S41231-020-00064-Z.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Supraventricular Tachycardia: from Fetus to Adult
Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across the Ages Narrow-complex Wide complex: VT Tachycardia HR >160: fetuses HR >220: infants HR >180: children HR >120: adults Above AV junction Types of SVT Re-entrant Automatic 1. Sudden onset and 1. Warms-up and cools offset down 2. Accessory pathway 2. Sensitive to 3. Terminates with catecholamines adenosine or 3. Does not respond to cardioversion either Most common: AVRT Most common: EAT Mechanism of SVT Re-entrant Automatic 90% <1% 10% AVN dependant AVN independant AVRT Atrial flutter AET AVNRT Atrial fib. CAR PJRT SNRT JET Mahaim Tachycardia IART 5 Re-entrant Automatic Fetal SVT Definition HR > 160 not associated with contraction or periodic decelerations Epidemiology Incidence ~1/1000 of all pregnancies Fetal arrhythmia: 1/3 of referrals to fetal echo lab CHD in 3% Copel et al., Am J Obstet Gynecol 2000 7 Clinical Approach to Fetal SVT 1. Define type SVT vs Flutter vs Fibrillation 2. Define absolute HR 3. Presence of CHD 4. Presence of hydrops 8 1. Type of SVT Best: 16-32 weeks Methods Phonocardiography Fetal echo Magnetocardiography (MCG) Fetal scalp electrode Fetal QRS Maternal QRS 9 Assessment of Rhythm by Fetal Echo Doppler SVC Aorta PAC Normal 10 Assessment of Rhythm by Fetal Echo M-Mode RV RA Atrium Rate~ 500 Ventricle Rate~240 11 2. Determine HR Atrial Rate Variability A:V Ventricular (bpm) Conduction Rate Normal 120-160 >10 bpm 1:1 120-160 Sinus 180-220 5-15 bpm 1:1 180-220 tachycardia SVT >220 No 1:1 >220 Atrial flutter 300-500 No 2-5:1 60-200 Atrial 300-500 Yes, due to 2-5:1 60-200 fibrillation variable AV conduction Bergmans et al., Obstet Gynecol Surv 1985 12 3. -

Thursday Poster Assignment
Corresponding Author Paper Title Board Assignment Number ‐ Thursday Classification of Typical Developing and Autism Spectrum Disorder Using Connectivity A.R., Jac Fredo Matrix and Support Vector Machine 111 Abbaszadeh, Behrooz Probabilistic Prediction of Epileptic Seizures Using SVM 220 Abe, Takuto Surrogate Modeling for Neuroprotective Focal Brain Cooling Device 110 Comprehensive Comparison of 2D vs. 3D Resource Usage in Large Volumetric Medical Agris, Jacob Image Segmentation 109 On Smartphone Sensability of Bi‐Phasic User Intoxication Levels from Diverse Walk Agu, Emmanuel Types in Standardized Field Sobriety Tests 327 The Effect of Perceived Sound Quality of Speech in Noisy Speech Perception by Akbarzadeh, Sara Normal Hearing and Hearing Impaired Listeners 370 Towards the Development of an Optrode Biopotential Sensor: Characterization Using Al Abed, Amr in Vitro Cardiac Tissue Recordings 108 Spatially Filtered Low‐Density EMG and Time‐Domain Descriptors Improves Hand Al‐Jumaily, Adel Movement Recognition 419 Optimizing Stimulation Strategies for Retinal Electrical Stimulation: A Modelling Study Alqahtani, Abdulrahman 287 An Automatic Navigation and Pressure Monitoring for Guided Insertion Procedure Alsunaydih, Fahad Nasser 326 A Statistical Determination of the Energy Delivered to Muscular Tissue in Amador, Alejandro Electrostimulation Protocols 149 Analysis of Muscle Fatigue During Exercise and Exercise Combined with Electrostimulation 151 Signal‐To‐Noise Ratio Determination in a Hybrid System of Electrostimulation and Electromiography 150 Continuous Prediction of Cognitive State Using a Marked‐Point Process Modeling Amidi, Yalda Framework 286 Antônio Freire Teixeira, Marcos Automatic Counting of Erythrocytes Using Image Processing 153 Feature Extraction from Radiographic Images for Bone Age Identification 152 Arantes, Ana Paula Bittar Britto Towards the Improvement of Algorithms Used in Robot‐Assisted Therapies 107 Arce‐Diego, José L. -

Transcatheter Ablation for the Treatment of Supraventricular Tachycardia in Adults
