Epidemic Spastic Paraparesis in Bandundu (Zaire)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Global and Local Health – Legacy of Hans Rosling
Seminar Global and Local Health – Legacy of Hans Rosling When: 26th October, 2017. 9.00 – 13.00. Where: Jacob Berzelius, Berzelius väg 3 Please register for the event here: https://sv.surveymonkey.com/r/PC3JR9Z In 2006, Hans Rosling presented his TED talk, which made him known internationally and changed the way we look at the world. However, long before that Hans Rosling had discovered a disease related to Cassava toxicity. It is an interesting story of a researcher who went to Mozambique to work as a health worker. Hans Rosling and his wife had traveled from Sweden to Mozambique. He had studied medicine and public health. In mid-1981, a disease appeared in the province of Nampula, north of Mozambique causing paralysis, with blurred vision and difficulty speaking. Soon over 1,000 cases were reported. The condition was called Konzo, which, in the Yaka language (spoken in a village of southeastern Democratic Republic of the Congo) means “tied legs.” Cassava is the third most important food crop in the tropics, after rice and maize. Esteemed by smallholder farmers for its tolerance to drought and infertile soils, the crop is inherently eco-efficient, offering a reliable source of food and income. Half a billion people in Africa eat cassava every day, and this high-starch root is also an important staple in Latin America and the Caribbean. The seminar “Global and Local Health – Legacy of Hans Rosling will discuss the disease Konzo in the context of research carried out by Hans Rosling. The seminar is a collaboration between Swedish Agriculture University, Uppsala (SLU – Global) and Centre for global health, Karolinska Institutet. -

Research on Motor Neuron Diseases Konzo and Neurolathyrism: Trends from 1990 to 2010
Research on Motor Neuron Diseases Konzo and Neurolathyrism: Trends from 1990 to 2010 Delphin Diasolua Ngudi1,2, Yu-Haey Kuo2, Marc Van Montagu2, Fernand Lambein2* 1 Programme National de Nutrition (PRONANUT), Kinshasa, Democratic Republic of the Congo, 2 Institute of Plant Biotechnology Outreach (IPBO), Ghent University, Ghent, Belgium Abstract Konzo (caused by consumption of improperly processed cassava, Manihot esculenta) and neurolathyrism (caused by prolonged overconsumption of grass pea, Lathyrus sativus) are two distinct non-infectious upper motor neurone diseases with identical clinical symptoms of spastic paraparesis of the legs. They affect many thousands of people among the poor in the remote rural areas in the central and southern parts of Africa afflicting them with konzo in Ethiopia and in the Indian sub-continent with neurolathyrism. Both diseases are toxico-nutritional problems due to monotonous consumption of starchy cassava roots or protein-rich grass pea seeds as a staple, especially during drought and famine periods. Both foods contain toxic metabolites (cyanogenic glycosides in cassava and the neuro-excitatory amino acid b-ODAP in grass pea) that are blamed for theses diseases. The etiology is also linked to the deficiency in the essential sulfur amino acids that protect against oxidative stress. The two diseases are not considered reportable by the World Health Organization (WHO) and only estimated numbers can be found. This paper analyzes research performance and determines scientific interest in konzo and neurolathyrism. A literature search of over 21 years (from 1990 to 2010) shows that in terms of scientific publications there is little interest in these neglected motorneurone diseases konzo and neurolathyrism that paralyze the legs. -

Similarities Between Tropical Spastic Paraparesis And
