
Evolutions of "Paradise": Japanese Tourist Discourse about Hawaii Yujin Yaguchi and Mari Yoshihara I in the summer of 1963, the popular Japanese actor Yuzo Kayama starred in a film called Hawai no Waka Daisho (translated as A Young Guy in Hawaii by the distributor).1 The film is set in Hawai'i, a paradise-like vacation land that many Japanese long to visit.2 Waka Daisho [Young Guy], a handsome college student played by Kayama, visits Hawai'i on behalf of a wealthy Japanese businessman whose spoiled son has turned into a "beachboy" in Hawaii.3 Waka Daisho manages to find the son, but he also accidentally meets an acquaintance, Sumiko, a beautiful young woman sent by a Japanese cosmetic company to help establish a branch in Honolulu. The two become close friends, and in one scene, they stroll on the beach together, Waka Daisho sings with an 'ukulele, and the sun sets beautifully in the Pacific Ocean. The film, the first of the extremely popular "Waka Daisho" film series to be shot abroad, portrayed many of the iconic images of Hawai'i for the Japanese audience. In the narrative and filmic construction, Hawai'i serves as the setting where beautiful women await the young, clean-cut hero who accomplishes his mission of finding a "lost" son, refines his skill as a sailor, and, through integrity and honesty, is united with the heroine. The popular icons of Hawai'i—clear sky, blue ocean, yachts, surfing, palm trees, lei, 'ukulele, hula, and Hawaiian 0026-3079/2004/4503-081 $2.50/0 American Studies, 45:3 (Fall 2004): 81-106 81 82 Yujin Yaguchi and MariYoshihara melodies—all provide a setting for the narrative in ways that the Japanese audience could recognize. -

Center for Hawaiian Sovereignty Studies 46-255 Kahuhipa St. Suite 1205 Kane'ohe, HI 96744 (808) 247-7942 Kenneth R
Center for Hawaiian Sovereignty Studies 46-255 Kahuhipa St. Suite 1205 Kane'ohe, HI 96744 (808) 247-7942 Kenneth R. Conklin, Ph.D. Executive Director e-mail [email protected] Unity, Equality, Aloha for all To: HOUSE COMMITTEE ON EDUCATION For hearing Thursday, March 18, 2021 Re: HCR179, HR148 URGING THE SUPERINTENDENT OF EDUCATION TO REQUEST THE BOARD OF EDUCATION TO CHANGE THE NAME OF PRESIDENT WILLIAM MCKINLEY HIGH SCHOOL BACK TO THE SCHOOL'S PREVIOUS NAME OF HONOLULU HIGH SCHOOL AND TO REMOVE THE STATUE OF PRESIDENT MCKINLEY FROM THE SCHOOL PREMISES TESTIMONY IN OPPOSITION There is only one reason why some activists want to abolish "McKinley" from the name of the school and remove his statue from the campus. The reason is, they want to rip the 50th star off the American flag and return Hawaii to its former status as an independent nation. And through this resolution they want to enlist you legislators as collaborators in their treasonous propaganda campaign. The strongest evidence that this is their motive is easy to see in the "whereas" clauses of this resolution and in documents provided by the NEA and the HSTA which are filled with historical falsehoods trashing the alleged U.S. "invasion" and "occupation" of Hawaii; alleged HCR179, HR148 Page !1 of !10 Conklin HSE EDN 031821 suppression of Hawaiian language and culture; and civics curriculum in the early Territorial period. Portraying Native Hawaiians as victims of colonial oppression and/or belligerent military occupation is designed to bolster demands to "give Hawaii back to the Hawaiians", thereby producing a race-supremacist government and turning the other 80% of Hawaii's people into second-class citizens.