Leopard Gecko Diseases and Care Thomas H. Boyer, DVM, DABVP (Reptile & Amphibian Practice); Michael M
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Lentiviral Transgenesis of the Leopard Gecko, Eublepharis Macularius
Vol. 8(10), pp. 1070-1079, 5 March, 2014 DOI: 10.5897/AJMR2013.6532 ISSN 1996-0808 ©2014 Academic Journals African Journal of Microbiology Research http://www.academicjournals.org/AJMR Full Length Research Paper Lentiviral transgenesis of the leopard gecko, Eublepharis macularius Kaitlyn Hull1, Dee Hodgson1, Bob Clark2, Timothy W. Hickok2, James N. Petitte1 and Paul E. Mozdziak1,3 1Department of Poultry Science, North Carolina State University, Raleigh NC, 27695, United States. 2Nucleic Sciences LLC. 6701 W. 121st Suite 200, Overland Park KS 66209, United States. Accepted 13 January, 2014 Lentiviral vectors are an effective method of introducing transgenes into the genome of early stage embryos because they transduce both dividing and non-dividing cells. Lentiviral pseudoparticles containing the coding sequence for the fluorescent protein DsRed were injected into freshly laid leopard gecko eggs. Tissue samples were collected from hatchlings, and the samples were tested for the presence of the transgene. Of the injected gecko population, greater than 89% of efficiency of transgenesis was confirmed using polymerase chain reaction (PCR). Histological evaluations revealed the presence of DsRed 2 in injected gecko organs; with protein production concentrated in the muscle, kidney, and heart. Therefore, lentiviral vectors appear to be viable technology to create transgenic geckos. Key words: DsRed, Eublepharis macularius, Feline Immunodeficienty Virus (FIV), lentiviral transgenesis, reptiles. INTRODUCTION Lentiviruses are used in biotechnology to integrate and pancreas (Wang et al., 1999; Loewen et al., 2001; foreign DNA into a host genome, facilitating foreign gene Curran and Nolan, 2002; Curran et al., 2002; Derksen et expression (Pfeifer, 2004). Lentiviruses belong to the al., 2002; Price et al., 2002; Stein and Davidson 2002). -

Leopard Geckos & African Fat-Tails Geckos
A Compassionate Commitment to Quality Pet Care! LEOPARD GECKOS & AFRICAN FAT-TAILS GECKOS SPECIES NAMES Leopard geckos (Eublepharis maclarius), African fat-tailed geckos (Hemitheconyx caudicinctus). Both are members of the Eublepharidae family, which includes all species of geckos with moveable eyelids. CAGING/HOUSING For a single gecko, a 10-gallon glass aquarium with a securely fastened wire mesh top is appropriate. For two or more geckos a 20- gallon or larger aquarium is necessary. For substrate use paper towels, newspaper, or artificial turf, washed orchard bark, or aquarium gravel. The use of sand or calcium-fortified sand (such as ReptiSand™ or Calci-Sand™) is not recommended for geckos less than 6 inches in length, due to the risk of ingestion and subsequent impaction in the gastrointestinal tract. A hide-box, or shelter, should be provided to allow the gecko a quiet retreat. LIGHTING/HEATING In order to properly thermo-regulate, leopard geckos need a temperature gradient that allows them to move from a cooler end of the tank to a warmer end. This temperature gradient should range between 70°F at the cool end at 85°F at the high end. African fat-tailed geckos require slightly higher temperatures ranging from between 80°F and 92°F. Since these geckos are nocturnal, UV lighting is not necessary. HUMIDITY A moderate level of humidity is required for these geckos, which can be provided by misting and providing a large water bowl for the animal to soak in. Low humidity levels can lead to problems with shedding. FEEDING Food items, as a general rule, should be no longer than the length, and less than half the width of the geckos head. -