Lathyrus Lathyrism Newsletter 2 (2001) Similarities between Tropical Neurolathyrism Neurolathyrism is a neurologic disorder caused by Spastic Paraparesis (TSP) and excessive ingestion of Lathyrus species. Lathyrism has neurolathyrism been known since ancient times; epidemics have occurred in some regions, including Russia, southern Europe, the Middle East and India, particularly during times of famine. At these times increased consumption of Lathyrus sativus, L. cicera and Vicia sativa has been implicated. Horses, cattle, swine and birds have been Vladimir Zaninovic’ affected. Emeritus Professor of Neurology, Universidad del Clinically, lathyrism often presents relatively rapidly Valle, Cali, Colombia after a prolonged period (months) of ingesting large amounts of the grain, often in the context of general malnutrition. Disease often commences with Email: [email protected] OR complaints of pain or cramps in the legs or in the [email protected] region of the lumbar spine. Lower extremity weakness and sphincter disfunction then develop, soon evolving into permanent spastic paraparesis. The cramping pains and the sphincter dysfunction usually subside when the intoxication ceases and spasticity develops7. There are a few pathologic studies of lathyrism, but a report by Hirano et al.8 confirms earlier descriptions of bilateral atrophy in the distal pyramidal tract in the lumbar cord. Additionally, there have been Tropical Spastic Paraparesis morphologic descriptions of degenerative changes in Tropical Spastic Paraparesis (TSP) is a slowly the spinocerebellar tracts and dorsal columns. In progressive spastic paraparesis with an insidious onset concert, these data suggest a central nervous system in adulthood. It has been found all around the world (CNS) disease expressed most pronouncedly in the (except in the poles), mainly in tropical and subtropical distribution of the longest CNS fibres. -

Awareness and Knowledge of Konzo and Tropical Ataxic Neuropathy (TAN) Among Women in Andom Village - East Region, Cameroon
International Journal of Research and Review www.ijrrjournal.com E-ISSN: 2349-9788; P-ISSN: 2454-2237 Original Research Article Awareness and Knowledge of Konzo and Tropical Ataxic Neuropathy (TAN) Among Women in Andom Village - East Region, Cameroon Esther Etengeneng Agbor1, J Howard Bradbury2, Jean Pierre Banea3, Mbu Daniel Tambi4,A Desire Mintop5, Koulbout David6, R Mendounento7 1Senior Lecturer/researcher, Department of Biochemistry, University of Dschang – Cameroon 2Evolution, Ecology and Genetics Research School of Biology, Australian National University, Canberra, ACT 0200 Australia 3Programme National de Nutrition (PRONANUT), Kinshasa, Democratic Republic of Congo (DRC) 4Lecturer, Department of Agricultural Economics, University of Dschang, Cameroon 5Medical Doctor, Regional delegation of Ministry of Public health – Bertoua, East region - Cameroon 6Administrator/researcher, Regional delegation of Ministry of Scientific Research and Innovation - Cameroon 7Medical personnel, Government health Centre – Andom, East Region – Cameroon. Corresponding author: Esther Etengeneng Agbor Received: 29/10/2014 Revised: 25/11/2014 Accepted: 25/11/2014 ABSTRACT Background: Konzo and Tropical Ataxic Neuropathy (TAN) are toxico – nutritional neurological diseases associated with sub-lethal and moderate dietary cyanide exposure respectively, resulting from the consumption of insufficiently processed cassava products. In Cameroon, the cassava growing and consuming rural communities appear to have little awareness and knowledge of these nutritional diseases. Objective: To provide a preliminary insight into the awareness and knowledge of Konzo and TAN among rural women specifically in Andom village located in the East Region of Cameroon. Methodology: A convenient sample of 57 women between the ages of 20 - 70 years from a cassava growing/consuming local community was surveyed about Konzo and TAN. -

Neuro-Ophthalmologic Findings in Konzo, an Upper Motor Neuron Disorder in Africa
