Gene Expression Network Analysis of Lymph Node Involvement in Colon
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Mammalian Adult Neurogenesis Gene Ontology (MANGO) Provides a Structural Framework for Published Information on Genes Regulating Adult Hippocampal Neurogenesis
The Mammalian Adult Neurogenesis Gene Ontology (MANGO) Provides a Structural Framework for Published Information on Genes Regulating Adult Hippocampal Neurogenesis Rupert W. Overall1, Maciej Paszkowski-Rogacz2, Gerd Kempermann1,3* 1 CRTD – Center for Regenerative Therapies Dresden, Technische Universita¨t Dresden, Dresden, Germany, 2 UCC – University Cancer Center, Medical Faculty, Technische Universita¨t Dresden, Dresden, Germany, 3 DZNE, German Center for Neurodegenerative Diseases, Dresden, Germany Abstract Background: Adult hippocampal neurogenesis is not a single phenotype, but consists of a number of sub-processes, each of which is under complex genetic control. Interpretation of gene expression studies using existing resources often does not lead to results that address the interrelatedness of these processes. Formal structure, such as provided by ontologies, is essential in any field for comprehensive interpretation of existing knowledge but, until now, such a structure has been lacking for adult neurogenesis. Methodology/Principal Findings: We have created a resource with three components 1. A structured ontology describing the key stages in the development of adult hippocampal neural stem cells into functional granule cell neurons. 2. A comprehensive survey of the literature to annotate the results of all published reports on gene function in adult hippocampal neurogenesis (257 manuscripts covering 228 genes) to the appropriate terms in our ontology. 3. An easy-to- use searchable interface to the resulting database made freely available online. The manuscript presents an overview of the database highlighting global trends such as the current bias towards research on early proliferative stages, and an example gene set enrichment analysis. A limitation of the resource is the current scope of the literature which, however, is growing by around 100 publications per year. -

The Amyloid-Β Precursor Protein (App)-Binding Protein Fe65 and App Processing
! !"#$ #"%"" & '( ) ' *#+,% - . /0 - 1 2 /20 %2 3 2 /02 4 % 5 ' 64 ' 6% 7 1 +8 % +8 ' - /790' 4 %5 ': +8 ' 79: +8 1 %; +8 +<8 % = +8% ' +8 / 70' +8 - / 770% ' ;,! +8' == ' - +8/ 770%7 ' !!$ +8 : +8 / 7770%; ' 64 +8 - ' 6 +8 - / 777770%> ' 7? +<8 ' 6%; ' +<8 ' +<8 6 2% 7 +8 ' % ! !"#$ @:: %% : A B @@ @ @ #CDD"+ 7,D<$D#<<D<##!! 7,D<$D#<<D<##ED " # '#"+D# THE AMYLOID-Β PRECURSOR PROTEIN (APP)-BINDING PROTEIN FE65 AND APP PROCESSING Niina Koistinen The amyloid-β precursor protein (APP)-binding protein Fe65 and APP processing Niina Koistinen ©Niina Koistinen, Stockholm University 2018 ISBN print 978-91-7797-112-2 ISBN PDF 978-91-7797-113-9 Cover: An healthy and AD diseased brain half freely interpreted by Conrad, aged 9, and Cleo, aged 6 Printed in Sweden by Universitetsservice US-AB, Stockholm 2017 Distributor: Department of Neurochemistry, Stockholm University Till min familj List of Publications I. Koistinen NA, Bacanu S, Iverfeldt K Phosporylation of Fe65 amyloid precursor protein-binding protein in respons to neuronal differentiation Neuroscience Letters, 2016, Feb2;613:54-9 -

Whole Exome Sequencing in Families at High Risk for Hodgkin Lymphoma: Identification of a Predisposing Mutation in the KDR Gene
