Systemic Sclerosis/Scleroderma: a Treatable Multisystem Disease
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Understanding and Managing Scleroderma
Understanding and Managing Scleroderma A publication of Scleroderma Foundation 300 Rosewood Drive, Suite 105 Danvers, MA 01923 Maureen D. Mayes, M.D., M.P.H. Understanding and Understanding My notes and Managing Scleroderma Managing Scleroderma This booklet is intended to help people with scleroderma, their families and others interested ________________________ in learning more about the disease to better understand what scleroderma is, what effects ________________________ it may have, and what those with scleroderma can do to help themselves and their physicians ________________________ manage the disease. It answers some of the most frequently asked questions about ________________________ A publication of Maureen D. Mayes, M.D., M.P.H. Scleroderma Foundation 300 Rosewood Drive, Suite 105 scleroderma. Danvers, MA 01923 800-722-HOPE (4673) www.scleroderma.org www.facebook.com/sclerodermaUS www.twitter.com/scleroderma ________________________ Disclaimer The Scleroderma Foundation does not provide medical advice nor does it ________________________ endorse any drug or treatment mentioned herein. ________________________ The material contained in this booklet is presented for general information only. It is not intended to provide medical advice, to answer questions specific to the condition or problems of particular individuals, nor in ________________________ any way to substitute for the professional advice and care of qualified physicians. Mention of particular drugs and/or treatments is for ________________________ information purposes only and does not constitute an endorsement of said drugs and/or treatments. ________________________ Thanks! ________________________ The Scleroderma Foundation expresses its deep appreciation to the many ________________________ physicians whose efforts have led to this booklet. Special thanks are owed to Maureen D. Mayes, M.D., M.P.H., of the ________________________ University of Texas McGovern Medical School, Houston. -

The Voice of the Patient
The Voice of the Patient A series of reports from the U.S. Food and Drug Administration’s (FDA’s) Patient-Focused Drug Development Initiative Systemic Sclerosis Public Meeting: October 13, 2020 Report Date: June 30, 2021 Center for Drug Evaluation and Research (CDER) U.S. Food and Drug Administration (FDA) 1 Table of Contents Introduction ............................................................................................................................ 3 Overview of Systemic Sclerosis ................................................................................................................. 3 Meeting Overview ..................................................................................................................................... 3 Report Overview and Key Themes ............................................................................................................ 5 Topic 1: Disease Symptoms and Daily Impacts That Matter Most to Patients .......................... 6 Perspectives on Most Significant Symptoms ............................................................................................ 6 Overall Impact of Systemic Sclerosis on Daily Life .................................................................................... 9 Topic 2: Patient Perspectives on Treatments for Systemic Sclerosis ....................................... 11 Perspectives on Current Treatments ...................................................................................................... 11 Perspectives on Ideal -

Visual Recognition of Autoimmune Connective Tissue Diseases
Seeing the Signs: Visual Recognition of Autoimmune Connective Tissue Diseases Utah Association of Family Practitioners CME Meeting at Snowbird, UT 1:00-1:30 pm, Saturday, February 13, 2016 Snowbird/Alta Rick Sontheimer, M.D. Professor of Dermatology Univ. of Utah School of Medicine Potential Conflicts of Interest 2016 • Consultant • Paid speaker – Centocor (Remicade- – Winthrop (Sanofi) infliximab) • Plaquenil – Genentech (Raptiva- (hydroxychloroquine) efalizumab) – Amgen (etanercept-Enbrel) – Alexion (eculizumab) – Connetics/Stiefel – MediQuest • Royalties Therapeutics – Lippincott, – P&G (ChelaDerm) Williams – Celgene* & Wilkins* – Sanofi/Biogen* – Clearview Health* Partners • 3Gen – Research partner *Active within past 5 years Learning Objectives • Compare and contrast the presenting and Hallmark cutaneous manifestations of lupus erythematosus and dermatomyositis • Compare and contrast the presenting and Hallmark cutaneous manifestations of morphea and systemic sclerosis Distinguishing the Cutaneous Manifestations of LE and DM Skin involvement is 2nd most prevalent clinical manifestation of SLE and 2nd most common presenting clinical manifestation Comprehensive List of Skin Lesions Associated with LE LE-SPECIFIC LE-NONSPECIFIC Cutaneous vascular disease Acute Cutaneous LE Vasculitis Leukocytoclastic Localized ACLE Palpable purpura Urticarial vasculitis Generalized ACLE Periarteritis nodosa-like Ten-like ACLE Vasculopathy Dego's disease-like Subacute Cutaneous LE Atrophy blanche-like Periungual telangiectasia Annular Livedo reticularis -

