Name: Nabina Lawoti Address: Bhadrapur:14, Jhapa E-Mail
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

"Disappearance" / Fear for Safety/Arbitrary Detention New Concern: Fear of Torture Or Ill-Treatment
PUBLIC AI Index: ASA 31/146/2004 27 July 2004 Further Information on UA 24/04 (ASA 31/010/2004, 19 January 2004) and follow-up (ASA 31/080/2004, 24 March 2004) - "Disappearance" / Fear for Safety/Arbitrary detention New concern: Fear of torture or ill-treatment NEPAL Pushpa Lal Dhakal (m) aged 31, farmer New Names: Pushpa Neupane (m) aged 25 four other unnamed people Amnesty International is seriously concerned for the safety of Pushpa Lal Dhakal, Pushpa Neupane and four other people who were reportedly rearrested by security forces personnel on 25 July. They were detained immediately after being released from Jhapa District Court, Chandragadi, Bhadrapur municipality and are at risk of torture or ill-treatment. At around 4pm on 25 July, Jhapa District Court reportedly ordered the release of Pushpa Lal Dhakal, Pushpa Neupane and four other people. As soon as they left the court premises they were reportedly arrested by around 50 armed security forces personnel in civilian clothes. Witnesses then saw them being taken away in a van towards Charali Army barracks. According to information received, Pushpa Lal Dhakal was first arrested on 13 January and held at Charali Army barracks for 10 days, where he was reportedly beaten so badly that several of his ribs were broken. He was then transferred to Chandragadi prison, where he was held under the Terrorist and Disruptive Activities (Control and Punishment) Act (TADA). His family were allowed four visits to the Chandragadi prison. On 26 July, Pushpa Lal Dhakal's family were reportedly told by an officer at Charali Army barracks that he was being held there following his rearrest. -

ANNUAL REPORT 2013/14 A.D.(2070/71 B.S.) 2 Sunrise Bank Limited Seventh Annual Report 2013/14 BOARD of DIRECTORS
;g\/fOh a}+s lnld6]8 SUNRISE BANK LIMITED RISING TO SERVE www.sunrisebank.com.np ANNUAL REPORT 2013/14 A.D.(2070/71 B.S.) 2 Sunrise Bank Limited Seventh Annual Report 2013/14 BOARD OF DIRECTORS MR. MOTILAL DUGAR Chairman DR. BHOGENDRA GURAGAIN ER. BACHH RAJ TATER MR. SHRAWAN KUMAR GOYAL MR. MALCHAND DUGAR Director Director Director Director DR. DEEPAK PRASAD MR. DEEPAK NEPAL MR. JYOTI KUMAR BEGANI MR. SHANKHAR PD. DAHAL BHATTARAI Public Director Public Director Professional Director Public Director MR. ISHWOR KUMAR PATHAK (Company Secretary) Seventh Annual Report 2013/14 Sunrise Bank Limited 3 FINANCIAL GLANCE OF THE YEAR 2013/14 DEPOSITS GROSS LOANS NET PROFIT 26,617M 20,978M 247M 14% 14% 21% NET INTEREST OTHER OPETATING STAFF & INCOME INCOME OPERATING COST 1,095M 309M 624M 11% 15% 14% LOAN LOSS PROVISION TAX TO PROVISION WRITE BACK GOVERNMENT 467M 94M 124M 27% 55% 16% NET INTEREST SPREAD NPA PERCENTAGE LIQUIDITY 4.55% 4.94% 33.31% 0.21% 1.20% 0.20% CAPITAL ADEQUACY EARNING PER SHARE CLOSING SHARE PRICE 11.49% 11.03 510 0.31% 4.43 278 NO OF EMPLOYEES NO OF BRANCHES/ATM NO OF ACCOUNTS 445 51/61* 2,50,000 5 2/4 16% (* Currently Bank has 53 brances & 64 ATMs) (M = million) 4 Sunrise Bank Limited Seventh Annual Report 2013/14 CHAIRMAN MESSAGE Dear Shareholders, With the increased market competition as well as I am privileged to welcome all our distinguished bargaining power of customers and compliance with shareholders, guest and stakeholders to the Seventh internal, national and international standards etc Annual General Meeting of Sunrise Bank Limited and it is evident that the bank will have to face several would like to present the Bank’s Annual Report for the challenges in the various aspects in the coming Financial Year 2013/14. -