Medical Coverage Policy Effective Date ............................................. 4/15/2021 Next Review Date ....................................... 4/15/2022 Coverage Policy Number .................................. 0529 Transcatheter Ablation for the Treatment of Supraventricular Tachycardia in Adults Table of Contents Related Coverage Resources Overview .............................................................. 1 Cardiac Electrophysiological (EP) Studies Coverage Policy ................................................... 1 Nonpharmacological Treatments for Atrial Fibrillation General Background ............................................ 2 Medicare Coverage Determinations .................. 12 Coding/Billing Information .................................. 12 References ........................................................ 13 INSTRUCTIONS FOR USE The following Coverage Policy applies to health benefit plans administered by Cigna Companies. Certain Cigna Companies and/or lines of business only provide utilization review services to clients and do not make coverage determinations. References to standard benefit plan language and coverage determinations do not apply to those clients. Coverage Policies are intended to provide guidance in interpreting certain standard benefit plans administered by Cigna Companies. Please note, the terms of a customer’s particular benefit plan document [Group Service Agreement, Evidence of Coverage, Certificate of Coverage, Summary Plan Description (SPD) or similar plan document] may differ significantly -

Radiofrequency Ablation: Technique and Clinical Applications
Diagn Interv Radiol 2012; 18:508–516 INTERVENTIONAL RADIOLOGY © Turkish Society of Radiology 2012 REVIEW Radiofrequency ablation: technique and clinical applications Servet Tatlı, Ümit Tapan, Paul R. Morrison, Stuart G. Silverman ABSTRACT n last decade, there has been a rapid advancement in the utiliza- Radiofrequency ablation is the most commonly used percu- tion of percutaneous, image-guided tumor ablation methods. taneous ablation technique and well-documented in the lit- erature on focal therapies. It has become the image-guided I Radiofrequency (RF) ablation has become the method of choice be- ablation method of choice because of its efficacy, safety, and cause of its safety and efficacy. Image-guided RF ablation is minimally ease of use. Radiofrequency ablation has shown promise in treating selected solid tumors, particularly those involving the invasive and usually appropriate for inoperable patients with other co- liver, kidneys, lungs, and the musculoskeletal system. It is a morbidities. It requires a minimal hospital stay or can be performed on minimally invasive technique often used in inoperable patients an outpatient basis. It preserves more normal organ tissue and is less with other comorbidities. Radiofrequency ablation requires a minimal hospital stay or can be performed on an outpatient expensive than surgery (1–3). The procedures are generally performed by basis. The aim of this article is to review radiofrequency abla- using 14–21 G, partially insulated electrodes that are placed under guid- tion techniques and their clinical applications. ance (computed tomography [CT], magnetic resonance imaging [MRI], Key words: • radiofrequency catheter ablation • tumor or ultrasonography [US]) into the tumor to be ablated. -
Artificial Pneumothorax Improves Radiofrequency Ablation Of
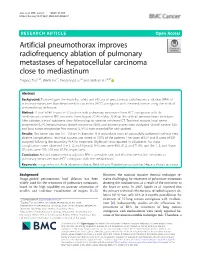
Zuo et al. BMC Cancer (2021) 21:505 https://doi.org/10.1186/s12885-021-08223-7 RESEARCH ARTICLE Open Access Artificial pneumothorax improves radiofrequency ablation of pulmonary metastases of hepatocellular carcinoma close to mediastinum Taiyang Zuo1,2†, Wenli Lin1†, Fengyong Liu1,2 and Jinshun Xu1,2,3* Abstract Background: To investigate the feasibility, safety and efficacy of percutaneous radiofrequency ablation (RFA) of pulmonary metastases from hepatocellular carcinoma (HCC) contiguous with the mediastinum using the artificial pneumothorax technique. Method: A total of 40 lesions in 32 patients with pulmonary metastases from HCC contiguous with the mediastinum accepted RFA treatment from August 2014 to May 2018 via the artificial pneumothorax technique. After ablation, clinical outcomes were followed up by contrast enhanced CT. Technical success, local tumor progression (LTP), intrapulmonary distant recurrence (IDR), and adverse events were evaluated. Overall survival (OS) and local tumor progression free survival (LTPFS) were recorded for each patient. Results: The tumor size was 1.4 ± 0.6 cm in diameter. RFA procedures were all successfully performed without intra- ablative complications. Technical success was noted in 100% of the patients. Five cases of LTP and 8 cases of IDR occurred following the secondary RFA for treatment. Slight pain was reported in all patients. No major complications were observed. The 1, 2, and 3-year LTPFS rates were 90.6, 81.2, and 71.8%, and the 1, 2, and 3-year OS rates were 100, 100 and 87.5%, respectively. Conclusion: Artificial pneumothorax adjuvant RFA is a feasible, safe, and efficient method for treatment of pulmonary metastases from HCC contiguous with the mediastinum. -