A Review of the Evidence for and Against a Role for Mast Cells in Cutaneous Scarring and Fibrosis
International Journal of Molecular Sciences Review A Review of the Evidence for and against a Role for Mast Cells in Cutaneous Scarring and Fibrosis Traci A. Wilgus 1,*, Sara Ud-Din 2 and Ardeshir Bayat 2,3 1 Department of Pathology, Ohio State University, Columbus, OH 43210, USA 2 Centre for Dermatology Research, NIHR Manchester Biomedical Research Centre, Plastic and Reconstructive Surgery Research, University of Manchester, Manchester M13 9PT, UK; [email protected] (S.U.-D.); [email protected] (A.B.) 3 MRC-SA Wound Healing Unit, Division of Dermatology, University of Cape Town, Observatory, Cape Town 7945, South Africa * Correspondence: [email protected]; Tel.: +1-614-366-8526 Received: 1 October 2020; Accepted: 12 December 2020; Published: 18 December 2020 Abstract: Scars are generated in mature skin as a result of the normal repair process, but the replacement of normal tissue with scar tissue can lead to biomechanical and functional deficiencies in the skin as well as psychological and social issues for patients that negatively affect quality of life. Abnormal scars, such as hypertrophic scars and keloids, and cutaneous fibrosis that develops in diseases such as systemic sclerosis and graft-versus-host disease can be even more challenging for patients. There is a large body of literature suggesting that inflammation promotes the deposition of scar tissue by fibroblasts. Mast cells represent one inflammatory cell type in particular that has been implicated in skin scarring and fibrosis. Most published studies in this area support a pro-fibrotic role for mast cells in the skin, as many mast cell-derived mediators stimulate fibroblast activity and studies generally indicate higher numbers of mast cells and/or mast cell activation in scars and fibrotic skin. -

Genes in Eyecare Geneseyedoc 3 W.M
Genes in Eyecare geneseyedoc 3 W.M. Lyle and T.D. Williams 15 Mar 04 This information has been gathered from several sources; however, the principal source is V. A. McKusick’s Mendelian Inheritance in Man on CD-ROM. Baltimore, Johns Hopkins University Press, 1998. Other sources include McKusick’s, Mendelian Inheritance in Man. Catalogs of Human Genes and Genetic Disorders. Baltimore. Johns Hopkins University Press 1998 (12th edition). http://www.ncbi.nlm.nih.gov/Omim See also S.P.Daiger, L.S. Sullivan, and B.J.F. Rossiter Ret Net http://www.sph.uth.tmc.edu/Retnet disease.htm/. Also E.I. Traboulsi’s, Genetic Diseases of the Eye, New York, Oxford University Press, 1998. And Genetics in Primary Eyecare and Clinical Medicine by M.R. Seashore and R.S.Wappner, Appleton and Lange 1996. M. Ridley’s book Genome published in 2000 by Perennial provides additional information. Ridley estimates that we have 60,000 to 80,000 genes. See also R.M. Henig’s book The Monk in the Garden: The Lost and Found Genius of Gregor Mendel, published by Houghton Mifflin in 2001 which tells about the Father of Genetics. The 3rd edition of F. H. Roy’s book Ocular Syndromes and Systemic Diseases published by Lippincott Williams & Wilkins in 2002 facilitates differential diagnosis. Additional information is provided in D. Pavan-Langston’s Manual of Ocular Diagnosis and Therapy (5th edition) published by Lippincott Williams & Wilkins in 2002. M.A. Foote wrote Basic Human Genetics for Medical Writers in the AMWA Journal 2002;17:7-17. A compilation such as this might suggest that one gene = one disease. -