Hodgkin Lymphoma SUPPLEMENTARY APPENDIX Whole exome sequencing in families at high risk for Hodgkin lymphoma: identification of a predisposing mutation in the KDR gene Melissa Rotunno, 1 Mary L. McMaster, 1 Joseph Boland, 2 Sara Bass, 2 Xijun Zhang, 2 Laurie Burdett, 2 Belynda Hicks, 2 Sarangan Ravichandran, 3 Brian T. Luke, 3 Meredith Yeager, 2 Laura Fontaine, 4 Paula L. Hyland, 1 Alisa M. Goldstein, 1 NCI DCEG Cancer Sequencing Working Group, NCI DCEG Cancer Genomics Research Laboratory, Stephen J. Chanock, 5 Neil E. Caporaso, 1 Margaret A. Tucker, 6 and Lynn R. Goldin 1 1Genetic Epidemiology Branch, Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD; 2Cancer Genomics Research Laboratory, Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD; 3Ad - vanced Biomedical Computing Center, Leidos Biomedical Research Inc.; Frederick National Laboratory for Cancer Research, Frederick, MD; 4Westat, Inc., Rockville MD; 5Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD; and 6Human Genetics Program, Division of Cancer Epidemiology and Genetics, National Cancer Institute, NIH, Bethesda, MD, USA ©2016 Ferrata Storti Foundation. This is an open-access paper. doi:10.3324/haematol.2015.135475 Received: August 19, 2015. Accepted: January 7, 2016. Pre-published: June 13, 2016. Correspondence: [email protected] Supplemental Author Information: NCI DCEG Cancer Sequencing Working Group: Mark H. Greene, Allan Hildesheim, Nan Hu, Maria Theresa Landi, Jennifer Loud, Phuong Mai, Lisa Mirabello, Lindsay Morton, Dilys Parry, Anand Pathak, Douglas R. Stewart, Philip R. Taylor, Geoffrey S. Tobias, Xiaohong R. Yang, Guoqin Yu NCI DCEG Cancer Genomics Research Laboratory: Salma Chowdhury, Michael Cullen, Casey Dagnall, Herbert Higson, Amy A. -

Regulation of Neuronal Survival and Morphology by the E3 Ubiquitin Ligase RNF157
Cell Death and Differentiation (2015) 22, 626–642 & 2015 Macmillan Publishers Limited All rights reserved 1350-9047/15 www.nature.com/cdd Regulation of neuronal survival and morphology by the E3 ubiquitin ligase RNF157 A Matz1,5, S-J Lee1,5, N Schwedhelm-Domeyer1,5, D Zanini2, A Holubowska1,3, M Kannan1, M Farnworth1, O Jahn3,4, MC Göpfert2 and J Stegmüller*,1,3 Neuronal health is essential for the long-term integrity of the brain. In this study, we characterized the novel E3 ubiquitin ligase ring finger protein 157 (RNF157), which displays a brain-dominant expression in mouse. RNF157 is a homolog of the E3 ligase mahogunin ring finger-1, which has been previously implicated in spongiform neurodegeneration. We identified RNF157 as a regulator of survival in cultured neurons and established that the ligase activity of RNF157 is crucial for this process. We also uncovered that independently of its ligase activity, RNF157 regulates dendrite growth and maintenance. We further identified the adaptor protein APBB1 (amyloid beta precursor protein-binding, family B, member 1 or Fe65) as an interactor and proteolytic substrate of RNF157 in the control of neuronal survival. Here, the nuclear localization of Fe65 together with its interaction partner RNA-binding protein SART3 (squamous cell carcinoma antigen recognized by T cells 3 or Tip110) is crucial to trigger apoptosis. In summary, we described that the E3 ligase RNF157 regulates important aspects of neuronal development. Cell Death and Differentiation (2015) 22, 626–642; doi:10.1038/cdd.2014.163; published online 24 October 2014 Neurodegeneration leads to loss of neurons and thus to In this study, we characterized the novel E3 ubiquitin ligase severe and irreparable damage of the brain. -

Convergence of Genes Implicated in Alzheimer's Disease on the Cerebral
