The Imaging Features of Metanephric Adenoma: a Case Report and Review of Literature
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Genitourinary PAX8
174A ANNUAL MEETING ABSTRACTS RMC and 19/21 (90%) of CDC cases. In contrast, 31/34 (91%) UUC were negative for Genitourinary PAX8. p63: p63 was positive in 7/12 (58%) RMC and in 3/21 (14%) CDC. Staining was focal in 6/7 RMC and strong in 4/7. Almost all (97%) UUC were p63 positive 767 Histopathologic Features of Bilateral Renal Cell Carcinomas: A (moderate/strong and multifocal/diffuse in 80% of cases). The one p63 negative UUC Study of 24 Cases was a microinvasive high grade tumor and was also negative for PAX8. J Abdelsayed, JY Ro, LD Truong, AG Ayala, SS Shen. The Methodist Hospital and Weill Conclusions: We suggest a binary panel of PAX8 and p63 as an aid in the differential Medical College of Cornell University, Houston, TX. diagnosis of high grade renal sinus epithelial neoplasms. (PAX8+/p63+) profile Background: The incidence of bilateral renal cell carcinoma (bRCC) has been reported supported the dx of RMC with a sensitivity of 58.3% and specificity of 89%. (PAX8+/ to vary from 1.5% to 11%. Clear understanding of the clinicopathologic features of p63-) profile supported the diagnosis of CDC with a sensitivity of 85.7% and a specificity bRCCs including the distinction between synchronous and metachronous tumors has of 89%. Finally (PAX8-/p63+) profile supported the diagnosis of UUC with a sensitivity important implications in patients’ management and follow up. The purpose of this study of 88% and a specificity of 100%. The concomitant expression of p63 and PAX8 in RMC is to summarize the clinicopathologic features of bRCCs and compare them with those seen in our study further suggests an intermediate phenotype between renal tubular and of unilateral renal cell carcinomas (uRCCs). -

A Metanephric Adenoma of the Kidney Associated with Polycythemia: a Case Report
352 ONCOLOGY LETTERS 11: 352-354, 2016 A metanephric adenoma of the kidney associated with polycythemia: A case report PENGFEI WANG, YUAN TIAN, YUEHAI XIAO, YANG ZHANG, FA SUN and KAIFA TANG Department of Urology, Affiliated Hospital of Guizhou Medical University, Guiyang, Guizhou 550004, P.R. China Received January 11, 2015; Accepted September 24, 2015 DOI: 10.3892/ol.2015.3868 Abstract. Metanephric adenoma (MA) of the kidney is a 54-year-old female that presented with MA associated with rare and frequently benign tumor with a favorable prognosis polycythemia. that is often diagnosed following surgical treatment. In the present study, a 54-year-old female patient presented with Case Report complaints of intermittent right-flank pain and anterior abdominal pain occurring over 2 years and sporadic gross A 54-year-old female patient presented to the Affiliated hematuria occurring over 3 months. Ultrasonography and Hospital of Guizhou Medical University (Guiyang, China), computerized tomography imaging revealed a neoplasm with complaints of intermittent right flank pain and ante- lesion localized in the right kidney. Successful open approach rior abdominal pain that occurred over a 2-year period and radical nephrectomy was performed and post-surgical histo- sporadic gross hematuria that occurred over 3 months in pathological examination verified the lesion as a MA of the March 2013. The patient had no other symptoms. Physical kidney. Radical nephrectomy, cryoablation or radiofrequency examination revealed no significant conclusions. Urinalysis may used to treat MA and a selective panel of immunostains, revealed hematuria in the urine culture and a routine including WT1, EMA and AMACR, may be useful for diag- blood examination exhibited a hematocrit (Hct) volume of nosis. -

Metanephric Adenoma with Diffuse Calcifications: a Case Report
