Winter 2019 Texas Psychologist
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
TAYLOR Your Community
PRESSTAYLOR your community. your newspaper. General Election | Nov. 6, 2018 FULL-TIME EARLY VOTING LOCATIONS MOBILE-TEMPORARY EARLY VOTING LOCATIONS Monday, Oct. 22 through Friday, Georgetown Randall Monday, Oct. 22 through Friday, Saturday, Oct. 27 Nov. 2 — 7 am to 7 pm 5721 Williams Drive, Georgetown Nov. 2, 10 am to 7 pm Williamson County Annex, 3407 RR Sunday, Oct. 28 — 1 pm to 6 pm Parks & Recreation Admin Bldg Sunday, Oct. 28 1869, Liberty Hill 1101 North College Street, 1 pm to 6 pm Sunday, Oct. 28 Williamson County Inner Loop Georgetown Granger ISD, Annex Hutto City Hall Monday, Oct. 22 300 Colorado Street, Granger 301 SE Inner Loop, Georgetown 401 W Front Street, Hutto Southwestern University – Robert- Monday, Oct. 29 son Center, 930 Southwestern Dr., Anderson Mill Limited District Leander Public Library Spicewood Springs Branch, Austin Georgetown 11500 El Salido Parkway, Austin 1011 South Bagdad Street, Leander Public Library, 8637 Spicewood Tuesday, Oct. 23 Hartfield PAC at McNeil HS BACA Senior Center Springs Rd, Austin Clairmont Retirement Community, 5800 McNeil Drive, Austin 301 West Bagdad St, Building 2, Tuesday, Oct. 30 12463 Los Indios Tr., Austin Cedar Park Public Library Round Rock Bartlett Town Hall, 140 W Clark St., Wednesday, Oct. 24 550 Discovery Boulevard, Cedar Round Rock Randalls Bartlett Florence City Hall, 106 S Patterson Park 2051 Gattis School Road, Wednesday, Oct. 31 Avenue, Florence Cedar Park Randalls Round Rock Schwertner Community Center, Thursday, Oct. 25 1400 Cypress Creek Road, Cedar Brushy Creek Community Cnter 14774 FM 1105, Schwertner Jarrell Memorial Park Community Park 16318 Great Oaks Drive, Thursday, Nov. -

IDEOLOGY and PARTISANSHIP in the 87Th (2021) REGULAR SESSION of the TEXAS LEGISLATURE
IDEOLOGY AND PARTISANSHIP IN THE 87th (2021) REGULAR SESSION OF THE TEXAS LEGISLATURE Mark P. Jones, Ph.D. Fellow in Political Science, Rice University’s Baker Institute for Public Policy July 2021 © 2021 Rice University’s Baker Institute for Public Policy This material may be quoted or reproduced without prior permission, provided appropriate credit is given to the author and the Baker Institute for Public Policy. Wherever feasible, papers are reviewed by outside experts before they are released. However, the research and views expressed in this paper are those of the individual researcher(s) and do not necessarily represent the views of the Baker Institute. Mark P. Jones, Ph.D. “Ideology and Partisanship in the 87th (2021) Regular Session of the Texas Legislature” https://doi.org/10.25613/HP57-BF70 Ideology and Partisanship in the 87th (2021) Regular Session of the Texas Legislature Executive Summary This report utilizes roll call vote data to improve our understanding of the ideological and partisan dynamics of the Texas Legislature’s 87th regular session. The first section examines the location of the members of the Texas Senate and of the Texas House on the liberal-conservative dimension along which legislative politics takes place in Austin. In both chambers, every Republican is more conservative than every Democrat and every Democrat is more liberal than every Republican. There does, however, exist substantial ideological diversity within the respective Democratic and Republican delegations in each chamber. The second section explores the extent to which each senator and each representative was on the winning side of the non-lopsided final passage votes (FPVs) on which they voted. -
2018 BMS PAC Contributions
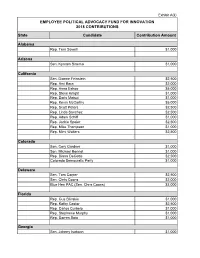