Neurochemistry International 50 (2007) 12–38 www.elsevier.com/locate/neuint Review Convergence of genes implicated in Alzheimer’s disease on the cerebral cholesterol shuttle: APP, cholesterol, lipoproteins, and atherosclerosis C.J. Carter 176 Downs Road, Hastings, East Sussex TN34 2DZ, UK Received 5 April 2006; received in revised form 30 June 2006; accepted 11 July 2006 Available online 12 September 2006 Abstract Polymorphic genes associated with Alzheimer’s disease (see www.polygenicpathways.co.uk) delineate a clearly defined pathway related to cerebral and peripheral cholesterol and lipoprotein homoeostasis. They include all of the key components of a glia/neurone cholesterol shuttle including cholesterol binding lipoproteins APOA1, APOA4, APOC1, APOC2, APOC3, APOD, APOE and LPA, cholesterol transporters ABCA1, ABCA2, lipoprotein receptors LDLR, LRP1, LRP8 and VLDLR, and the cholesterol metabolising enzymes CYP46A1 and CH25H, whose oxysterol products activate the liver X receptor NR1H2 and are metabolised to esters by SOAT1. LIPA metabolises cholesterol esters, which are transported by the cholesteryl ester transport protein CETP. The transcription factor SREBF1 controls the expression of most enzymes of cholesterol synthesis. APP is involved in this shuttle as it metabolises cholesterol to 7-betahydroxycholesterol, a substrate of SOAT1 and HSD11B1, binds to APOE and is tethered to LRP1 via APPB1, APBB2 and APBB3 at the cytoplasmic domain and via LRPAP1 at the extracellular domain. APP cleavage products are also able to prevent cholesterol binding to APOE. BACE cleaves both APP and LRP1. Gamma-secretase (PSEN1, PSEN2, NCSTN) cleaves LRP1 and LRP8 as well as APP and their degradation products control transcription factor TFCP2, which regulates thymidylate synthase (TS) and GSK3B expression. -

Total Body 100-Mgy X-Irradiation Does Not Induce Alzheimer's
Journal of Radiation Research, 2014, 55, 84–96 doi: 10.1093/jrr/rrt096 Advance Access Publication 1 August 2013 Total body 100-mGy X-irradiation does not induce Alzheimer’s disease-like pathogenesis or memory impairment in mice Bing WANG1,*, Kaoru TANAKA1, Bin JI2, Maiko ONO2, Yaqun FANG3, Yasuharu NINOMIYA1, Kouichi MARUYAMA1, Nakako IZUMI-NAKAJIMA3, Nasrin BEGUM4, Makoto HIGUCHI2, Akira FUJIMORI3, Yoshihiko UEHARA5, Tetsuo NAKAJIMA1, Tetsuya SUHARA2, Tetsuya ONO6 and Mitsuru NENOI1 1Research Center for Radiation Protection, National Institute of Radiological Sciences, 4-9-1, Anagawa, Inage-ku, Chiba 263-8555, Japan 2Molecular Imaging Center, National Institute of Radiological Sciences, 4-9-1, Anagawa, Inage-ku, Chiba 263-8555, Japan 3Research Center for Charged Particle Therapy, National Institute of Radiological Sciences, 4-9-1, Anagawa, Inage-ku, Chiba 263-8555, Japan 4Center for Nuclear Medicine and Ultrasound, Rajshahi H-18, Rajshahi Medical College Hospital Campus, Medical College Road, Rajshahi 6000, People’s Republic of Bangladesh 5Graduate School of Medicine, Tohoku University, 2-1, Seiryo-machi, Aoba-ku, Sendai 980-8575, Japan 6Institute for Environmental Sciences, 1-7, Ienomae, Obuchi, Rokkasho-mura, Kamikita-gun, Aomori 039-3212, Japan *Corresponding author. Tel: +81-43-206-3093; Fax: +81-43-251-4582; Email: [email protected] (Received 18 May 2013; revised 1 July 2013; accepted 3 July 2013) The cause and progression of Alzheimer’s disease (AD) are poorly understood. Possible cognitive and behav- ioral consequences induced by low-dose radiation are important because humans are exposed to ionizing radi- ation from various sources. Early transcriptional response in murine brain to low-dose X-rays (100 mGy) has been reported, suggesting alterations of molecular networks and pathways associated with cognitive functions, advanced aging and AD. -