1816 ONCOLOGY LETTERS 10: 1816-1818, 2015 Metanephric adenoma with diffuse calcifications: A case report JINGTAO WU*, QINGQIANG ZHU*, WENRONG ZHU and HONGYING ZHANG Department of Medical Imaging, Subei People's Hospital, Medical School of Yangzhou University, Yangzhou, Jiangsu 225001, P.R. China Received September 2, 2014; Accepted April 29, 2015 DOI: 10.3892/ol.2015.3491 Abstract. Metanephric adenoma is a rare and benign renal to the development of less invasive treatment strategies in the neoplasm originating in the epithelial cells of the kidney. future. The current study presents the case of a male patient The tumor has a benign course and a characteristic histo- diagnosed with atypical metanephric adenoma with diffuse pathological appearance, typically exhibiting a solid and calcifications who subsequently underwent radical nephrectomy. poorly-demarcated margin with rare cystic components or calcifications. However, it is often difficult to distinguish Case report metanephric adenoma from malignant neoplasms prior to surgical resection. To the best of our knowledge, only one case A 23‑year‑old male patient was admitted to Subei People's of metastasis to the lymph nodes has been described in the Hospital (Yangzhou, China) with a history of flank pain literature thus far. The present study retrospectively analyzed on October 23, 2013, and appeared in good general condi- one case of surgically and pathologically‑confirmed atypical tion. The patient had no history of occupational exposure metanephric adenoma. Clinical and pathological analysis, as to carcinogens.At >1 month after the onset of symptoms, a well as computed tomography scans, revealed a mass with a medical examination identified a left renal mass with diffuse clearly defined margin and diffuse calcifications. -

Imaging Findings of Common Benign Renal Tumors in The
Review Article | Genitourinary Imaging http://dx.doi.org/10.3348/kjr.2015.16.1.99 pISSN 1229-6929 · eISSN 2005-8330 Korean J Radiol 2015;16(1):99-113 Imaging Findings of Common Benign Renal Tumors in the Era of Small Renal Masses: Differential Diagnosis from Small Renal Cell Carcinoma – Current Status and Future Perspectives Sungmin Woo, MD1, Jeong Yeon Cho, MD1, 2 1Department of Radiology, Seoul National University College of Medicine, Seoul 110-744, Korea; 2Institute of Radiation Medicine and Kidney Research Institute, Seoul National University Medical Research Center, Seoul 110-744, Korea The prevalence of small renal masses (SRM) has risen, paralleling the increased usage of cross-sectional imaging. A large proportion of these SRMs are not malignant, and do not require invasive treatment such as nephrectomy. Therefore, differentation between early renal cell carcinoma (RCC) and benign SRM is critical to achieve proper management. This article reviews the radiological features of benign SRMs, with focus on two of the most common benign entities, angiomyolipoma and oncocytoma, in terms of their common imaging findings and differential features from RCC. Furthermore, the role of percutaneous biopsy is discussed as imaging is yet imperfect, therefore necessitating biopsy in certain circumstances to confirm the benignity of SRMs. Index terms: Small renal mass; Angiomyolipoma; Oncocytoma; Renal cell carcinoma INTRODUCTION instance, in a report by Frank et al. (6), it was found that 30% of tumors less than 2 cm in diameter were benign, The increased detection of small renal tumors has whereas 20% of those with a diameter greater than 4 cm paralleled the increased use of cross-sectional imaging (1). -

Wilms' Tumour – Histology and Differential Diagnosis
Chapter 1 Wilms’ Tumour – Histology and Differential Diagnosis Sergey D. Popov,1 Neil J. Sebire,2 Gordan M. Vujanic1 1Department of Cellular Pathology, University Hospital of Wales, Cardiff, UK; 2Department of Histopathology, Great Ormond Street Hospital, London, UK Author for correspondence: Sergey D. Popov, MD, PhD, Department of Cellular Pathology, University Hospital of Wales, Cardiff CF14 4XW, UK. Email: [email protected]; [email protected] Doi: http://dx.doi.org/10.15586/codon.wt.2016.ch1 Copyright: The Authors. Licence: This open access article is licensed under Creative Commons Attribution 4.0 Interna- tional (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/ Users are allowed to share (copy and redistribute the material in any medium or format) and adapt (remix, transform, and build upon the material for any purpose, even commercially), as long as the authors and the publisher are explicitly identified and properly acknowledged as the original source. Abstract Wilms’ tumour (WT) is the most common paediatric renal tumour, which can present as a single nodule, as multifocal unilateral lesions or as bilateral tumours. Typically, WT comprises three histological components namely blastemal, epithelial and stro- mal. The proportion and the degree of maturation of these components vary signifi- cantly, making the histological appearance of each tumour unique. Classical triphasic WT rarely presents diagnostic difficulty for pathologists, but when only one compo- nent is present, especially in a small biopsy specimen, the differential diagnosis may In: Wilms Tumor. Marry M. van den Heuvel-Eibrink (Editor) ISBN: 978-0-9944381-1-9; Doi: http://dx.doi.org/10.15586/codon.wt.2016 Codon Publications, Brisbane, Australia Popov et al. -