Exhibit A(ii) EMPLOYEE POLITICAL ADVOCACY FUND FOR INNOVATION 2018 CONTRIBUTIONS State Candidate Contribution Amount Alabama Rep. Terri Sewell $1,000 Arizona Sen. Kyrsten Sinema $1,000 California Sen. Dianne Feinstein $2,500 Rep. Ami Bera $2,000 Rep. Anna Eshoo $5,000 Rep. Steve Knight $1,000 Rep. Doris Matsui $1,000 Rep. Kevin McCarthy $5,000 Rep. Scott Peters $2,500 Rep. Linda Sanchez $2,500 Rep. Adam Schiff $1,000 Rep. Jackie Speier $2,500 Rep. Mike Thompson $1,000 Rep. Mimi Walters $2,500 Colorado Sen. Cory Gardner $1,000 Sen. Michael Bennet $1,000 Rep. Diana DeGette $2,500 Colorado Democratic Party $1,000 Delaware Sen. Tom Carper $2,500 Sen. Chris Coons $2,000 Blue Hen PAC (Sen. Chris Coons) $3,000 Florida Rep. Gus Bilirakis $1,000 Rep. Kathy Castor $2,500 Rep. Carlos Curbelo $1,000 Rep. Stephanie Murphy $1,000 Rep. Darren Soto $1,000 Georgia Sen. Johnny Isakson $1,000 Sen. David Perdue $2,000 Rep. Buddy Carter $2,500 Iowa Gov. Kim Reynolds $2,000 Sen. Chuck Grassley $2,500 State Sen. Charles Schneider $2,000 State Sen. Tom Shipley $500 Idaho Sen. Mike Crapo $5,000 Illinois Rep. Cheri Bustos $1,000 Rep. Bill Foster $1,000 Rep. Robin Kelly $1,000 Rep. Darin LaHood $1,000 Rep. Pete Roskam $1,000 Rep. Brad Schneider $1,000 Rep. John Shimkus $2,500 Indiana Sen. Mike Braun $1,000 Sen. Joe Donnelly $2,500 Rep. Larry Bucshon $2,500 Rep. Susan Brooks $2,000 Rep. Andre Carson $1,000 Rep. -

Legislative Update
January 29, 2021| Regular Session, Issue 3 | 87th Regular Session Every Friday, this newsletter will keep you up to speed on some of the legislation important to Texas Farm Bureau members that Austin staff are following. Please do not hesitate to contact the appropriate staff with any questions. Legislative Update Water SB 152 and companion HB 668: Relating to the regulation of groundwater conservation districts. Perry, Charles (R) and Harris, Cody (R) Summary: SB 152 and HB 668 empower landowners to protect their constitutional rights from illegal groundwater regulations. Current law does not require enough transparency or provide landowners with reasonable options to change or challenge bad regulations. If property owners are faced with an illegal regulation, they only have one option— to challenge the district’s action in court and take on the risk having to pay the district’s attorney fees. The language in SB 152 and HB 668 is currently being negotiated. The following description of the bills is based upon the current state of negotiations: 1. Requiring notice of a permit or permit amendment that will prevent a neighboring landowner from being able to drill a well on their property or drill at a particular location on their property. The local district will determine how that notice will be provided. This notice will give landowners who will be DIRECTLY affected by the district’s actions an opportunity to decide if they should participate in the permitting process to protect their right to drill a well. In some districts, spacing rules allow a neighbor to drill a well 50 feet from a property line. -
2021 Nurse Day Program
Welcome to TNA’s Nurse Day at the Capitol! Today is an exciting day — you join nurse colleagues from across the state to learn about nursing’s legislative agenda for the 87th session. Thank you for joining hundreds of nurses from across the state to advocate for our policy agenda with one strong voice. Though not gathered under the Capitol dome this year, our message is no less united and powerful as we connect virtually with policy makers to advance legislative interests to benefit nurses and the Texans we serve. Your presence with us today makes a difference! We hope you gain perspective of opportunities you have to engage with TNA, leverage your influence and advance the health of Texans. Previous participants have said that attending this event has been pivotal in their professional career — providing them a window into a whole new avenue of nursing influence and advocacy to improve patient care. We hope you share this experience and continue your involvement in TNA long after today. Thank you for participating in TNA’s Nurse Day at the Capitol! Sincerely, Tammy Eades, DNP, MSN, Cindy Zolnierek, PhD, RN, RN CAE President Chief Executive Officer Agenda February 8, 2021 1 – 1:15 p.m. Welcome Tammy Eades, DNP, MSN, RN President, Texas Nurses Association 1:15 – 1:50 p.m. Keynote: Texas’ Public Health Landscape John Hellerstedt, MD Commissioner Stay Informed! Texas Department of State Health Services Follow @TXNursesLege. 1:50 – 2 p.m. Break Use #TXNurseDay. 2 – 2:45 p.m. Nursing’s Role in Health Policy Serena Bumpus, DNP, MSN, RN Director of Practice, Texas Nurses Association 2:45 – 3:30 p.m. -

