Information for Adults with Eczema Contents Page
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pompholyx Factsheet Pompholyx Eczema (Also Known As Dyshidrotic Eczema/Dermatitis) Is a Type of Eczema That Usually Affects the Hands and Feet
12 Pompholyx factsheet Pompholyx eczema (also known as dyshidrotic eczema/dermatitis) is a type of eczema that usually affects the hands and feet. In most cases, pompholyx eczema involves the development of intensely itchy, watery blisters, mostly affecting the sides of the fingers, the palms of the hands and soles of the feet. Some people have pompholyx eczema on their hands and/or feet with other types of eczema elsewhere on the body. This condition can occur at any age but is usually seen in adults under 40, and is more common in women. The skin is initially very itchy with a burning sensation of heat and prickling in the palms and/or soles. Then comes a sudden crop of small blisters (vesicles), which turn into bigger weepy blisters, which can become infected, causing redness, pain, swelling and pustules. There is often subsequent peeling as the skin dries out, and then the skin can become red and dry with painful cracks (skin fissures). Pompholyx eczema can also affect the nail folds and skin around the nails, causing swelling (paronychia). What causes it? A reaction could be the result of contact with potential irritants such as soap, detergents, solvents, acids/alkalis, The exact causes of pompholyx eczema are not known, chemicals and soil, causing irritant contact dermatitis. Or although it is thought that factors such as stress, there could be an allergic reaction to a substance that is sensitivity to metal compounds (such as nickel, cobalt or not commonly regarded as an irritant, such as rubber or chromate), heat and sweating can aggravate this nickel, causing allergic contact dermatitis. -

Hand Dermatitis – Contact Dermatitis David E
3/2/2021 Hand Dermatitis – Contact Dermatitis David E. Cohen, M.D., M.P.H. Charles and Dorothea Harris Professor and Vice Chairman for Clinical Affairs Director of Allergic, Occupational and Environmental Dermatology New York University School of Medicine Department of Dermatology IEC 2021 Hand Eczema Virtual Symposium 1 •David E Cohen has declared the following financial interests: . Consultant and Honorarium: . Ferndale Laboratories, . Asana . Medimetriks . Leo . UCB . Cutanea [past] . Ferrer [past] . Celgene [past] . Novartis . Dermavant . FSJ . FIDE. (FIDE receives industry sponsorship from AbbVie, Almirall, Amgen, Bausch and Lomb, Bristol- Myers Squibb, Celgene Dermavant, Dermira, Janssen, Kyowa Hakko Kirin, LEO, Lilly, Novartis, Ortho Dermatologics, Pfizer, Sanofi Genzyme, Sun Pharma, UCB, Valeant) . Cosmetic Ingredient Review (CIR) •Stock or stock options: Dermira [past], Medimetriks [past], Brickell Biotech, Kadmon, Evommune, Timber •Board of Directors: Kadmon, Timber, Evommune, [Dermira-Past] I will discuss non-FDA approved patch test allergens, and emerging therapies 2 Hand Dermatitis • General population prevalence is 5% to 10% . Health care workers, exposed to wet work, frequent hand washing, and AD. Atopic dermatitis (AD) is recognized as the top risk factor Causes: • Exogenous: Irritant and Allergic Contact Dermatitis • Endogenous: Psoriasis, Dyshidrosis, Atopic Dermatitis, Nummular • ID • HYBRID • Spectrum for eczematous disease is vesicular and eroded to hyperkeratotic and fissured • Hand Psoriasis may have higher rates of allergic contact dermatitis. Int J Occup Environ Health. 2018 Jan 23:1-10. Ther Clin Risk Manag. 2020 Dec 31;16:1319-1332. doi: Contact Dermatitis. 2014 Jan;70(1):44-55. 10.2147/TCRM.S292504.eCollection 2020 Indian Dermatol Online J. 2012 Sep;3(3):177-81. -