Imaging of Unusual Renal Tumors
Current Urology Reports (2019) 20: 5 https://doi.org/10.1007/s11934-019-0867-7 KIDNEY DISEASES (G CIANCIO, SECTION EDITOR) Imaging of Unusual Renal Tumors R. Patricia Castillo1 & Juan Francisco Santoscoy1 & Leonardo Pisani 1 & Beatrice L. Madrazo1 & V. Javier Casillas1 Published online: 21 January 2019 # Springer Science+Business Media, LLC, part of Springer Nature 2019 Abstract Purpose of Review Renal masses are a wide entity and a common finding in clinical practice. Detection of these masses has increased in the last years, yet mortality rates have slightly decreased. Recent Findings According to the World Health Organization classification, there are 8 types, 51 subtypes, and a lot more subsequent subclassifications of renal tumors. Histopathological analysis should always be assessed for final diagnosis of theses tumors. However, imaging can be an important diagnostic guidance. The most common diagnoses of renal tumor are clear cell carcinoma, papillary renal cell carcinoma, angiomyolipoma, and transitional cell carcinoma. Nonetheless, a considerable variety of particular tumors can arise from the kidney, challenging the expertise of radiologists and urologists on this subject. Summary The awareness of these unusual entities is vital for professionals working at a complex medical facility with greater volume of patients. We hereby present uncommon renal tumors and its pathological and radiological features. Keywords Renalneoplasm . Renal cell tumor . Mesenchymalrenaltumor .Mixedepithelialand stromaltumors .Imagingfeatures Introduction recommended by the World Health Organization (WHO) and is the most frequently used grading system in RCC Renal masses are a wide heterogeneous entity that is frequent- but has not been validated for most of the new subtypes of ly diagnosed incidentally. -

Metanephric Adenoma with Cystic Changes- an Uncommon Presentation of a Rare Tumor in a Young Adult
Article / Clinical Case Report Metanephric Adenoma with cystic changes- An uncommon presentation of a rare tumor in a young adult Darilin Shangplianga , Pakesh Baishyaa , Jaya Mishraa , Evarisalin Marbanianga , Biswajit Deya , Baphira Wankharb , Ronika Saikiaa How to cite: Shangpliang D, Baishya P, Mishra J, et al. Metanephric Adenoma with cystic changes- An uncommon presentation of a rare tumor in a young adult. Autops Case Rep [Internet]. 2020;10(3):e2020148. https://doi.org/10.4322/ acr.2020.148 ABSTRACT Metanephric adenoma (MA) is a rare benign neoplasm of the kidney that is usually asymptomatic and incidentally diagnosed. MA usually present as a solid mass; however, a cystic presentation has been reported. The main differential diagnosis of MA is the epithelial predominant Wilms tumor (e-WT) and the solid variant of papillary renal cell carcinoma (pRCC). The presence of the BRAF gene mutation has recently been reported in 85% of MA, and less than 10% of cases of MA do not express this specific gene mutation. Herein we report a 22-year-old man who presented with back pain and abdominal discomfort with a renal mass on the computed tomographic scan. The diagnosis of metanephric adenoma was confirmed histopathologically. In our case, the tumor presented as a solid and cystic mass hence mimicking a papillary renal cell carcinoma. The VE1 protein, which correlates with BRAF gene mutation, did not show any significant expression. We want to highlight that MA can present as a cystic lesion that should be taken into account to avoid unnecessary radical nephrectomy. Also, we demonstrated that a subset of MA might not harbor the BRAF gene and, they are classified as the BRAF wild type MA. -
A Study of 28 Cases
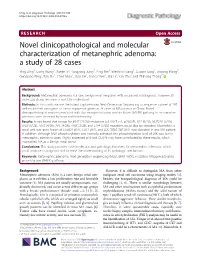