12Th Annual Report 075/076
12th Annual Report 075/076 ljifo–;"rL != afx|f}+ ;fwf/0f ;ef ;DaGwL ;"rgf ! @= ;fwf/0f;ef ;DaGwL ;fdfGo hfgsf/Lx? @ #= k|f]S;L kmf/d tyf k|j]zkq # $= ;+rfns ;ldltsf] cWoIfsf] k|ltj]bg % %= ;+rfns ;ldltaf6 k|:t't cf=j= @)&%÷&^ sf] k|ltj]bg & ^= sDkgL P]g @)^# sf] bkmf !)( cg';f/sf] cltl/Qm ljj/0f !@ &= lwtf]kq btf{ tyf lgisfzg lgodfjnL, @)&# sf] lgod @^ sf] pklgod @ ;Fu ;DalGwt cg';"rL !% adf]lhdsf] jflif{s ljj/0f !$ *= n]vfkl/Ifssf] k|ltj]bg !% (= ljQLo cj:yfsf] ljj/0f -jf;nft_ !& !)= gfkmf gf]S;fg ljj/0f !* !!= cGo lj:t[t cfDbfgLsf] ljj/0f !( !@= OlSj6Ldf ePsf] kl/jt{gsf] ljj/0f @) !#= gub k|jfx ljj/0f @@ !$= k|d'v n]vf gLltx? tyf n]vf ;DaGwL l6Kk0fLx? @$ !%= ljlQo ljj/0fsf cg';"rLx? $! !^= Basel III pb\3f]if0f / cGo ljj/0fx? ^$ !&= )=%Ü eGbf dfly z]o/ ePsf z]o/wgLx?sf] ;"rL *) !*= n]vfkl/If0f gePsf] ljQLo ljj/0f *! !(= n]vfkl/If0f gePsf] / n]vfkl/If0f kl5sf] t'ngfTds ljQLo ljj/0f *$ @)= ljQLo ;"rsf+sx? *^ @!= g]kfn /fi6« a+}ssf] :jLs[lt kq *& @@= k|aGwkq / lgodfjnL ;+zf]wgsf] tLg dxn] ljj/0f ** 12th Annual Report 075/076 12th Annual Report 075/076 s]Gb|Lo sfof{noM sdnkf]v/L, sf7df8f}+} sf] afx|f}+ jflif{s ;fwf/0f;ef ;DaGwL ;"rgf ldlt @)&^÷)(÷)# -tb\g';f/ !( l8;]Dj/, @)!(_ ut] a;]sf] ;+rfns ;ldltsf] #*& cf}+ a}7ssf] lg0f{ofg';f/ o; a}+ssf] afx|f}+ aflif{s ;fwf/0f;ef lgDg lnlvt ldlt, :yfg / ;dodf lgDg ljifox¿ pk/ 5nkmn tyf lg0f{o ug{ a:g] ePsf] x'“bf cfb/0fLo ;Dk"0f{ z]o/wgL dxfg'efjx¿sf] pkl:yltsf]nflu cg'/f]w ub{5' . -

Food Act, 2023 (1967)
Food Act, 2023 (1967) Date of Royal Seal and Publication 2023.5.24 (9 September 1967) The Amending Acts: 1. The Food (First Amendment) Act, 2030 (1973) 2030.12.23 (5 April 1970) 2. The Administration of Justice Act, 2048 (1991) 2048.2.16 (30 May 1991) 3. The Food (Second Amendment) Act, 2048 (1991) 2048.2.21 (3 June 1992) 4. The Food (Third Amendment) Act, 2049 (1992) 2049.7.6 (22 October 1992) An Act Made to Maintain Purity in Food Preamble: Whereas, it is expedient to make legal provisions so as to prevent any undesirable adulteration in food or subtraction or extraction of any natural quality or utility from food and keep on proper standards of food, for the purpose of maintaining the health and convenience of the general public; Now therefore, His Majesty King Mahendra Bir Bikram Shah Dev has enacted this law on the advice and with the approval of the National Panchayat, enacted this Act. 1. Short Title, Extent and Commencement 1. This Act may be cited as the "Food Act, 2023 (1967)" 2. It shall come into force in such area and on such date as His Majesty's Government may, by notification in the Nepal Gazette, appoint. 2. Definitions Unless the subject or the context otherwise requires, in this Act: a. "food" means any unprocessed, semi-processed, processed or produced food or drinking substance which the human being generally consumes and drinks, and includes any species, food additives, color or flavor to be used in any food or drinking substance. b. "adulterated food" means any food in any of the following conditions: 1. -