An Analysis of 15 Polymorphisms in Prior Candidate Genes for Sporadic Alzheimer's Disease
European Journal of Human Genetics (2001) 9, 437 ± 444 ã 2001 Nature Publishing Group All rights reserved 1018-4813/01 $15.00 www.nature.com/ejhg ARTICLE Lack of replication of association findings in complex disease: an analysis of 15 polymorphisms in prior candidate genes for sporadic Alzheimer's disease Jonathan A Prince*,1, Lars Feuk1, Sarah L Sawyer1, Johan Gottfries5, Anne Ricksten2, Katarina NaÈgga3, Nenad Bogdanovic4, Kaj Blennow2 and Anthony J Brookes1 1Center for Genomics Research, Karolinska Institute, Stockholm, Sweden; 2Department of Clinical Neuroscience and Transfusion Medicine, University of GoÈteborg, Sahlgren's University Hospital, Sweden; 3Department of Geriatric Medicine, LinkoÈping University Hospital, LinkoÈping, Sweden; 4Department of Clinical Neuroscience and Family Medicine, Section of Geriatric Medicine, Karolinska Institute, Huddinge University Hospital, Stockholm, Sweden; 5Department of Medicinal Chemistry, AstraZeneca, MoÈlndal, Sweden There is considerable enthusiasm for the prospect of using common polymorphisms (primarily single nucleotide polymorphisms; SNPs) in candidate genes to unravel the genetics of complex disease. This approach has generated a number of findings of loci which are significantly associated with sporadic Alzheimer's disease (AD). In the present study, a total of 15 genes of interest were chosen from among the previously published reports of significant association in AD. Genotyping was performed on polymorphisms within those genes (14 SNPs and one deletion) using Dynamic Allele Specific -

A System for Enhancing Genome-Wide Coexpression Dynamics Study
A system for enhancing genome-wide coexpression dynamics study Ker-Chau Li†‡, Ching-Ti Liu, Wei Sun, Shinsheng Yuan†, and Tianwei Yu Department of Statistics, 8125 Mathematical Sciences Building, University of California, Los Angeles, CA 90095-1554 Edited by Michael S. Waterman, University of Southern California, Los Angeles, CA, and approved August 30, 2004 (received for review April 28, 2004) Statistical similarity analysis has been instrumental in elucidation mRNA level. Yet a third possibility can be described in terms of LA. of the voluminous microarray data. Genes with correlated expres- This more advanced concept of statistical association originates sion profiles tend to be functionally associated. However, the from the need to describe a situation as schematized in Fig. 1 Left, majority of functionally associated genes turn out to be uncorre- wherein two opposing trends between X and Y are displayed. The lated. One conceivable reason is that the expression of a gene can positive and negative correlations cancel each other out, rendering be sensitively dependent on the often-varying cellular state. The the overall correlation insignificant. It would be valuable to learn intrinsic state change has to be plastically accommodated by why and how the change of trend occurs. But for real data, such gene-regulatory mechanisms. To capture such dynamic coexpres- hidden trends are not easy to detect directly from the scatterplot of sion between genes, a concept termed ‘‘liquid association’’ (LA) has X and Y. To alleviate the difficulty, we look for additional variables been introduced recently. LA offers a scoring system to guide a that may be associated with the change of the trend. -

Intracellular Lipid Metabolism Impairs Β Cell Compensation During Diet-Induced Obesity