Ding et al. Diagnostic Pathology (2018) 13:54 https://doi.org/10.1186/s13000-018-0732-x RESEARCH Open Access Novel clinicopathological and molecular characterization of metanephric adenoma: a study of 28 cases Ying Ding1, Cong Wang1, Xuejie Li2, Yangyang Jiang3, Ping Mei4, Wenbin Huang5, Guoxin Song1, Jinsong Wang5, Guoqiang Ping1, Ran Hu1, Chen Miao1, Xiao He1, Gang Chen1, Hai Li1, Yan Zhu1 and Zhihong Zhang1* Abstract Background: Metanephric adenoma is a rare, benign renal neoplasm with occasional misdiagnosis. However, its molecular characterization is not fully understood. Methods: In this study, we use the hybrid capture-based Next-Generation Sequencing to sequence a panel of 295 well-established oncogene or tumor suppressor genes in 28 cases of MA patients in China. Novel clinicopathological markers associated with the mitogen-activated protein kinase (MAPK) pathway in metanephric adenoma were detected by immunohistochemistry. Results: It was found that except for BRAF (22/28) mutations (c.1799 T > A, p.V600E), NF1 (6/28), NOTCH1 (5/28), SPEN (5/28), AKT2 (4/28), APC (4/28), ATRX (3/28), and ETV4 (3/28) mutations could also be detected. Meanwhile, a novel and rare gene fusion of STARD9-BRAF, CUX1-BRAF, and LOC100507389-BRAF was detected in one MA patient. In addition, although MEK phosphorylation was normally activated, the phosphorylation level of ERK was low in metanephric adenoma cases. Highly expressed p16 and DUSP6 may have contributed to these results, which maintained MA as a benign renal tumor. Conclusions: This study provides novel molecular and pathological markers for metanephric adenoma, which could improve its diagnosis and increase the understanding of its pathologic mechanism. -
A Practical Approach to Surgical and Cytopathology
3rd Annual A Practical Approach to Surgical and Cytopathology Friday, April 7, 2017 Hotel Del Coronado Coronado, California Educational Symposia TABLE OF CONTENTS Friday, April 7, 2017 Diagnostic Approach to Flat and Papillary Urothelial Lesion (Ming Zhou, M.D.) ............................................................ 137 Practical Issues Related to the Endometrium Biopsy II (Marisa Rose Nucci, M.D.) .......................................................... 155 What’s New in the World Health Organization Classification of Lung Tumors (Carol Farver, M.D.) ................................ 185 Thyroid Pathology in the Molecular Era (Jennifer L. Hunt, M.D.) .................................................................................... 199 Pattern Based Approach to Diagnosis and Classification of Renal Tumors (Ming Zhou, M.D.) ...................................... 215 SAVE THE DATES - 2018 Pathology Symposia 137 138 Diagnostic Approach to Papillary and Flat Urothelial Clinical Implications of Pathological Diagnoses on TUR or Biopsy Specimens: Lesions What Diagnoses Pathologists Really Matter? Ming Zhou, MD, PhD Dr. Charles T. Ashworth Professor of Pathology Director, Anatomic Pathology The University of Texas Southwestern Medical Center Dallas, TX [email protected] What Diagnoses Pathologists May Not Need to Struggle with? 2 Pathological Parameters Important Urothelial Carcinoma Staging for Management of Patients with Ta, Tis- non- Urothelial Carcinoma invasive T1- Lamina propria invasion 1. Depth of invasion )tumor stage) T2- muscularis 2. Tumor grade propria invasion 3. Variant histology T3- Perivesical 4. Lymphovascular invasion invasion T4- Invasion into adjacent organs AJCC 2016 3 4 Grading of Papillary Urothelial Clinical Decision Based on Stage and Grade Neoplasms Muscle Radical cystectomy WHO 2016 Invasive UC LN dissection Biopsy/TUR Non-muscle 1. Papilloma Invasive UC 2. Papillary urothelial neoplasm of low malignant potential (PUNLMP) Low risk Intermediate risk High risk 3. -

Kidney Solid Tumor Rules
Kidney Equivalent Terms and Definitions C649 (Excludes lymphoma and leukemia M9590 – M9992 and Kaposi sarcoma M9140) Introduction Note 1: Tables and rules refer to ICD-O rather than ICD-O-3. The version is not specified to allow for updates. Use the currently approved version of ICD-O. Note 2: 2007 MPH Rules and 2018 Solid Tumor Rules are used based on date of diagnosis. • Tumors diagnosed 01/01/2007 through 12/31/2017: Use 2007 MPH Rules • Tumors diagnosed 01/01/2018 and later: Use 2018 Solid Tumor Rules • The original tumor diagnosed before 1/1/2018 and a subsequent tumor diagnosed 1/1/2018 or later in the same primary site: Use the 2018 Solid Tumor Rules. Note 3: Renal cell carcinoma (RCC) 8312 is a group term for glandular (adeno) carcinoma of the kidney. Approximately 85% of all malignancies of the kidney C649 are RCC or subtypes/variants of RCC. • See Table 1 for renal cell carcinoma subtypes/variants. • Clear cell renal cell carcinoma (ccRCC) 8310 is the most common subtype/variant of RCC. Note 4: Transitional cell carcinoma rarely arises in the kidney C649. Transitional cell carcinoma of the upper urinary system usually arises in the renal pelvis C659. Only code a transitional cell carcinoma for kidney in the rare instance when pathology confirms the tumor originated in the kidney. Note 5: For those sites/histologies which have recognized biomarkers, the biomarkers are most frequently used to target treatment. Biomarkers may identify the histologic type. Currently, there are clinical trials being conducted to determine whether these biomarkers can be used to identify multiple primaries. -