TOGETHER, WE CAN BUILD. We Make Commitments, Take Responsibilities, Promote Trust and Build Partnership; Summing up We Can Say, “YOU & US TOGETHER, WE CAN BUILD”
ANNUAL REPORT 2015-16 TOGETHER, WE CAN BUILD. We make commitments, take responsibilities, promote trust and build partnership; summing up we can say, “YOU & US TOGETHER, WE CAN BUILD”. Through our best governance, disciplined management, talented and skilled human resources, a customer oriented approach and robust infrastructure, we have been successful to deliver the services smoothly and achieve our growth year on year. We believe in being available to you all times. Because, if “you and us” work together, we can build a better future. FORWARD-LOOKING STATEMENTS The Annual Report for the year 2015/16 presented hereby shows the growth we made from the inception. This achievement is the result of the support from all the stakeholders. Please have a look at our Bank, the driving force, Management Team, products and services we offer, our present growth and the achievements. 2 SUNRISE BANK LIMITED ANNUAL REPORT 2015-16 ANNUAL REPORT 2015/16 3 Report Objectives The report is intended to provide simplified information to our stakeholders as well as other interested parties on how we performed in 2015/16. The report is a reflection on the overall operation of the Bank and exhibits the Bank’s direction to achieve its mission and vision. The Annual Report Sunrise Bank The Bank Global growth, On behalf of the The Bank has Capitalizing on its core strength, The Board comprises Limited, a leading performance this year currently estimated at Board of Directors of performed significantly of a Chairman, four market orientation and innovation in Commercial Bank of was remarkable; 3.1 percent in 2015, your company, well during the fiscal year Directors from promoter’s Nepal.. -
Tender List of Baisakh 2076
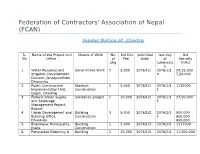
Federation of Contractors' Association of Nepal (FCAN) Tender Notice of Chaitra S. Name of the Project and Nature of Work No. Bid Doc published last day Bid No Office of Fee date: of Security pkg submissio (NRs) n 1. Water Resource and Canal Intake Work 2 5,000 2076/1/1 2076/1/3 24,25,000 irrigation Development 0 7,20,000 Davison, Janakpurdham, Dhanusha 2. Public Construction Stadium 1 5,000 2076/1/1 2076/1/3 1132000 Implementation Unit, Construction 1 Gajuri, Dhading 3. Federal Water Supply Sanitation project 1 10,000 2076/1/2 2076/1/3 27,00,000 and Sewerage 1 Management Project, Butwal 4. Urban Development and Building 3 5,000 2076/1/2` 2076/1/3 800,000 Building Office, Construction 1 850,000 Dhankuta 800,000 5. Bhadrapur Municipality, Building 1 5,000 2076/1/3 2076/2/2 1517500 Jhapa Construction 6. Paroparkat Maternity & Building 1 20,000 2076/1/3 2076/2/2 11,500,000 Womens Hospital Construction 7. Infrastructure Road Construction 1 10,000 2076/1/3 2076/2/2 40,00,000 Development Office, Kaski 8. Chhatreshwori Rural Water Supply 1 5,000 2076/1/3 2076/2/2 514960 Municipality, Project Bhotechaur, Salyan 9. Federal project Building 6 5,000 2076/1/3 2076/2/2 13,70,000 Implementation Unit, Construction (2) Surkhet 10,10,000 6,40,000 3,50,000 21,00,000 10. Urban Development Building 11 5,000 2076/1/4 2076/2/3 --------------- Bulding Office, Morang, Construction - Biratnagar 11. -