European Journal of Ophthalmology / Vol. 13 no. 4, 2003 / pp. 383-389 Neuro-ophthalmologic findings in konzo, an upper motor neuron disorder in Africa J.-C.K. MWANZA 1,5, D. TSHALA-KATUMBAY 2,3, D.L. KAYEMBE 1, K.E. EEG-OLOFSSON 4, T. TYLLESKÄR 5 1 Department of Ophthalmology, Kinshasa University Hospital, Kinshasa 2 Department of Neurology, Kinshasa University Hospital, Kinshasa - Democratic Republic of Congo 3 Center for Research on Occupational and Environmental Toxicology, Oregon Health Sciences University, Portland, Oregon - USA 4 Department of Neurosciences, Section for Clinical Neurophysiology, Uppsala University Hospital, Uppsala - Sweden 5 Center for International Health, University of Bergen, Bergen - Norway PURPOSE. To investigate the neuro-ophthalmological manifestations in konzo, a non-pro- gressive symmetric spastic para/tetraparesis of acute onset associated with consumption of insufficiently processed bitter cassava roots combined with a low protein intake. METHODS. Twenty-one Congolese konzo patients underwent neuro-ophthalmological inves- tigations including visual acuity testing, assessment of light pupillary reflexes, evaluation of ocular motility and deviation, direct ophthalmoscopy, and visual field perimetry. Objec- tive refraction including retinoscopy and keratometry, and slit-lamp biomicroscopy were al- so done. RESULTS. Five patients had visual impairment, and 14 had temporal pallor of the optic disc. Fourteen presented visual field defects, the most frequent being concentric constriction and peripheral defects. Overall, 11 subjects had symptoms qualifying for the diagnosis of optic neuropathy. Two had spontaneous pendular nystagmus in primary position of gaze. Visual field defects and pallor of the optic discs were found in mild, moderate and severe forms of konzo. No correlation was found between the severity of the motor disability of konzo and the extent of visual field loss. -

Reviewing the Effect of Bitter Cassava Neurotoxicity on the Motor Neurons of Cassava-Induced Konzo Disease on Wistar Rats Stella Enefa, Chikwuogwo W
Saudi Journal of Medicine Abbreviated Key Title: Saudi J Med ISSN 2518-3389 (Print) |ISSN 2518-3397 (Online) Scholars Middle East Publishers, Dubai, United Arab Emirates Journal homepage: https://saudijournals.com Original Research Article Model of Konzo Disease: Reviewing the Effect of Bitter Cassava Neurotoxicity on the Motor Neurons of Cassava-Induced Konzo Disease on Wistar Rats Stella Enefa, Chikwuogwo W. Paul, Lekpa K. David* Department of Anatomy, Faculty of Basic Medical Sciences, College of Health Sciences, University of Port Harcourt, Rivers State, Nigeria DOI: 10.36348/sjm.2020.v05i11.005 | Received: 05.10.2020 | Accepted: 21.10.2020 | Published: 28.11.2020 *Corresponding Author: Lekpa K. David Abstract Introduction: Cassava (Manihot Esculenta) is a staple food in tropical and subtropical regions in Africa, and is the main source of carbohydrate in these regions. Nevertheless, it contains cyanogenic glycosides metabolised to hydrogen cyanide, which has been shown by studies to affect the motor neurons of the central nervous system and causes neurodegenerative disease as konzo. However, the cassava-induced konzo disease and its neurotoxicity in rat model is yet to be explored. Method: 30 Adult female Wistar rats were assigned to 4 experimental groups (i) negative control n=5 (ii) positive control n=5, (iii) konzo-induced group n=15, (iv) protein-treated group n=5. The bitter cassava foods were taken by oral ingestion for a period of 5 weeks. Motor activity was evaluated using forelimb grip strength testing done weekly. RESULTS: There was significant difference in weight and forelimb grip strength between the negative control group and the konzo-induced group p˂0.05. -

Toxic Disorders of the Upper Motor Neuron System