Body-Size Effect on Egg Size in Eublepharid Geckos (Squamata
Blackwell Publishing LtdOxford, UKBIJBiological Journal of the Linnean Society0024-4066The Linnean Society of London, 20062006 884 527532 Original Article EGG-SIZE ALLOMETRY IN EUBLEPHARID GECKOS L. KRATOCHVÍL and D. FRYNTA Biological Journal of the Linnean Society, 2006, 88, 527–532. With 2 figures Body-size effect on egg size in eublepharid geckos (Squamata: Eublepharidae), lizards with invariant clutch size: negative allometry for egg size in ectotherms is not universal LUKÁT KRATOCHVÍL1* and DANIEL FRYNTA2 1Department of Ecology, Charles University, Vinidná 7, CZ-128 44 Praha 2, the Czech Republic 2Department of Zoology, Charles University, Vinidná 7, CZ-128 44 Praha 2, the Czech Republic Received 1 February 2005; accepted for publication 5 December 2005 Within a single clutch, smaller species of ectotherms generally lay a smaller number of relatively larger eggs than do larger species. Many hypotheses explaining both the interspecific negative allometry in egg size and egg size– number trade-off postulate the existence of an upper limit to the egg size of larger species. Specifically, in lizards, large eggs of large species could have too long a duration of incubation, or they could be too large to pass through the pelvic opening, which is presumably constrained mechanically in larger species. Alternatively, negative allometry could be a result of limits affecting eggs of smaller species. Under the latter concept, hatchling size in smaller species may be close to the lower limit imposed by ecological interactions or physiological processes, and therefore smaller species have to invest in relatively larger offspring. Contrary to these lower limit hypotheses, explanations based on the existence of an upper limit always predict negative egg-size allometry even in animals with invariant clutch size, in which naturally there is no egg size–number trade-off. -

Identifikasi Parasit Saluran Pencernaan Leopard Gecko
IR – PERPUSTAKAAN UNIVERSITAS AIRLANGGA DAFTAR PUSTAKA Arabkhazaeli, F., A. Rostami, A. Gilvari, S. Nabian and S.A. Madani. 2018. Frequently Observed Parasites in Pet Reptiles’ Feces in Tehran. Iran. J. Vet. Med. 12:23. Boyer, T.H., M.M. Garner, D.R. Reavill and Z.J. Steffes. 2013. Common Problems of Leopard Geckos (Eublepharis macularius). Proceedings Association of Reptilian and Amphibian Veterinarians. 120-121. Brooks, R. 2015. Leopard Gecko Characteristics. CareSheet.com. http://www.caresheets.com/leopard-gecko-care/leopardgeckocharacteristics/ [9 April 2019]. Caccio, S.M. and G. Widmer. 2014. Cryptosporidium: Parasite and Disease. Springer- Verlag Wien. New York. 3. Dellarupe, A., J.M. Unzaga, G. More, M. Kienast, A. Larsen, C. Stiebel, M. Rambeaud and M.C. Venturini. 2016. Cryptosporidium varanii infection in leopard geckos (Eublepharis macularius) in Argentina. Open Vet. Journal. 6(2): 98. De La Navarre, B. 2011. Common Parasitic Disease of Reptiles & Amphibian. Fetch dvm360 Conference. // https://www.fetchdvm360.com/ [26 Juni 2019]. Denver, M.C. 2016. Reptile Protozoa. Veterinarian Key. https://veteriankey.com/reptile-protozoa/ [4 Juli 2019]. De Vosjoli, P., R. Klingenberg, R. Tremper, and B. Viets. 2011. The Leopard gecko Manual: Includes African Fat-Tailed Geckos. i5 Publishing. De Vosjoli, P., T. Mazorlig, R. Klingenberg, R. Tremper, and B. Viets. 2017. The Leopard Gecko Manual: Expert Advice for Keeping and Caring for a Healthy Leopard Gecko. 2nd Edition. Fox Chapel Publishers International. United Kingdom. Donoghue, S. 2016. Basic Information Sheet: Leopard Gecko. LaveberVet. Laveber Company. USA. Eyspana, B.D. 2014. Prevalence of Intestinal Pathogen Protozoa on Dairy Calves in Setia Kawan Dairy Cooperates Nongkojajar Pasuruan. -