S.N Local Government Bodies EN स्थानीय तहको नाम NP District
S.N Local Government Bodies_EN थानीय तहको नाम_NP District LGB_Type Province Website 1 Fungling Municipality फु ङलिङ नगरपालिका Taplejung Municipality 1 phunglingmun.gov.np 2 Aathrai Triveni Rural Municipality आठराई त्रिवेणी गाउँपालिका Taplejung Rural municipality 1 aathraitribenimun.gov.np 3 Sidingwa Rural Municipality लिदिङ्वा गाउँपालिका Taplejung Rural municipality 1 sidingbamun.gov.np 4 Faktanglung Rural Municipality फक्ताङिुङ गाउँपालिका Taplejung Rural municipality 1 phaktanglungmun.gov.np 5 Mikhwakhola Rural Municipality लि啍वाखोिा गाउँपालिका Taplejung Rural municipality 1 mikwakholamun.gov.np 6 Meringden Rural Municipality िेररङिेन गाउँपालिका Taplejung Rural municipality 1 meringdenmun.gov.np 7 Maiwakhola Rural Municipality िैवाखोिा गाउँपालिका Taplejung Rural municipality 1 maiwakholamun.gov.np 8 Yangworak Rural Municipality याङवरक गाउँपालिका Taplejung Rural municipality 1 yangwarakmuntaplejung.gov.np 9 Sirijunga Rural Municipality लिरीजङ्घा गाउँपालिका Taplejung Rural municipality 1 sirijanghamun.gov.np 10 Fidhim Municipality दफदिि नगरपालिका Panchthar Municipality 1 phidimmun.gov.np 11 Falelung Rural Municipality फािेिुुंग गाउँपालिका Panchthar Rural municipality 1 phalelungmun.gov.np 12 Falgunanda Rural Municipality फा쥍गुनन्ि गाउँपालिका Panchthar Rural municipality 1 phalgunandamun.gov.np 13 Hilihang Rural Municipality दिलििाङ गाउँपालिका Panchthar Rural municipality 1 hilihangmun.gov.np 14 Kumyayek Rural Municipality कु म्िायक गाउँपालिका Panchthar Rural municipality 1 kummayakmun.gov.np 15 Miklajung Rural Municipality लि啍िाजुङ गाउँपालिका -

Cfreptiles & Amphibians
HTTPS://JOURNALS.KU.EDU/REPTILESANDAMPHIBIANSTABLE OF CONTENTS IRCF REPTILES & AMPHIBIANSREPTILES • VOL &15, AMPHIBIANS NO 4 • DEC 2008 • 28(1):182–184189 • APR 2021 IRCF REPTILES & AMPHIBIANS CONSERVATION AND NATURAL HISTORY TABLEHUSBANDRY OF CONTENTS FEATURE ARTICLES . Chasing Bullsnakes (Pituophis catenifer sayi) in Wisconsin: OnHatching the Road to Understanding the Ecology Buff-striped and Conservation of the Midwest’s Giant Serpent Keelback ...................... Joshua M. Kapfer 190 . The Shared History of Treeboas (Corallus grenadensis) and Humans on Grenada: A Hypothetical Excursion(Amphiesma ............................................................................................................................ stolatum)Robert W. Henderson 198 RESEARCH ARTICLES . The EggsTexas Horned Lizard in in Central a and WesternHome-made Texas ....................... Emily Henry, Jason Brewer,Incubator Krista Mougey, and Gad Perry 204 . The Knight Anole (Anolis equestris) in Florida .............................................Brian J. Camposano,Tapil P. Kenneth Rai1,2 L. andKrysko, Sabin Kevin M.Adhikari Enge, Ellen3 M. Donlan, and Michael Granatosky 212 CONSERVATION1Turtle Rescue and Conservation ALERT Centre (TRCC), Arjundhara Municipality-9, Jhapa, Nepal ([email protected]) 2Department of Environmental Science, Mechi Multiple Campus, Bhadrapur Municipality-8, Jhapa, Nepal . World’s Mammals in Crisis ............................................................................................................................................................ -