Foot Pain in Scleroderma
Foot Pain in Scleroderma Dr Begonya Alcacer-Pitarch LMBRU Postdoctoral Research Fellow 20th Anniversary Scleroderma Family Day 16th May 2015 Leeds Institute of Rheumatic and Musculoskeletal Medicine Presentation Content n Introduction n Different types of foot pain n Factors contributing to foot pain n Impact of foot pain on Quality of Life (QoL) Leeds Institute of Rheumatic and Musculoskeletal Medicine Scleroderma n Clinical features of scleroderma – Microvascular (small vessel) and macrovascular (large vessel) damage – Fibrosis of the skin and internal organs – Dysfunction of the immune system n Unknown aetiology n Female to male ratio 4.6 : 1 n The prevalence of SSc in the UK is 8.21 per 100 000 Leeds Institute of Rheumatic and Musculoskeletal Medicine Foot Involvement in SSc n Clinically 90% of SSc patients have foot involvement n It typically has a later involvement than hands n Foot involvement is less frequent than hand involvement, but is potentially disabling Leeds Institute of Rheumatic and Musculoskeletal Medicine Different Types of Foot Pain Leeds Institute of Rheumatic and Musculoskeletal Medicine Ischaemic Pain (vascular) Microvascular disease (small vessel) n Intermittent pain – Raynaud’s (spasm) • Cold • Throb • Numb • Tingle • Pain n Constant pain – Vessel center narrows • Distal pain (toes) • Gradually increasing pain • Intolerable pain when necrosis is present Leeds Institute of Rheumatic and Musculoskeletal Medicine Ischaemic Pain (vascular) Macrovascular disease (large vessels) n Intermittent and constant pain – Peripheral Arterial Disease • Intermittent claudication – Muscle pain (ache, cramp) during walking • Aching or burning pain • Night and rest pain • Cramps Leeds Institute of Rheumatic and Musculoskeletal Medicine Ulcer Pain n Ulcer development – Constant pain n Infected ulcer – Unexpected/ excess pain or tenderness Leeds Institute of Rheumatic and Musculoskeletal Medicine Neuropathic Pain n Nerve damage is not always obvious. -

The Articular Manifestations of Progressive Systemic Sclerosis (Scleroderma) MURRAY BARON, PETER LEE, and EDWARD C
Ann Rheum Dis: first published as 10.1136/ard.41.2.147 on 1 April 1982. Downloaded from Annals ofthe Rheumatic Diseases, 1982, 41, 147-152 The articular manifestations of progressive systemic sclerosis (scleroderma) MURRAY BARON, PETER LEE, AND EDWARD C. KEYSTONE From the University of Toronto Rheumatic Disease Unit, The Wellesley Hospital, 160 Wellesley Street East, Toronto, Ontario, Canada M4Y 1J3 SUMMARY The articular manifestations of progressive systemic sclerosis (PSS) were studied in 38 patients. Of these, 66 % experienced joint pain and 61 % had signs of joint inflammation. Limita- tion of joint movement was seen in 45 %. Radiological abnormalities included periarticular osteoporosis (42 %), joint space narrowing (34%), and erosions (40%). Erosive disease did not correlate with disease duration, presence of rheumatoid factor, antinuclear antibodies, distal tuft resorption, or the extent of the scleroderma skin changes. Calcinosis was seen more frequently in those patients with articular erosions (67 %). Erosive osteoarthritis of the distal interphalangeal joints (7 patients) was associated with impaired finger flexion. Joint involvement in PSS occurs frequently and may resemble rheumatoid arthritis in the early stages but is less destructive. The occurrence of unrelated arthropathy, such as primary osteoarthritis, is not uncommon, and its differentiation from true PSS joint disease can be difficult. Articular manifestations are common in progressive spective study and fulfilling the preliminary diagnos- systemic sclerosis (scleroderma, PSS), and joint pain tic criteria for PSS1 were evaluated by one author is a frequent presenting feature of this disease.' Joint (M.B.). A history of joint manifestations was symptoms have been noted in 12 to 66% of patients obtained in each case according to a standard pro- http://ard.bmj.com/ at the time of diagnosis2`6 and in 24 to 97% of tocol. -