GECKO EUBLEPHARIS Scale
SHORT NOTES HERPETOLOGlCAL JOURNAL, Vol. 12, pp. 79-80 (2002) partly regenerated tail. Snout-vent length (SVL) 148 mm, partly regenerated tail length 66 mm, supranasal FIRST RECORD OF THE LEOPARD scales separated by a single, almost hexagonal internasal GECKO EUBLEPHARIS scale. The width of the internasal scale is more than its length, six small additional nasal scales surround the ANGRAMAINYU (REPTILIA: SAURIA: nostril; 11 supra- and 11 infralabial scales; the ear is EUBLEPHARIDAE) FROM ANATOLIA large, with its length (5 mm) 2.5 times its width (2 mm); pentagonal mental is shorter than wide and fo llowed by BAYRAM Gb<;:MEN,M URAT TOSUNOGLU AND fourrows of enlarged scales (postmentalia); chin shields DiN<;:ERA YAZ (the first row of postmentalia) in contact with first Department of Biology, Faculty of Science, Ege infralabials; dorsal tubercles on the flanks almost touch University, 35100 Bornova, lzmir, Turkey ing each other; ventral scales hexagonal and non-imbricate, with 26 hexagonal ventral scales across Key words: gecko, geographical distribution, new record midbody; 13 feebly marked (preanal) pores arranged between the anal cleft and the ventral scales in the form The leopard gecko Eublepharis angramainyu of an inverted "V"; 24 smooth subdigital lamellae on Anderson & Leviton, 1966 occurs in the western foot both hind feet; three transverse rows of ventral scales in hills of the Zagros Mountains and the Mesopotamian each caudal whorl. The background colour of the body plain in Iran, Iraq and north-eastern Syria, with a verti is ochreous with lilac-brown spots; on the head these cal distribution of 300-1 000 m (Anderson & Leviton spots are roughly arranged in longitudinal rows with 1966; Nader & Jawdat, 1976; Leviton et al., 1992; Mar� wider interspaces, bordering the pale continuous stripe tens & Kock, 1991; Anderson, 1999). -

The New Mode of Thought of Vertebrates' Evolution
etics & E en vo g lu t lo i y o h n a P r f y Journal of Phylogenetics & Kupriyanova and Ryskov, J Phylogen Evolution Biol 2014, 2:2 o B l i a o n l r o DOI: 10.4172/2329-9002.1000129 u g o y J Evolutionary Biology ISSN: 2329-9002 Short Communication Open Access The New Mode of Thought of Vertebrates’ Evolution Kupriyanova NS* and Ryskov AP The Institute of Gene Biology RAS, 34/5, Vavilov Str. Moscow, Russia Abstract Molecular phylogeny of the reptiles does not accept the basal split of squamates into Iguania and Scleroglossa that is in conflict with morphological evidence. The classical phylogeny of living reptiles places turtles at the base of the tree. Analyses of mitochondrial DNA and nuclear genes join crocodilians with turtles and places squamates at the base of the tree. Alignment of the reptiles’ ITS2s with the ITS2 of chordates has shown a high extent of their similarity in ancient conservative regions with Cephalochordate Branchiostoma floridae, and a less extent of similarity with two Tunicata, Saussurea tunicate, and Rinodina tunicate. We have performed also an alignment of ITS2 segments between the two break points coming into play in 5.8S rRNA maturation of Branchiostoma floridaein pairs with orthologs from different vertebrates where it was possible. A similarity for most taxons fluctuates between about 50 and 70%. This molecular analysis coupled with analysis of phylogenetic trees constructed on a basis of manual alignment, allows us to hypothesize that primitive chordates being the nearest relatives of simplest vertebrates represent the real base of the vertebrate phylogenetic tree. -
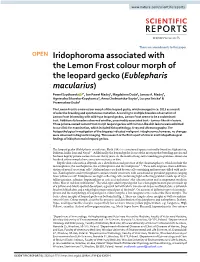
Iridophoroma Associated with the Lemon Frost Colour Morph of The
www.nature.com/scientificreports There are amendments to this paper OPEN Iridophoroma associated with the Lemon Frost colour morph of the leopard gecko (Eublepharis macularius) Paweł Szydłowski 1*, Jan Paweł Madej2, Magdalena Duda3, Janusz A. Madej4, Agnieszka Sikorska-Kopyłowicz3, Anna Chełmońska-Soyta1, Lucyna Ilnicka5 & Przemysław Duda6 The Lemon Frost is a new colour morph of the leopard gecko, which emerged in ca. 2015 as a result of selective breeding and spontaneous mutation. According to multiple breeders observation of Lemon Frost inbreeding with wild-type leopard geckos, Lemon Frost seems to be a codominant trait. Additionally breeders observed another, presumably associated trait - tumour-like skin lesions. Three private-owned Lemon Frost morph leopard geckos with tumour-like skin lesions were admitted to our clinic for examination, which included histopathology, X-ray and ultrasonography. The histopathological investigation of the biopsies indicated malignant iridophoroma; however, no changes were observed in diagnostic imaging. This research is the first report of clinical and histopathological findings of iridophoroma in leopard geckos. The leopard gecko (Eublepharis macularius, Blyth 1845) is a nocturnal species naturally found in Afghanistan, Pakistan, India, Iran and Nepal1,2. Additionally, the leopard gecko is one of the most popular breeding species and has been kept by private owners for over thirty years. As the result of long-term breeding programmes, about one hundred colour morphs have come into existence to date. Reptile skin colouration depends on a distribution and presence of the chromatophores, which include the melanophores, the xanthophores, the erythrophores and the iridophores3–5. These cells originate from a differen- tiation of neural crest stem cells5. -