Food Act, 2023 (1967) Date of Authentication 2023.5.24 (9 September 1966 Amendments 1
www.lawcommission.gov.np Food Act, 2023 (1967) Date of Authentication 2023.5.24 (9 September 1966 Amendments 1. Food (First Amendment) Act, 2030 (1974) 2030.12.11 (24 March 1974) 2. Administration of Justice Act, 2048 (1991) 2048.2.16 (30 May 1991 ) 3. Food ( Second Amendment) Act, 1991 2048.2.21 (4 June 1991) 4. Food (Third Amendment) Act, 1992 2049.7.6 (22 October 1992) Act No. 8 of the year, 2052 (1966) An Act made to maintain purity in foodstuffs Preamble : Whereas, it is expedient to make legal provisions to maintain proper standard of foodstuffs and to prevent any undesirable adulteration in foodstuffs or prevent from reducing in, or extracting, any natural quality or utility from foodstuffs in order to maintain health and convenience of the general public; Be it enacted by His Majesty the King Mahendra Bir Bikram Shah Dev has enacted this Act on the advice and with the consent of the Rastriya Panchayat. 1. Short title, extent and commencement: (1) This Act may be called as the "Food Act, 1966" (2) This Act shall come into force in such area and on such date as the Government of Nepal may, by notification published in the Nepal Gazette, appoint. * 2. Definition : Unless the subject or context otherwise requires, in this Acts,- (a) "foodstuffs" means the produced, processed, semi-processed or raw foodstuffs or drinks which human beings generally consume or drink and this word also includes the spices, food additives, colour or aroma to be used in foodstuffs or drinks. * Amended by the third amendment. -

Table of Province 01, Preliminary Results, Nepal Economic Census 2018
Number of Number of Persons Engaged District and Local Unit establishments Total Male Female Taplejung District 4,653 13,225 7,337 5,888 10101PHAKTANLUNG RURAL MUNICIPALITY 539 1,178 672 506 10102MIKWAKHOLA RURAL MUNICIPALITY 269 639 419 220 10103MERINGDEN RURAL MUNICIPALITY 397 1,125 623 502 10104MAIWAKHOLA RURAL MUNICIPALITY 310 990 564 426 10105AATHARAI TRIBENI RURAL MUNICIPALITY 433 1,770 837 933 10106PHUNGLING MUNICIPALITY 1,606 4,832 3,033 1,799 10107PATHIBHARA RURAL MUNICIPALITY 398 1,067 475 592 10108SIRIJANGA RURAL MUNICIPALITY 452 1,064 378 686 10109SIDINGBA RURAL MUNICIPALITY 249 560 336 224 Sankhuwasabha District 6,037 18,913 9,996 8,917 10201BHOTKHOLA RURAL MUNICIPALITY 294 989 541 448 10202MAKALU RURAL MUNICIPALITY 437 1,317 666 651 10203SILICHONG RURAL MUNICIPALITY 401 1,255 567 688 10204CHICHILA RURAL MUNICIPALITY 199 586 292 294 10205SABHAPOKHARI RURAL MUNICIPALITY 220 751 417 334 10206KHANDABARI MUNICIPALITY 1,913 6,024 3,281 2,743 10207PANCHAKHAPAN MUNICIPALITY 590 1,732 970 762 10208CHAINAPUR MUNICIPALITY 1,034 3,204 1,742 1,462 10209MADI MUNICIPALITY 421 1,354 596 758 10210DHARMADEVI MUNICIPALITY 528 1,701 924 777 Solukhumbu District 3,506 10,073 5,175 4,898 10301 KHUMBU PASANGLHAMU RURAL MUNICIPALITY 702 1,906 904 1,002 10302MAHAKULUNG RURAL MUNICIPALITY 369 985 464 521 10303SOTANG RURAL MUNICIPALITY 265 787 421 366 10304DHUDHAKOSHI RURAL MUNICIPALITY 263 802 416 386 10305 THULUNG DHUDHA KOSHI RURAL MUNICIPALITY 456 1,286 652 634 10306NECHA SALYAN RURAL MUNICIPALITY 353 1,054 509 545 10307SOLU DHUDHAKUNDA MUNICIPALITY -