Radiofrequency Ablation for Spinal Pain
Radiofrequency Ablation for Spinal Pain Last Review Date: October 9, 2020 Number: MG.MM.ME.39cC2v2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth the clinical evidence that the patient meets the criteria for the treatment or surgical procedure. Without this documentation and information, EmblemHealth will not be able to properly review the request for prior authorization. The clinical review criteria expressed below reflects how EmblemHealth determines whether certain services or supplies are medically necessary. EmblemHealth established the clinical review criteria based upon a review of currently available clinical information (including clinical outcome studies in the peer-reviewed published medical literature, regulatory status of the technology, evidence-based guidelines of public health and health research agencies, evidence-based guidelines and positions of leading national health professional organizations, views of physicians practicing in relevant clinical areas, and other relevant factors). EmblemHealth expressly reserves the right to revise these conclusions as clinical information changes, and welcomes further relevant information. Each benefit program defines which services are covered. The conclusion that a particular service or supply is medically necessary does not constitute a representation or warranty that this service or supply is covered and/or paid for by EmblemHealth, as some programs exclude coverage for services or supplies that EmblemHealth considers medically necessary. If there is a discrepancy between this guideline and a member's benefits program, the benefits program will govern. In addition, coverage may be mandated by applicable legal requirements of a state, the Federal Government or the Centers for Medicare & Medicaid Services (CMS) for Medicare and Medicaid members. -

2019 HRS/EHRA/APHRS/LAHRS Expert Consensus Statement on Catheter Ablation of Ventricular Arrhythmias
2019 HRS/EHRA/APHRS/LAHRS expert consensus statement on catheter ablation of ventricular arrhythmias Edmond M. Cronin, MB, BCh, BAO, FHRS, CCDS, CEPS-A (Chair),1 Frank M. Bogun, MD (Vice-Chair),2 Philippe Maury, MD (EHRA Chair),3 Petr Peichl, MD, PhD (EHRA Vice-Chair),4 Minglong Chen, MD, PhD, FHRS (APHRS Chair),5 Narayanan Namboodiri, MBBS, MD (APHRS Vice-Chair),6 Luis Aguinaga, MD, PhD, FESC, FACC (LAHRS Chair),7 Luiz Roberto Leite, MD, PhD, FHRS (LAHRS Vice-Chair),8 Sana M. Al-Khatib, MD, MHS, FHRS, CCDS,9 Elad Anter, MD,10 Antonio Berruezo, MD, PhD,11,* David J. Callans, MD, FHRS, CCDS,12 Mina K. Chung, MD, FHRS,13,† Phillip Cuculich, MD,14 Andre d’Avila, MD, PhD,15,‡ Barbara J. Deal, MD, FACC,16,x Paolo Della Bella, MD,17,* Thomas Deneke, MD, PhD, FHRS,18,* Timm-Michael Dickfeld, MD, PhD, FACC, FHRS,19 Claudio Hadid, MD,20,{ Haris M. Haqqani, MBBS, PhD, FHRS,21,# G. Neal Kay, MD, CCDS,22 Rakesh Latchamsetty, MD, FHRS,2 Francis Marchlinski, MD, FHRS,12 John M. Miller, MD, FHRS,23,† Akihiko Nogami, MD, PhD,24,** Akash R. Patel, MD, FHRS, CEPS-P,25,†† Rajeev Kumar Pathak, MBBS, PhD, FHRS,26,# Luis C. Saenz Morales, MD,27,{ Pasquale Santangeli, MD, PhD,12 John L. Sapp, Jr., MD, FHRS,28 Andrea Sarkozy, MD, PhD, FEHRA,29,* Kyoko Soejima, MD,30,# William G. Stevenson, MD, FHRS,31 Usha B. Tedrow, MD, MS, FHRS,32 Wendy S. Tzou, MD, FHRS,33 Niraj Varma, MD, PhD,13 Katja Zeppenfeld, MD, PhD, FESC, FEHRA34,* Document Reviewers: Samuel J. -
Hip Joint Nerve Block/ Radiofrequency Ablation
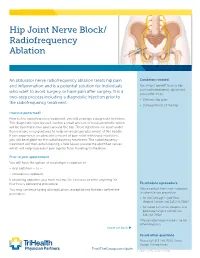