Independent Evolution of Sex Chromosomes in Eublepharid Geckos, a Lineage with Environmental and Genotypic Sex Determination
life Article Independent Evolution of Sex Chromosomes in Eublepharid Geckos, A Lineage with Environmental and Genotypic Sex Determination Eleonora Pensabene , Lukáš Kratochvíl and Michail Rovatsos * Department of Ecology, Faculty of Science, Charles University, 12844 Prague, Czech Republic; [email protected] (E.P.); [email protected] (L.K.) * Correspondence: [email protected] or [email protected] Received: 19 November 2020; Accepted: 7 December 2020; Published: 10 December 2020 Abstract: Geckos demonstrate a remarkable variability in sex determination systems, but our limited knowledge prohibits accurate conclusions on the evolution of sex determination in this group. Eyelid geckos (Eublepharidae) are of particular interest, as they encompass species with both environmental and genotypic sex determination. We identified for the first time the X-specific gene content in the Yucatán banded gecko, Coleonyx elegans, possessing X1X1X2X2/X1X2Y multiple sex chromosomes by comparative genome coverage analysis between sexes. The X-specific gene content of Coleonyx elegans was revealed to be partially homologous to genomic regions linked to the chicken autosomes 1, 6 and 11. A qPCR-based test was applied to validate a subset of X-specific genes by comparing the difference in gene copy numbers between sexes, and to explore the homology of sex chromosomes across eleven eublepharid, two phyllodactylid and one sphaerodactylid species. Homologous sex chromosomes are shared between Coleonyx elegans and Coleonyx mitratus, two species diverged approximately 34 million years ago, but not with other tested species. As far as we know, the X-specific gene content of Coleonyx elegans / Coleonyx mitratus was never involved in the sex chromosomes of other gecko lineages, indicating that the sex chromosomes in this clade of eublepharid geckos evolved independently. -

Cfreptiles & Amphibians
WWW.IRCF.ORG/REPTILESANDAMPHIBIANSJOURNALTABLE OF CONTENTS IRCF REPTILES & AMPHIBIANSIRCF REPTILES • VOL15, &NO AMPHIBIANS 4 • DEC 2008 189 • 26(1):58–61 • APR 2019 IRCF REPTILES & AMPHIBIANS CONSERVATION AND NATURAL HISTORY TABLE OF CONTENTS FEATURE ARTICLES First. Chasing BullsnakesRecords (Pituophis catenifer sayi) inof Wisconsin: the Common Leopard On the Road to Understanding the Ecology and Conservation of the Midwest’s Giant Serpent ...................... Joshua M. Kapfer 190 Gecko,. The Shared Eublepharis History of Treeboas (Corallus grenadensis) and Humansmacularius on Grenada: (Blyth 1854) A Hypothetical Excursion ............................................................................................................................Robert W. Henderson 198 RESEARCH ARTICLES(Eublepharidae), in Nepal . The Texas Horned Lizard in Central and Western Texas ....................... Emily Henry, Jason Brewer, Krista Mougey, and Gad Perry 204 .YamThe Knight Bahadur Anole ( AnolisRawat equestris1, Kul) in Florida Bahadur Thapa2, Santosh Bhattarai3, and Karan Bahadur Shah2 .............................................Brian J. Camposano, Kenneth L. Krysko, Kevin M. Enge, Ellen M. Donlan, and Michael Granatosky 212 1Department of National Parks and Wildlife Conservation, Shuklaphanta National Park, Kanchanpur, Nepal CONSERVATION ALERT2Himalayan Nature, POB- 10918, Lazimpat, Kathmandu, Nepal 3National Trust for. World’s Nature Mammals Conservation-Biodiversity in Crisis .............................................................................................................................. -