MCF CONTRIBUTIONS JULY 1 - DECEMBER 31, 2016 Name State Candidate Amount U.S
MCF CONTRIBUTIONS JULY 1 - DECEMBER 31, 2016 Name State Candidate Amount U.S. House Robert Aderholt for Congress AL Rep. Robert Aderholt $2,000 ALABAMA TOTAL U.S. House Crawford for Congress AR Rep. Rick Crawford $1,500 Womack for Cogress Committee AR Rep. Stephen Womack $500 ARKANSAS TOTAL U.S. House Kyrsten Sinema for Congress AZ Rep. Kyrtsen Sinema $500 ARIZONA TOTAL U.S. House Denham for Congress CA Rep. Jeff Denham $1,500 Garamendi for Congress CA Rep. John Garamendi $500 Kevin McCarthy for Congress CA Rep. Kevin McCarthy $1,000 Valadao for Congress CA Rep. David Valadao $1,500 U.S. House Leadership Majority Committee PAC--Mc PAC CA Rep. Kevin McCarthy $5,000 State Assembly Adam Gray for Assembly 2016 CA Assm. Adam Gray $1,500 Catharine Baker for Assembly 2016 CA Assm. Catharine Baker $2,500 Cecilia Aguiar-Curry for Assembly 2016 CA Assm. Cecilia Aguiar-Curry $2,000 Chad Mayes for Assembly 2016 CA Assm. Chad Mayes $2,000 James Gallagher for Assembly 2016 CA Assm. James Gallagher $1,500 Patterson for Assembly 2016 CA Assm. James Patterson $2,000 Jay Obernolte for Assembly 2016 CA Assm. Jay Obernolte $1,500 Jim Cooper for Assembly 2016 CA Assm. Jim Cooper $1,500 Jimmy Gomez for Assembly 2016 CA Assm. Jimmy Gomez $1,500 Dr. Joaquin Arambola for Assembly 2016 CA Assm. Joaquin Arambula $1,500 Ken Cooley for Assembly 2016 CA Assm. Ken Cooley $1,500 Miguel Santiago for Assembly 2016 CA Assm. Miguel Santiago $1,500 Rudy Salas for Assembly 2016 CA Assm. -
Charles Schwertner, M.D. T E X a S S E N a T O R
AN OFFICIAL PUBLICATION OF THE TEXAS SENATE FALL 2018 CHARLES SCHWERTNER, M.D. T E X A S S E N A T O R Dear Friends, I’d like to begin by thanking you for the great privilege of representing you and your family in the Texas State Senate. As your voice in Austin, I’m working each and every day to make sure that we’re building a Texas government that’s both responsive to your needs and responsible with your tax dollars. Like all legislative sessions, the meeting of the 85th Texas Legislature in 2017 presented its fair share of challenges. With you, the hard-working taxpayer in mind, we started by passing a balanced and appropriate state budget that doesn’t raise taxes on citizens or businesses. We cracked down on sanctuary cities that allow dangerous illegal immigrants to commit crimes in our country and roam our streets with impunity. We worked to protect vulnerable foster children by making sweeping changes to our state’s foster system and office of Child Protective Services (CPS). We got tough on bad nursing homes that put our parents and grandparents at risk for abuse or neglect. Perhaps most importantly of all, we defended the God-given constitutional rights of our citizens. As the 10th largest economy in the world, Texas continues to attract new investment and new opportunities from all across the globe. This past year, Texas added a staggering 230,300 new private-sector jobs and saw our state’s unemployment rate drop to its lowest point in over 40 years (4%). -

Oil & Gas Companies, AT&T Affiliated Pacs, USAA, and San Antonio