4738-Eisen-18 6/16/06 5:58 PM Page 361 Handbook of Clinical Neurology, Vol. 82 (3rd series) Motor Neuron Disorders and Related Diseases A.A. Eisen, P.J. Shaw, Editors © 2007 Elsevier B.V. All rights reserved Chapter 18 Toxic disorders of the upper motor neuron system D. DESIRE TSHALA-KATUMBAY* AND PETER S. SPENCER Center for Research on Occupational and Environmental Toxicology and Department of Neurology, School of Medicine, Oregon Health and Science University, Portland, Oregon, USA 18.1. Introduction 18.2. Epidemiology Dysfunction of the motor system has been associated 18.2.1. Historical background with dietary dependence on food plants with neurotoxic potential, notably the grass pea (chickling pea) and cas- Lathyrism has affected humans and animal populations sava (manioc), in various and geographically distinct since antiquity. The disease was known to ancient regions of the world. Reliance on grass pea (Lathyrus Hindus, to Hippocrates (460–377 BC), Pliny the Elder sativus or related neurotoxic species) or on insufficiently (23–79 AD), Pedanius Dioskurides (50 AD) and Galen processed bitter cassava (Manihot esculenta Crantz) as (130–210 AD) (Desparanches, 1829; Hippocrates, staples, the latter in association with malnutrition, has 1846; Proust, 1883; Hubert, 1886; Schuchardt, 1887; resulted in epidemics of (neuro)lathyrism and konzo Spirtoff, 1903). Lathyrism affects populations reliant (neurocassavism), respectively; these are clinically on food products derived from neurotoxic species of the similar self-limiting neurodegenerative disorders con- Lathyrus genus, member of the Fabacae family, most fined to the upper motor neuron system. Studies of out- commonly Lathyrus sativus (grass pea) (Stockman, breaks of lathyrism and konzo have suggested 1917; Selye, 1957; Dwivedi and Prasad, 1964; Rao et al., individual susceptibility to the toxic effects of these 1969; Kislev, 1985). -
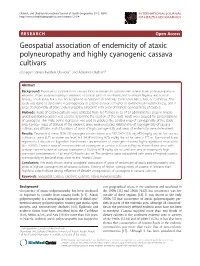
Geospatial Association of Endemicity of Ataxic Polyneuropathy and Highly Cyanogenic Cassava Cultivars Olusegun Steven Ayodele Oluwole1* and Adeyinka Oludiran2
Oluwole and Oludiran International Journal of Health Geographics 2013, 12:41 INTERNATIONAL JOURNAL http://www.ij-healthgeographics.com/content/12/1/41 OF HEALTH GEOGRAPHICS RESEARCH Open Access Geospatial association of endemicity of ataxic polyneuropathy and highly cyanogenic cassava cultivars Olusegun Steven Ayodele Oluwole1* and Adeyinka Oludiran2 Abstract Background: Exposure to cyanide from cassava foods is present in communities where ataxic polyneuropathy is endemic. Ataxic polyneuropathy is endemic in coastal parts of southwest and southeast Nigeria, and coastal Newala, south India, but it has been reported in epidemic or endemic forms from Africa, Asia, or Caribbean. This study was done to determine if cyanogenicity of cassava cultivars is higher in lowland than highland areas, and if areas of endemicity of ataxic polyneuropathy colocalize with areas of highest cyanogenicity of cassava. Methods: Roots of cassava cultivars were collected from 150 farmers in 32 of 37 administrative areas in Nigeria. Global positioning system was used to determine the location of the roots. Roots were assayed for concentrations of cyanogens. Thin Plate Spline regression was used to produce the contour map of cyanogenicity of the study area. Contour maps of altitude of the endemic areas were produced. Relationship of cyanogenicity of cassava cultivars and altitude, and of locations of areas of high cyanogenicity and areas of endemicity were determined. Results: Geometrical mean (95% CI) cyanogen concentration was 182 (142–233) mg HCN eq/kg dry wt for cassava cultivars in areas ≤ 25 m above sea level, but 54 (43–66) mg HCN eq/kg dry wt for areas > 375 m. Non-spatial linear regression of altitude on logarithm transformed concentrations of cyanogens showed highly significant association, (p < 0.0001). -