Care of Leopard and Fat-Tailed Geckos
Care of Leopard and Fat-Tailed Geckos Leopard geckos (Eublepharis macularius) and Fat-Tailed geckos (Hemitheconyx caudicinctus) belong to the family of Eubleparidae, which includes all geckos with moveable eyelids. This family also lacks toe pads, thus are unable to climb vertical surfaces. The leopard gecko is found in Afghanistan, India, and Pakistan. As far as reptiles go, the Leopard gecko makes one of the finest pets. They are one of the hardiest lizard species, reach a maximum length of 8 inches, are relatively docile, easy to keep, easy to breed, are potentially long-lived and are undeniably beautiful. Females have been known to live 20 years, and males seem to live longer, the eldest male reported nearly reached 30 years old. There are at least 10 different color and pattern varieties (morphs) of Leopard geckos available in the pet trade. Fat-Tailed geckos are from West Africa and can be as hardy and docile as Leopard geckos. Male Fat-Tailed geckos grow to ten inches while females are less than 8 inches long. Sexing There are slight differences between males and females. Males have a V-shaped row of enlarged pre-anal pores in front of the vent, are more heavy-bodied and have a broader head and thicker necks than females. Males also have paired hemipenal swellings at the tail base. Enclosure and Substrate Leopard and Fat-Tailed geckos do not require the company of other geckos and seem to thrive by themselves. Males will fight and should never be kept together. If you wish to keep two geckos, two females of the same species would be best. -

Clues to the Past and Inspiration for the Future by Gregory D
MODEL OF THE MONTH Clues to the past and inspiration for the future by Gregory D. Larsen vision3. These traits are common and specialized among different Scientific name gecko species, though rare among other lizards, and their various Gekko gecko forms might hold clues as to how these complex senses evolved in TaxOnOmy other lineages of terrestrial vertebrates. PHYLUM: Chordata Like many reptiles and amphibians, geckos can sever their own ClASS: Reptilia tails and grow a similar replacement. Although the new tail is not a complete replica, it reflects regenerative capabilities far superior OrDEr: Squamata to those of most non-reptilian amniotes1. Many researchers have FAmIly: Gekkonidae therefore investigated the mechanisms of the underlying process, hoping that they might advance regenerative medicine in humans. Geckos are perhaps best known for their ability to scale and grip Physical description nearly any surface, which has inspired many studies and The Tokay gecko (Gekko gecko) is a inventions in recent years. Many gecko species nocturnal arboreal lizard whose possess adhesive pads on their toes, which native range spans the rainforests are covered in keratinous setae made of south and s outheast Asia, up of hundreds of 200-nm spatu- from India through New lae4. As a gecko walks along a Guinea. Tokay geckos are surface, these spatulae flat- one of the largest gecko ten against the substrate species, growing up to 51 cm material and form weak p u o in length and w eighing up to r chemical bonds through G g Nature America, Inc. All rights reserved. America, Inc. Nature n 400 g. -
Rules Amending Title 4
Rules Amending Title 4 Hawaii Administrative Rules September 26, 2017 1. Chapter 71 of Title 4, Hawaii Administrative Rules, entitled “Plant and Non-Domestic Animal Quarantine Non-Domestic Animal Import Rules” is amended and compiled to read as follows: “HAWAII ADMINISTRATIVE RULES” TITLE 4 DEPARTMENT OF AGRICULTURE SUBTITLE 6 DIVISION OF PLANT INDUSTRY CHAPTER 71 PLANT AND NON-DOMESTIC ANIMAL QUARANTINE NON-DOMESTIC ANIMAL IMPORT RULES Subchapter 1 General Provisions §4-71-1 Objective §4-71-2 Definitions §4-71-3 Permits §4-71-3.1 User permit fees 71-1 §4-71-4 Submission of permit application to the board §4-71-4.1 Maximum time period for permit approvals, disapprovals, extensions, or automatic approvals §4-71-4.2 Public input and notification for listing §4-71-4.3 Violations Subchapter 2 Non-Domestic Animal Introductions §4-71-5 Notice of quarantine §4-71-6 Prohibited introductions §4-71-6.1 Ad hoc panel for identification of prohibited hybrid animal §4-71-6.5 Permitted introductions §4-71-7 Bond for certain animals §4-71-8 Bonding procedure §4-71-9 Conditions for bonding §4-71-10 Failure to comply with bond conditions Historical note: Chapter 71 is based substantially upon Regulation 2 entitled "Concerning the Introduction of Feral and Other Non-Domestic Animals into Hawaii," of the Division of Entomology and Marketing, Department of Agriculture and Conservation [Eff. 12/12/41; am and ren. Regulation 2 8/30/47; am 9/16/60; R 7/13/81]; and Regulation 3 entitled "Concerning the Introduction of Bacteria, Fungi and Viruses into Hawaii," of the Division of Entomology, Board of Commissioners of Agriculture and Forestry [Eff.