Scleroderma Phenotype'' This Information Is Current As of September 27, 2021
Autoantibodies to Fibrillin-1 Activate Normal Human Fibroblasts in Culture through the TGF-β Pathway to Recapitulate the ''Scleroderma Phenotype'' This information is current as of September 27, 2021. Xiaodong Zhou, Filemon K. Tan, Dianna M. Milewicz, Xinjian Guo, Constantin A. Bona and Frank C. Arnett J Immunol 2005; 175:4555-4560; ; doi: 10.4049/jimmunol.175.7.4555 http://www.jimmunol.org/content/175/7/4555 Downloaded from References This article cites 32 articles, 11 of which you can access for free at: http://www.jimmunol.org/content/175/7/4555.full#ref-list-1 http://www.jimmunol.org/ Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication by guest on September 27, 2021 *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2005 by The American Association of Immunologists All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. The Journal of Immunology Autoantibodies to Fibrillin-1 Activate Normal Human Fibroblasts in Culture through the TGF- Pathway to Recapitulate the “Scleroderma Phenotype”1 Xiaodong Zhou,2* Filemon K. Tan,* Dianna M. -

Prevalence and Incidence of Rare Diseases: Bibliographic Data
Number 1 | January 2019 Prevalence and incidence of rare diseases: Bibliographic data Prevalence, incidence or number of published cases listed by diseases (in alphabetical order) www.orpha.net www.orphadata.org If a range of national data is available, the average is Methodology calculated to estimate the worldwide or European prevalence or incidence. When a range of data sources is available, the most Orphanet carries out a systematic survey of literature in recent data source that meets a certain number of quality order to estimate the prevalence and incidence of rare criteria is favoured (registries, meta-analyses, diseases. This study aims to collect new data regarding population-based studies, large cohorts studies). point prevalence, birth prevalence and incidence, and to update already published data according to new For congenital diseases, the prevalence is estimated, so scientific studies or other available data. that: Prevalence = birth prevalence x (patient life This data is presented in the following reports published expectancy/general population life expectancy). biannually: When only incidence data is documented, the prevalence is estimated when possible, so that : • Prevalence, incidence or number of published cases listed by diseases (in alphabetical order); Prevalence = incidence x disease mean duration. • Diseases listed by decreasing prevalence, incidence When neither prevalence nor incidence data is available, or number of published cases; which is the case for very rare diseases, the number of cases or families documented in the medical literature is Data collection provided. A number of different sources are used : Limitations of the study • Registries (RARECARE, EUROCAT, etc) ; The prevalence and incidence data presented in this report are only estimations and cannot be considered to • National/international health institutes and agencies be absolutely correct. -