Nepal Water Supply Corporation Water Supply Hour of Different Branches
Nepal Water Supply Corporation Water Supply hour of Different Branches 1.Branch Name: Taulihawa Branch Water Supply Supply hour S.N. Place Remarks. Area Morning Day Evening 1 Taulihawa Kapilbastu Municipality 5:00 to 8:00 5:00 to7:00 2.Branch Name: Dharan Branch Water Supply Supply hour S.N. Place Remarks. Area Morning Day Evening 1 Dharan Dharan Municipality Ward no. 04 2:00 to 5:00 Ward no. 12 2:00 to 5:00 Ward no. 13 2:00 to 5:00 Ward no. 13 2:00 to 5:00 Ward no. 15 2:00 to 5:00 Ward no. 16 2:00 to 5:00 Other remaining wards 2:00 to 6:00 2:00 to 5:00 3.Branch Name: Bhairahawa Branch Water Supply Supply hour S.N. Place Remarks. Area Morning Day Evening 1 Bhairahawa Siddhartha nagar Municipality 5:00 to 9:00 12:00 to 1:00 5:00 to7:00 4.Branch Name: Gaur Branch Water Supply Supply hour S.N. Place Remarks. Area Morning Day Evening 1 Gaur Gaur Municipality 5:00 to 9:30 12:00 to 1:30 6:00 to 9:00 5.Branch Name: Biratnagar Branch Water Supply Supply hour S.N. Place Remarks. Area Morning Day Evening Biratnagar Sub Metropolitan 1 Biratnagar city Devkota Pump station 4:00 to 9:00 12:00 to 2:00 5:00 to 9:00 Tinpani pump Station 4:00 to 9:00 12:00 to 2:00 5:00 to 9:00 Munalpath pump satation 4:00 to 10:00 12:00 to 2:00 3:00 to 10:00 6.Branch Name: Krishnanagar Branch Water Supply Supply hour S.N. -

Saath-Saath Project
Saath-Saath Project Saath-Saath Project THIRD ANNUAL REPORT August 2013 – July 2014 September 2014 0 Submitted by Saath-Saath Project Gopal Bhawan, Anamika Galli Baluwatar – 4, Kathmandu Nepal T: +977-1-4437173 F: +977-1-4417475 E: [email protected] FHI 360 Nepal USAID Cooperative Agreement # AID-367-A-11-00005 USAID/Nepal Country Assistance Objective Intermediate Result 1 & 4 1 Table of Contents List of Acronyms .................................................................................................................................................i Executive Summary ............................................................................................................................................ 1 I. Introduction ........................................................................................................................................... 4 II. Program Management ........................................................................................................................... 6 III. Technical Program Elements (Program by Outputs) .............................................................................. 6 Outcome 1: Decreased HIV prevalence among selected MARPs ...................................................................... 6 Outcome 2: Increased use of Family Planning (FP) services among MARPs ................................................... 9 Outcome 3: Increased GON capacity to plan, commission and use SI ............................................................ 14 Outcome