Intracellular lipid metabolism impairs β cell compensation during diet-induced obesity Risheng Ye, … , Joachim Herz, Philipp E. Scherer J Clin Invest. 2018;128(3):1178-1189. https://doi.org/10.1172/JCI97702. Research Article Endocrinology Metabolism The compensatory proliferation of insulin-producing β cells is critical to maintaining glucose homeostasis at the early stage of type 2 diabetes. Failure of β cells to proliferate results in hyperglycemia and insulin dependence in patients. To understand the effect of the interplay between β cell compensation and lipid metabolism upon obesity and peripheral insulin resistance, we eliminated LDL receptor–related protein 1 (LRP1), a pleiotropic mediator of cholesterol, insulin, energy metabolism, and other cellular processes, in β cells. Upon high-fat diet exposure, LRP1 ablation significantly impaired insulin secretion and proliferation of β cells. The diminished insulin signaling was partly contributed to by the hypersensitivity to glucose-induced, Ca2+-dependent activation of Erk and the mTORC1 effector p85 S6K1. Surprisingly, in LRP1-deficient islets, lipotoxic sphingolipids were mitigated by improved lipid metabolism, mediated at least in part by the master transcriptional regulator PPARγ2. Acute overexpression of PPARγ2 in β cells impaired insulin signaling and insulin secretion. Elimination of Apbb2, a functional regulator of LRP1 cytoplasmic domain, also impaired β cell function in a similar fashion. In summary, our results uncover the double-edged effects of intracellular lipid metabolism on β cell function and viability in obesity and type 2 diabetes and highlight LRP1 as an essential regulator of these processes. Find the latest version: https://jci.me/97702/pdf RESEARCH ARTICLE The Journal of Clinical Investigation Intracellular lipid metabolism impairs β cell compensation during diet-induced obesity Risheng Ye,1,2 Ruth Gordillo,1 Mengle Shao,1 Toshiharu Onodera,1 Zhe Chen,1,3 Shiuhwei Chen,1 Xiaoli Lin,1 Jeffrey A. -

Extracting Unrecognized Gene Relationships from the Biomedical Literature Via Matrix Factorizations
Extracting Unrecognized Gene Relationships from the Biomedical Literature via Matrix Factorizations Hyunsoo Kim∗1, Haesun Park∗1 and Barry L. Drake1 1 College of Computing, Georgia Institute of Technology, 266 Ferst Drive, Atlanta, GA 30332, USA. Email: H. Kim∗- [email protected]; H. Park∗- [email protected]; B. L. Drake - [email protected]; ∗Corresponding author Abstract Background: The construction of literature-based networks of gene-gene interactions is one of the most important applications of text mining in bioinformatics. Extracting potential gene relationships from the biomedical literature may be helpful in building biological hypotheses that can be explored further experimentally. Recently, latent semantic indexing based on the singular value decomposition (LSI/SVD) has been applied to gene retrieval. However, the determination of the number of factors k used in the reduced rank matrix is still an open problem. Results: In this paper, we introduce a way to incorporate a priori knowledge of gene relationships into LSI/SVD to determine the number of factors. We also explore the utility of the non-negative matrix factorization (NMF) to extract unrecognized gene relationships from the biomedical literature by taking advantage of known gene relationships. A gene retrieval method based on NMF (GR/NMF) showed comparable performance with LSI/SVD. Conclusions: Using known gene relationships of a given gene, we can determine the number of factors used in the reduced rank matrix and retrieve unrecognized genes related with the given gene by LSI/SVD or GR/NMF. 1 Background Latent semantic indexing based on the singular value decomposition (LSI/SVD) [1, 2] uses the truncated singular value decomposition as a low-rank approximation of a term-by-document matrix. -