Systemic Scleroderma
Systemic scleroderma Description Systemic scleroderma is an autoimmune disorder that affects the skin and internal organs. Autoimmune disorders occur when the immune system malfunctions and attacks the body's own tissues and organs. The word "scleroderma" means hard skin in Greek, and the condition is characterized by the buildup of scar tissue (fibrosis) in the skin and other organs. The condition is also called systemic sclerosis because the fibrosis can affect organs other than the skin. Fibrosis is due to the excess production of a tough protein called collagen, which normally strengthens and supports connective tissues throughout the body. The signs and symptoms of systemic scleroderma usually begin with episodes of Raynaud phenomenon, which can occur weeks to years before fibrosis. In Raynaud phenomenon, the fingers and toes of affected individuals turn white or blue in response to cold temperature or other stresses. This effect occurs because of problems with the small vessels that carry blood to the extremities. Another early sign of systemic scleroderma is puffy or swollen hands before thickening and hardening of the skin due to fibrosis. Skin thickening usually occurs first in the fingers (called sclerodactyly) and may also involve the hands and face. In addition, people with systemic scleroderma often have open sores (ulcers) on their fingers, painful bumps under the skin (calcinosis) , or small clusters of enlarged blood vessels just under the skin (telangiectasia). Fibrosis can also affect internal organs and can lead to impairment or failure of the affected organs. The most commonly affected organs are the esophagus, heart, lungs, and kidneys. Internal organ involvement may be signaled by heartburn, difficulty swallowing (dysphagia), high blood pressure (hypertension), kidney problems, shortness of breath, diarrhea, or impairment of the muscle contractions that move food through the digestive tract (intestinal pseudo-obstruction). -
Eosinophilic Fasciitis (Shulman Syndrome)
CONTINUING MEDICAL EDUCATION Eosinophilic Fasciitis (Shulman Syndrome) Sueli Carneiro, MD, PhD; Arles Brotas, MD; Fabrício Lamy, MD; Flávia Lisboa, MD; Eduardo Lago, MD; David Azulay, MD; Tulia Cuzzi, MD, PhD; Marcia Ramos-e-Silva, MD, PhD GOAL To understand eosinophilic fasciitis to better manage patients with the condition OBJECTIVES Upon completion of this activity, dermatologists and general practitioners should be able to: 1. Recognize the clinical presentation of eosinophilic fasciitis. 2. Discuss the histologic findings in patients with eosinophilic fasciitis. 3. Differentiate eosinophilic fasciitis from similarly presenting conditions. CME Test on page 215. This article has been peer reviewed and is accredited by the ACCME to provide continuing approved by Michael Fisher, MD, Professor of medical education for physicians. Medicine, Albert Einstein College of Medicine. Albert Einstein College of Medicine designates Review date: March 2005. this educational activity for a maximum of 1 This activity has been planned and implemented category 1 credit toward the AMA Physician’s in accordance with the Essential Areas and Policies Recognition Award. Each physician should of the Accreditation Council for Continuing Medical claim only that credit that he/she actually spent Education through the joint sponsorship of Albert in the activity. Einstein College of Medicine and Quadrant This activity has been planned and produced in HealthCom, Inc. Albert Einstein College of Medicine accordance with ACCME Essentials. Drs. Carneiro, Brotas, Lamy, Lisboa, Lago, Azulay, Cuzzi, and Ramos-e-Silva report no conflict of interest. The authors report no discussion of off-label use. Dr. Fisher reports no conflict of interest. We present a case of eosinophilic fasciitis, or Shulman syndrome apart from all other sclero- Shulman syndrome, in a 35-year-old man and dermiform states. -
Nodular Morphea
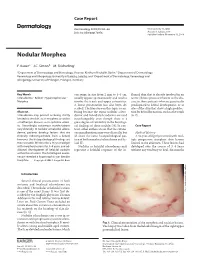
Case Report Dermatology 2009;218:63–66 Received: July 13, 2008 DOI: 10.1159/000173976 Accepted: July 23, 2008 Published online: November 13, 2008 Nodular Morphea a b c F. Kauer J.C. Simon M. Sticherling a b Department of Dermatology and Venerology, Vivantes Klinikum Neukölln, Berlin , Department of Dermatology, c Venerology and Allergology, University of Leipzig, Leipzig , and Department of Dermatology, Venerology and Allergology, University of Erlangen, Erlangen , Germany Key Words can range in size from 2 mm to 4–5 cm, flamed skin that is already involved in an -Scleroderma ؒ Keloid ؒ Hypertrophic scar ؒ usually appear spontaneously and tend to active fibrotic process inherent to the dis Morphea involve the trunk and upper extremities. ease in those patients who are genetically A linear presentation has also been de- predisposed to keloid development, or at scribed. The literature on this topic is con- sites of the skin that show a high predilec- Abstract fusing because the terms ‘nodular sclero- tion for keloid formation, such as the trunk Scleroderma may present as being strictly derma’ and ‘keloidal scleroderma’ are used [6, 7] . limited to the skin, as in morphea, or within interchangeably even though there is a a multiorgan disease, as in systemic sclero- great degree of variability in the histologi- sis. Accordingly, cutaneous manifestations cal findings of these nodules [4] . In con- C a s e R e p o r t vary clinically. In nodular or keloidal sclero- trast, other authors stress that the cutane- derma, patients develop lesions that are ous manifestations may vary clinically, but Medical History clinically indistinguishable from a keloid; all share the same histopathological pat- A 16-year-old girl presented with mul- however, the histopathological findings are tern of both morphea/scleroderma and ke- tiple progressive morpheic skin lesions more variable.