Oil & Gas Companies, AT&T Affiliated PACs, USAA, And San Antonio Spurs Leadership Are Among The Top Corporate Donors To The 15 Conservative Texas Lawmakers That Advanced Voting Restrictions Over The Weekend Of July 10th Top Corporate Donors Of The Six Conservative Members Of The Texas Senate State Affairs Committee—The Senate Committee Which Already Advanced Voting Restriction Bill SB1 During Texas’ Special Session— Include Texas Oil Moguls, AT&T Affiliated PACs, San Antonio Spurs Leadership, And Other Corporate Entities In 2021, The Texas Senate State Affairs Committee Advanced Senate Bill 7 (SB 7), A Voting Restrictions Bill That Legislators Later Killed By Walking Out Of The Regular Legislative Session—Now, Legislators Are Considering Similar Legislation During A July 2021 Special Session In 2021, The Texas Senate State Affairs Committee Advanced Texas’ Senate Bill 7 (SB 7), A Bill That Would Curb Early Voting Hours, Give “Alarming” Power To Poll Watchers, And Limit Voting Options That Were “Especially Effective Last Year In Reaching Voters Of Color” The Senate State Affairs Committee Advanced Texas’ Senate Bill 7 (SB 7) In 2021. [Texas Legislature, accessed 07/08/21] SB 7 Was “Best Known For Curbing Early Voting Hours And Banning 24-Hour Voting And Drive Through Voting.” “Amid the heated presidential race last fall, Texas polling places experienced ‘a surge in voter intimidation,’ according to the Texas Civil Rights Project. The group received 267 complaints from around the state. Many involved demonstrators shouting at voters outside of polling places, an escalation of harassment that local election officials in 2018 described as the worst they had seen in decades. -

Running on Hydrocarbons: Oil and Gas Funding to Every Texas Lawmaker
Running on Hydrocarbons: Oil and Gas Funding to Every Texas Lawmaker Texans for Public Justice Public Citizen’s Texas Office Sierra Club May 2017 Running on Hydrocarbons: Oil and Gas Funding to Every Texas Lawmaker (2013-2016) he Texas Sunset Advisory Commission typically reviews state agencies every 12 years to determine if the agencies are efficient, need reform, or should be abolished. The Texas Railroad Commission T just underwent its third Sunset review since 2010. A hard-hitting 2013 Sunset staff report recommended the agency’s three elected commissioners should only be allowed to raise money during an 18-month period surrounding an election (instead of throughout most of their six-year terms). It also recommended that the agency develop rules to prevent informal, ex parte discussions of contested cases, and to ban commissioners from taking money from parties to contested cases. Our recent Conflicted report found that commissioners continue to take contributions from parties with pending contested cases, despite their claims that they “self-police” such conflicts. The 2016 Sunset staff report slammed the agency’s deceptive name, calling for its rechristening as the “Texas Energy Resources Commission.” It suggested that the agency’s case hearings and gas-utility rate cases could be done more professionally and transparently by the State Office of Administrative Hearings and the Public Utility Commission, respectively. In their report, Sunset staff argued that major agency changes are needed to improve pipeline safety, increase bonding requirements for new oil and gas drilling and to intensify inspection and enforcement efforts. Yet the latest report did not address commissioner fundraising conflicts. -

April 13-23, 2021
the sentinel TEXAS ETHICS & RELIGIOUS LIBERTY COMMITTEE Texas Legislative Update April 13-23, 2021 Voting: Local Elections in Texas for City Council and School Board races are upon us and are very important! Early voting for the May 1st election is April 19-April 27. Please see here for info regarding candidates ivoterguide.com Click here to find your polling location and where to vote: teamrv-mvp.sos.texas.gov Your Christian guide to voting in city elections: christiansengaged.org 87th Texas Legislative Session: Please continue to pray and stay engaged in the session which ends May 31st. There is still much work to be done! A quick email or phone call can make all the difference. Bills left in committee after the end of April/beginning of May will have little chance of being passed. Update On Gender Modification Bills 1. Senator Bob Hall’s SB 1311 would protect children from receiving puberty-suppression drugs, cross-sex hormones, medical