Hip/leg Hip Joint Nerve Block/ Radiofrequency Ablation 1 Piriformis Injection 3 Hip Joint Nerve Block/ Trochanteric Bursa Injection 5 Genicular Nerve Block/Radiofrequency Ablation 7 Radiofrequency Knee Viscosupplementation Injection 9 Ischial Bursa Injection 10 Ablation Lateral Femoral Cutaneous Nerve Block 12 Knee Joint Injection 14 Hip Joint Injection 16 An obturator nerve radiofrequency ablation treats hip pain Conditions treated and inflammation and is a potential solution for individuals You might benefit from a hip who want to avoid surgery or have pain after surgery. It is a joint radiofrequency ablation if you suffer from: two-step process including a diagnostic injection prior to • Chronic hip pain the radiofrequency treatment. • Osteoarthritis of the hip How is it performed? Prior to the radiofrequency treatment, you will undergo a diagnostic injection. This diagnostic injection will involve a small amount of local anesthetic which will be injected in two spots around the hip. These injections are done under fluoroscopic x-ray guidance to help ensure proper placement of the needle. If you experience an adequate amount of pain relief with these injections, you will be eligible for the radiofrequency treatment. The radiofrequency treatment will then entail creating a heat lesion around the identified nerves which will help to prevent pain signals from traveling to the brain. Prior to your appointment You will have the option of receiving no sedation or: • oral sedation – or – • intravenous sedation If choosing sedation, you must not eat for six hours or drink anything for four hours before the procedure. To schedule a procedure You may continue taking all medications except blood thinners before the Please contact the nurse navigators procedure. -

Radiofrequency Ablation
Radiofrequency Ablation Radiofrequency ablation uses electricity to produce heat and numb nerve(s) that carry signals from a painful part of the body. The following are examples of radio-frequency ablation treatment: • Ablation of nerves supplying facet and/or sacroiliac joint, for treatment of back pain. • Ablation of nerves supplying a part of the body, for treatment of painful post-operative scar. • Ablation of the nerve supplying a painful joint. What are facet and sacroiliac joints? Facet joints (FJs) are pairs of small joints located at the back of the spine where one vertebra overlaps the next vertebra. These joints provide stability to the spine and allow it to twist and bend. Sacroiliac joints (SIJs) join the spine to the hips. Why do I need this treatment? Radiofrequency ablation to facet joints can treat neck (cervical), mid- back (thoracic) or low-back (lumbar) pain caused by degeneration/wear and tear of one or more of these facet joints. Cervical FJ degeneration can cause pain in the neck, shoulders arm and headache. Lumbar FJ degeneration can cause pain in the back, buttocks, groin and legs. SIJ degeneration can cause back and leg pain. Please inform us if you: • Are on medicines that thin the blood or prevent clotting, eg, Aspirin, Apixaban, Clopidogrel, Dipyridamole, Prasugrel, Rivaroxaban and Warfarin. We also need to know the name of the consultant who started you on the medication. WPR41994 July 2020 Review date: July 2022 • Suffer from a blood disorder that interferes with clotting eg haemophilia. • Are allergic to any medicine, food, sticky tapes, metal or latex. -

ECG Changes During Radiofrequency Ablation of Liver Metastasis Under General Anaesthesia - a Dilemma with Cardiac Event
Journal of Anesthesia & Critical Care: Open Access Case Report Open Access ECG changes during radiofrequency ablation of liver metastasis under general anaesthesia - a dilemma with cardiac event Abstract Volume 5 Issue 3 - 2016 Electrocardiogram (ECG) monitoring is one of the mandatory monitoring during surgery under anaesthesia for identifying any cardiac event like arrthymias or ischemic changes. Rakesh Garg, Rohini Dattatri, Swati Bhan, The operating room is increasingly being studded with various electrical equipments. Nishkarsh Gupta These electrical gadgets may interfere with the ECG monitoring and thus produce various Department of Onco-Anaesthesiology and Palliative Medicine, artifacts mimicking arrthymias or ischemic changes. We report a case of ECG changes Dr BRAIRCH, All India Institute of Medical Sciences, India induced artifactually by the use of radiofrequency ablation (RFA) for ablating hepatic metastasis under general anaesthesia. Our case emphasizes that awareness of such artifacts Correspondence: Rakesh Garg, Department of Anaesthesiology, Pain and Palliative Care, Dr BRAIRCH, All India in ECG during radiofrequency ablation is required and if it