Largest Metanephric Adenoma Kidney with Polycythemia Incidentally
Surgica l & l U a r ic o l Manoharan et al., Med Sur Urol 2018, 7:4 d o e g y M DOI: 10.4172/2168-9857.1000212 Medical & Surgical Urology ISSN: 2168-9857 Case Report Open Access Largest Metanephric Adenoma Kidney with Polycythemia Incidentally Detected in a Blood Donor Vignesh Manoharan1, Kalpesh Parmar1*, Varinder Attri1, Shrawan Kumar Singh1, Pranjali Vasisht2, Prateek Bhatia2, Meenu Singh2 and Nandita Kakkar3 1Department of Urology, PGIMER, Chandigarh, India 2Department of Pediatrics, PGIMER, Chandigarh, India 3Department of Pathology, PGIMER, Chandigarh, India *Corresponding author: Kalpesh Parmar, Assistant Professor, Department of Urology, PGIMER, Chandigarh, India, Tel: 9915105062; E-mail: [email protected] Received date: September 09, 2018; Accepted date: December 10, 2018; Published date: December 17, 2018 Copyright: ©2018 Manoharan V, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Metanephric adenoma of kidney is a rare entity. It presents in young individuals and its association with polycythemia is well described. Differentiation from Wilm’s tumor and renal cell carcinoma is challenging and hence definitive diagnosis is made by histopathology with immunohistochemistry. Recognition of this entity is important as it has a more favourable clinical outcome compared with Wilms' tumor and renal cell carcinoma. We report a case of largest metanephric adenoma presenting with polycythemia incidentally detected in young female during blood donation and managed by radical nephrectomy. Keywords: Metanephric adenoma; Polychythemia; BRAF Introduction Metanephric tumors of kidney represent a spectrum which contains renal epithelial or stromal cells or both. -
Passive Seeding in Metanephric Adenoma a Review of Pseudometastatic Lesions in Perinephric Lymph Nodes
Case Reports Passive Seeding in Metanephric Adenoma A Review of Pseudometastatic Lesions in Perinephric Lymph Nodes Gladell P. Paner, MD; Thomas M. Turk, MD; Joseph I. Clark, MD; Valerie Lindgren, PhD; Maria M. Picken, MD, PhD c Lymph node involvement derived from a discrete neo- longs to the spectrum of putatively nephrogenic rest-de- plastic process fundamentally implies tumor malignancy. rived tumors, which also include Wilms tumor (WT), However, rarely, inconsequential passive transport of be- metanephric adeno®broma (MAF), and metanephric stro- nign neoplastic cells to the lymph node can occur and may mal tumor.1±3 Although WT, or nephroblastoma, is thought cause confusion as to the nature of the neoplasm (ie, ma- to represent the malignant end of this spectrum, the other lignant vs benign). We describe a 10-cm right renal meta- metanephric neoplasms are generally regarded as benign, nephric adenoma incidentally discovered in a 30-year-old and thus far, only a few reports have suggested that a woman during cesarean section for a triplet pregnancy. small subset of these tumors can have atypical histologic Subsequent nephrectomy following an equivocal needle bi- features and behavior.3±6 Recently,acaseofMAina7- opsy diagnosis showed histologic features classic for meta- year-old child was reported with lymph node involvement nephric adenoma, including the lack of cytologic atypia that was interpreted as metastasis.7 and mitoses. Necrosis present in this lesion appeared to be Some cells indigenous to the lymph node could be mis- secondary to tumor physical disruption. The tumor cells taken for metastatic carcinoma, such as lymphoid follicles were positive for Wilms tumor 1 (WT1) antigen, pankera- or germinal centers protruding into sinuses, histiocytic tin, and CD57, focally positive for epithelial membrane an- granulomas, thick endothelial cells of postcapillary ve- tigen, and negative for cytokeratin 7, cytokeratin 34bE12, nules, and rarely, nodal megakaryocytes.8 Moreover, be- and CD56.