procedures or surgeries for the purpose of gender reassignment- this bill received a hearing and has passed out of the Senate State Affairs Committee, but now needs to be voted on the Senate floor. Senator Hall says, “ Every single child is created in the image of God. Altering a healthy, completely natural part of His creation in such a way is not only morally wrong, but also carries dire consequences. There are countless testimonies of adults who underwent transition procedures as children, but regret it now. Ranging from bone density problems to fertility issues, these are more than just side effects of a drug or procedure. -

Session 3 NP Leadership Presentation
11/6/17 Nurse Practitioners as Leaders: A Discussion with Nurse Executives, Legislators, and Grassroots Activists Texas Health Care Policy & Leadership Conference November 10th, 2017 Dr. Danielle Howa Pendergrass DNP, APRN, WHNP-BC EasternUtahWomensHealth @easternUTwomen Key Messages: #1 Nurses should practice to the full extent of their education and training (p.4) #3 Nurses Should Be Full Partners, with Physicians and Other Health Professionals, in Redesigning Health Care in the United States (p.7) 2 Recommendations: #1 Remove Scope of Practice Barriers (p.9) #7 Prepare and Enable Nurses to Lead Change to Advance Health (p.14) 3 1 11/6/17 We are here for YOU! #1 Priority 4 Representation in Texas Legislature Nurses Physicians 1. Rep. Howard, Donna, District 1. Rep. Bonnen, Greg District 24 48 2. Rep. Oliverson, Tom District 130 2. Rep. Klick, Stephanie, District 3. Rep. Sheffield, J. D. District 91 59 4. Rep. Zerwas, John District 28 5. Senator Donna Campbell, District 25 6. Senator Dawn Buckingham, District 24 7. Senator Charles Schwertner, District 5 8. * Rep. Anderson, Charles "Doc” District 56 9. * Rep. Stucky, Lynn District 64 5 Serving in Congress Nurses Physicians 1. Congresswoman Karen Bass (D-CA- 1. Rep. Ralph Abraham, MD, R-La. 33) 2. Sen. John Barrasso, MD, R-Wyo. 2. Congresswoman Diane Black (R-TN- 3. Rep. Ami Bera, MD, D-Calif. 06) 4. Rep. Larry Bucshon, MD, R-Ind. 3. Congresswoman Eddie Bernice 5. Rep. Michael C. Burgess, MD, R- Johnson (D-TX-30) Texas. 6. Sen. Bill Cassidy, MD, R-La. 7. Rep. Scott DesJarlais, MD, R-Tenn. -

Schwertner Tapped to Lead Senate Workgroup on Child Protection
SENATOR CHARLES SCHWERTNER, MD SENATE DISTRICT 5 FOR IMMEDIATE RELEASE October 27, 2016 Contact: Tom Holloway (512) 923-5944 Schwertner Tapped to Lead Senate Workgroup on Child Protection With the state facing substantial challenges in both CPS investigations and foster care capacity, Senator Schwertner takes the lead in getting child protection back on track AUSTIN, TX -- At the conclusion of last night's Senate Finance Committee hearing, Senator Charles Schwertner (R-Georgetown) was tasked with leading the new Senate Workgroup on Child Protection, a subset of the Senate Finance Committee that will evaluate the recent critical needs funding request submitted by the Department of Family and Protective Services (DFPS). "As a father of three, I believe that ensuring the safety and protection of our state's children is one of the legislature's most important responsibilities," said Schwertner. "As Chairman of the Senate Workgroup on Child Protection, I think I speak for everyone when I say we're committed to doing whatever is necessary to fix the disturbing gaps in our CPS and foster care system. We owe it to the children of Texas to get this right." The workgroup plans to solicit input from DFPS concerning its plans to address troubling deficiencies in conducting timely CPS investigations and ensuring sufficient foster care capacity before making its recommendations to the full Senate Finance Committee regarding the need for additional state resources. In addition to Senator Schwertner, Senators Brian Birdwell (R- Granbury), Lois Kolkhorst (R-Brenham), Kirk Watson (D-Austin), and John Whitmire (D-Houston) were also named to the Senate Workgroup on Child Protection.