occurs it should be cautiously Institute of Medical Sciences, Room No. 139, Ist floor, Ansari interperated and managed. Nagar, New Delhi-110029, India, Tel 9810394950, 9868398335, Email Keywords: electrocardiogram, artifacts, radiofrequency ablation, malignancy, anaesthesia Received: July 28, 2016 | Published: August 04, 2016 Introduction was started and after excision of the pelvic mass, RFA procedure was initiated. RFA ablation of solitary liver metastasis was under done Electrocardiogram (ECG) monitoring is an essential monitoring ultrasound guidance using RF ablation probe (3-5cm) (Angiodynamics for patient undergoing surgery. It is a tool to pick up the cardiac RitaModel 1500X, Manchester, GA 31816). -
EP) Study and Radiofrequency Ablation (RFA
FACT SHEET FOR PATIENTS AND FAMILIES Electrophysiology (EP) study and Radiofrequency Ablation (RFA) What are EP and RFA, and What do I need to do next? why are they used? An electrophysiology [ee-lek-troh-fiz-ee-AW-loh-jee] (EP) 1 Make a list of all your current medicines and study is a test that shows how electrical signals move give it to your doctor. Write down everything in pathways through your heart. When the pathway is you are taking, including prescription drugs, over-the-counter medicines (like Tylenol, normal, your heartbeat is regular. When these signals cough syrup, or allergy pills), inhalers, patches, are abnormal, your heartbeat is irregular. An irregular vitamins, herbal remedies, or street drugs. heartbeat is called an arrhythmia [ah-RITH-mee-ah]. 2 Tell your doctor if you are allergic to any Symptoms of an arrhythmia are different in each medicines or dyes. person. They can include: 3 Follow your doctor’s directions about taking your medicines. If you are taking • A pounding or rapid heartbeat an anticoagulant [an-tie-koe-AG-yoo-lant] • A heart “flutter” (sometimes called a blood thinner), you may need to stop taking it before the procedure. • Dizziness or feeling lightheaded If you are taking diabetes medications, you • Shortness of breath may need to change when you take it before and after your procedure. Radiofrequency [ray-dee-oh-FREE-kwen-see] ablation 4 Follow all instructions on when to stop eating [ah-BLAY-shun] (RFA) is a procedure used to treat some and drinking before the procedure. This will types of arrhythmias. -
Left Atrial Radiofrequency Ablation During Mitral Valve Surgery for Continuous Atrial Fibrillation a Randomized Controlled Trial
ORIGINAL CONTRIBUTION Left Atrial Radiofrequency Ablation During Mitral Valve Surgery for Continuous Atrial Fibrillation A Randomized Controlled Trial George Doukas, FRCSI Context Although left atrial radiofrequency ablation (RFA) is increasingly used for Nilesh J. Samani, MD, FRCP the treatment of chronic atrial fibrillation during mitral valve surgery, its efficacy to Christos Alexiou, FRCS, PhD restore sinus rhythm and any resulting benefits have not been examined in the con- text of an adequately powered randomized trial. Mehmet Oc, MD Objective To determine whether intraoperative RFA of the left atrium increases the Derek T. Chin, MD long-term restoration of sinus rhythm and improves exercise capacity. Peter G. Stafford, MD Design, Setting, and Patients Randomized, double-blind trial performed in a single Leong L. Ng, MD UK tertiary referral center with enrollment between December 2001 and November 2003. A total of 101 patients referred for mitral valve surgery with at least 6 months’ Tomasz J. Spyt, FRCS, MD history of uninterrupted atrial fibrillation were assessed for eligibility; 97 were en- TRIAL FIBRILLATION IS A FRE- rolled. Patients were followed up for 12 months. quent and important con- Intervention Patients were randomly assigned to undergo mitral valve surgery and tributor to symptoms and RFA of the left atrium (n=49) or mitral valve surgery alone (controls; n=48). morbidity in patients with Main Outcome Measures The primary outcome measure was presence of sinus Amitral valve disease. More than 40% of rhythm at 12 months; secondary measures were patient functional status and exercise patients referred for mitral valve sur- capacity (assessed by shuttle-walk test), left atrial contractility, and left atrial and left gery have continuous atrial fibrilla- ventricular dimension and function and plasma levels of B-type natriuretic peptide.