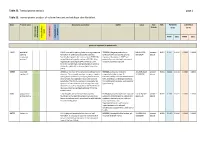
Inline-Supplementary-Material-6.Pdf
Table S3. Transcriptome analysis page 1 Table S3. Transcriptomic analysis of cultured mutant and wildtype skin fibroblast. Gene Protein name GeneCards annotation OMIM Locus Fold FDR PATIENTS CONTROLS - change (n=2) (n=4) ment apoptosis apoptosis Keratinocyte Keratinocyte inflammation differentiation Neurodevelop cell growth and growth cell FPKM [SD] FPKM [SD] genes up-regulated in patient cells ESRP1 epithelial ESRP1 is an mRNA splicing factor that regulates the *612959, the gene product is an 8:95653301 - present - 0.011 0.3547 0.0038 0.0000 0.0000 splicing formation of epithelial cell-specific isoforms. epithelial cell-type-specific splicing 95719694 absent regulatory Specifically regulates the expression of FGFR2-IIIb, regulator. Mutations in ESRP1 are protein 1 an epithelial cell-specific isoform of FGFR2. Also potentially associated with autosomal regulates the splicing of CD44, CTNND1, ENAH, recessive deafness type 109. three transcripts that undergo changes in splicing during the epithelial-to-mesenchymal transition (EMT). CERS3 ceramide CERS3 is a member of the ceramide synthase family #615023, autosomal recessive 15:100913143 - present - 0.011 0.1844 0.0118 0.0000 0.0000 synthase 3 of genes. The ceramide synthase enzymes regulate congenital ichthyosis type 9, 101085200 absent sphingolipid synthesis by catalyzing the formation characterized by collodian membrane at of ceramides from sphingoid base and acyl-CoA birth, acanthosis, orthohyperkeratosis, substrates. This family member is involved in the fine erythrodermic scales, palmoplantar synthesis of ceramides with ultra-long-chain acyl- hyperlinearity. moieties (ULC-Cers), important to the epidermis in its role in creating a protective barrier from the environment. GJB6 gap junction GJB6 encodes one of the connexin proteins. -

Table S1. 103 Ferroptosis-Related Genes Retrieved from the Genecards
Table S1. 103 ferroptosis-related genes retrieved from the GeneCards. Gene Symbol Description Category GPX4 Glutathione Peroxidase 4 Protein Coding AIFM2 Apoptosis Inducing Factor Mitochondria Associated 2 Protein Coding TP53 Tumor Protein P53 Protein Coding ACSL4 Acyl-CoA Synthetase Long Chain Family Member 4 Protein Coding SLC7A11 Solute Carrier Family 7 Member 11 Protein Coding VDAC2 Voltage Dependent Anion Channel 2 Protein Coding VDAC3 Voltage Dependent Anion Channel 3 Protein Coding ATG5 Autophagy Related 5 Protein Coding ATG7 Autophagy Related 7 Protein Coding NCOA4 Nuclear Receptor Coactivator 4 Protein Coding HMOX1 Heme Oxygenase 1 Protein Coding SLC3A2 Solute Carrier Family 3 Member 2 Protein Coding ALOX15 Arachidonate 15-Lipoxygenase Protein Coding BECN1 Beclin 1 Protein Coding PRKAA1 Protein Kinase AMP-Activated Catalytic Subunit Alpha 1 Protein Coding SAT1 Spermidine/Spermine N1-Acetyltransferase 1 Protein Coding NF2 Neurofibromin 2 Protein Coding YAP1 Yes1 Associated Transcriptional Regulator Protein Coding FTH1 Ferritin Heavy Chain 1 Protein Coding TF Transferrin Protein Coding TFRC Transferrin Receptor Protein Coding FTL Ferritin Light Chain Protein Coding CYBB Cytochrome B-245 Beta Chain Protein Coding GSS Glutathione Synthetase Protein Coding CP Ceruloplasmin Protein Coding PRNP Prion Protein Protein Coding SLC11A2 Solute Carrier Family 11 Member 2 Protein Coding SLC40A1 Solute Carrier Family 40 Member 1 Protein Coding STEAP3 STEAP3 Metalloreductase Protein Coding ACSL1 Acyl-CoA Synthetase Long Chain Family Member 1 Protein