Konzo and Cassava Toxicity
KONZO AND CASSAVA TOXICITY A STUDY OF ASSOCIATED NUTRITIONAL FACTORS IN THE POPOKABAKA DISTRICT, DEMOCRATIC REPUBLIC OF CONGO Delphin DIASOLUA NGUDI Academic Year 2004-2005 KONZO AND CASSAVA TOXICITY: A STUDY OF ASSOCIATED NUTRITIONAL FACTORS IN THE POPOKABAKA DISTRICT, DEMOCRATIC REPUBLIC OF CONGO KONZO-ZIEKTE EN DE TOXICITEIT VAN MANIOK: EEN STUDIE VAN DE VOEDINGSFACTOREN IN POPOKABAKA DISTRICT, DEMOCRATISCHE REPUBLIEK KONGO Door Delphin DIASOLUA NGUDI, M.Sc. Thesis submitted in fulfilment of the requirements for the degree of Doctor (Ph.D.) in Applied Biological Sciences Proefschrift voorgedragen tot het bekomen van de graad van Doctor in the Toegepaste Biologische Wetenschappen Op gezag van: Rector: Prof. Dr. Apr. A. DE LEENHEER Decaan: Promotoren: Prof. Dr. Ir. Herman VAN LANGENHOVE Prof. Dr. Patrick KOLSTEREN Prof. Dr. Ir. Fernand LAMBEIN CITATION “A person who has food has many problems. A person who has no food has only one problem” Chinese saying DEDICATION To Thérèse Luntala and our sons Berdit, Gaël and Beni In memory of my Grand Oncle André Banketa and my father Bernard Ngudi-a-nkama Promotoren: Prof. Dr. Patrick KOLSTEREN Vakgroep Voedselveiligheid en Voedselkwaliteit, Universiteit Gent Voedings unit, Prins Leopold Instituut voor Tropische Geneeskunde, Antwerpen Prof. Dr. Ir. Fernand LAMBEIN Instituut Planten Biotechnologie voor Ontwikkelingenlanden, Universiteit Gent Decaan: Prof. Dr. Ir. Herman VAN LANGENHOVE Academiejaar 2004 - 2005 Delphin DIASOLUA NGUDI KONZO AND CASSAVA TOXICITY A STUDY OF ASSOCIATED NUTRITIONAL FACTORS IN THE POPOKABAKA DISTRICT, DEMOCRATIC REPUBLIC OF CONGO Proefschrift voorgedragen tot het bekomen van de graad van Doctor in de Toegepaste Biologische Wetenschappen Op gezag van de rector, Prof. Dr. Apr. -

Contents 2,5 Differential Diagnosis of in the Same Population
Working together to eliminate cyanide poisoning, konzo and tropical ataxic neuropathy (TAN). Cassava Cyanide Diseases Network Issue Number 12, December 2008 and konzo if both disorders occurred Contents 2,5 Differential diagnosis of in the same population. konzo from other tropical Konzo and TAN have been Differential diagnosis of diseases: a review attributed to dietary cyanide konzo from other tropical exposure from consumption of diseases: a review .............. 1 Konzo with its upper motor neurone insufficiently processed cassava manifestations can be confused with roots, but rates of exposure differ in 7 other diseases and differential both diseases. In contrast to konzo, Comparison of cassava flour diagnosis is important. Using the TAN is a progressive disorder with and gari .................................... 2 WHO criteria, konzo by its spastic slow onset that mainly affects older paraparesis can easily be adults. Furthermore, konzo involves distinguished from causes of flaccid damage to upper motor neurones Outbreak of konzo disease in paraplegia such as poliomyelitis, without sensory involvement, health region No. 2 of the leprosy or trauma.1 The commonest whereas TAN is mainly caused by damage of sensory neurons in the Central African Republic ....... 3 neurological diseases to be considered in its differential spinal cord resulting in ataxia. TAN diagnoses include neurolathyrism, rarely progresses to inability to walk, Endomyocardial fibrosis: Tropical Ataxic Neuropathy (TAN) whereas walking difficulties are the primary symptom of konzo and a cause still unknown ................ 4 and Tropical Spastic Paraparesis/ HTL V-I Associated Myelopathy high proportion of the konzo- (TSP/HAM) (see Table 1). affected subjects are unable to walk. About half of the TAN cases have Konzo is clinically very similar to optic atrophy which is rare among konzo cases. -

Increased Sensitization of Health Workers Leading to Detection of Unintended Cases of Acute Flaccid Paralysis: a Case of a “Konzo” Outbreak in Western Zambia
Medical Journal of Zambia, Vol. 43 (2): pp 57 - 60 (2016) ORIGINAL ARTICLE Increased Sensitization of Health Workers Leading to Detection of Unintended Cases of Acute Flaccid Paralysis: A Case of a “Konzo” Outbreak in Western Zambia A Mtonga1, P Mwaba2, MLM Mazaba1,3, E Chizema2, M Kapina2, S Mwangala4, A Silumesi4, F Masaninga5, T Masuka4, L Hachambwa5, O Siddiqi5, I Mweene-Ndumba1, JS Kachimba5, B Vwalika5, S Kagulura5, P Songolo1, J Mufunda1 1World Health Organization, Lusaka, Zambia, 2Ministry of Health, Lusaka, Zambia 3Copperbelt University School of Medicine, Ndola, Zambia 4Ministry of Health, Mongu, Zambia, 5University of Zambia, School of Medicine, Lusaka, Zambia ABSTRACT comprehensively investigated the cases. To improve the diagnosis a detailed case investigation form and checklist Background: The threat of high profile diseases causing were used to capture clinical data and socio demographic outbreaks has drawn attention to public health information. surveillance systems, much needed for the timely detection of outbreaks. A disease characterized by Laboratory investigations included routine urine weakness of the lower limbs in Luatembo rural health microscopy and full blood count. Further analysis facility was reported to the province in 2013. Through the included viral analysis for enteroviruses, Acute Flaccid Paralysis surveillance (AFP) program the cytomegalovirus among others, copper levels and Western Province in Zambia recorded an increase in the thiocyanate levels. numbers of people affected with spastic paraparesis. The disease affected clusters of families, especially women Results: Preliminary laboratory results indicated no viral and children. The disease was found to be in specific infections. Thiocyanate and copper levels are yet to be geographic areas, with the initial cases being identified in analysed. -

Download File CCDN 30.Pdf
Working together to eliminate cyanide poisoning, konzo, tropical ataxic neuropathy (TAN) and neurolathyrism Cassava Cyanide Diseases & Neurolathyrism Network (ISSN 1838-8817 (Print): ISSN 1838-8825 (Online) Issue Number 30, December 2017 Contents an Ethiopian boy adopted in an American family 2. Editorial ......................................................................... 1 Some ‘recycled’ reports on cases that occurred Articles ........................................................................... 2 decades ago in India or Ethiopia were also Hans Rosling – edutainer and konzo researcher ........ 2 published. In the present issue professor Mishra Survey of grass pea consumption in Gazipur, Uttar reports on a survey in an area of India that is Pradesh, India ............................................................... 5 supposed to be prone to neurolathyrism, but found Mapping of konzo and rehabilitation needs in no new cases. The local diet consisted of a mixture Zambezia Province, Mozambique ................................ 6 of rice and grass pea seasoned with onion. This confirms the findings of dr Getahun in Ethiopia who CCDNN Coordination: identified addition of cereals and onion as protective 3 factors in the epidemiology of neurolatyrism . When dr Gopalan visited the Rewa district he noted that rice was cheaper than grass pea and that market Technologiepark 3, B-9052 Gent -Zwijnaarde, Belgium effects may be responsible for the absence of new Prof Fernand LAMBEIN, Coordinator cases of neurolathyrism. Also in Bangladesh no [email protected] recent cases are reported in the literature, and the price of rice seems to be lower than the price of Dr. Delphin DIASOLUA NGUDI grass pea. Poverty and food insufficiency during Phone: +32 92 64 52 82 Email: [email protected] or [email protected] drought are often reported as risk factors, when the poorest and often illiterate only can afford the Editorial Board: J.P.