Hand Dermatitis: Review of Etiology, Diagnosis, and Treatment
J Am Board Fam Med: first published as 10.3122/jabfm.2009.03.080118 on 8 May 2009. Downloaded from Hand Dermatitis: Review of Etiology, Diagnosis, and Treatment Adam D. Perry, MD, and John P. Trafeli, MD Hand dermatitis is a common condition seen in the primary care setting. Occupational exposures and frequent hand washing often lead to symptoms that are irritating and may cause discomfort. Irritant dermatitis, atopic hand dermatitis and contact hand dermatitis account for at least 70% of all diagnoses. A unifying feature in most cases is an underlying disruption in the stratum corneum, altering its barrier function. Transepidermal water loss increases with barrier disruption and is exacerbated by additional exposure to water. Precise diagnosis and subsequent treatment present a considerable challenge, and hand dermatitis often becomes chronic. Initial treatment should be aimed at controlling inflammation and restoring the skin’s natural barrier. Common management recommendations include the avoidance of irritants and potential allergens along with the use of emollients and topical corticosteroids to de- crease inflammation. Simple petroleum-based emollients are very effective at restoring hydration and repairing the stratum corneum. Referral to a Dermatologist or an Allergist may be necessary for pa- tients who require patch testing or those with refractory symptoms. (J Am Board Fam Med 2009;22: 325–30.) Hand dermatitis represents a large proportion of It is estimated that 5% to 7% of patients with occupation-associated skin disease. The prevalence hand dermatitis are characterized as having chronic among the general population has been estimated or severe symptoms and 2% to 4% of severe cases copyright. -

Seborrheic Dermatitis
432 Teams Dermatology Done by: Wael Al Saleh & Abdulrahman Al-Akeel Reviewer: Wael Al Saleh & Abdulrahman Al-Akeel 9 Team Leader: Basil Al Suwaine Color Code: Original, Team’s note, Important, Doctor’s note, Not important, Old teamwork 432 Dermatology Team Lecture 9: Atopic dermatitis/ Eczema Objectives 1- To know the definition & classification of Dermatitis/Eczema 2- To recognize the primary presentation of different types of eczema 3- To understand the possible pathogenesis of each type of eczema 4- To know the scheme of managements lines P a g e | 1 432 Dermatology Team Lecture 9: Atopic dermatitis/ Eczema Introduction: A groups and spectrum of related disorders with pruritus being the hallmark of the disease, they also come with dry skin. Every atopic dermatitis is eczema but not every eczema are atopic dermatitis. Atopic dermatitis mean that the patient has eczema (excoriated skin, itching and re-onset) and atopy (atopy; the patient or one of his family has allergic rhinitis, asthma or eczema). It starts early of life (eczema can happen at any time). It classified as: - Acute, characterized by erythema, papules, vesicles, oozing, and crusting. - Subacute, clinically it is represented by erythema, scaling, and crusting. - Chronic, presents with thickening of the skin, skin markings become prominent (lichenification); pigmentation and fissuring of the skin occur. Acute on top of chronic very dry 4 years old boy with chronic, itchy, well defined brownish plaque with bleeding plaques. lichenifications. Ill defined plaques Well defined erythematous excoriated Lichenification is the hallmark for plaques on both cheeks with erosion. chronic course. P a g e | 2 432 Dermatology Team Lecture 9: Atopic dermatitis/ Eczema Dermatitis Classification of dermatitis: Atopic, more common in children Seborrheic (oily skin)- (like naso-labial folds, scalp, ears) Contact dermatitis, substance cause eczema - Allergic - Irritant Nummular, coined shape, usually in the shin. -

Clinical Aspects of Irritant Contact Dermatitis Chapter 15 257
15_255_294 05.11.2005 10:22 Uhr Seite 255 Chapter 15 Clinical Aspects 15 of Irritant Contact Dermatitis Peter J. Frosch, Swen Malte John Contents multifactorial disease in most cases. Toxic chemicals 15.1 Definition . 255 (irritants) are the major cause, but mechanical, ther- mal, and climatic effects are important contributory 15.2 Clinical Pictures . 255 cofactors. The clinical spectrum of irritant contact 15.2.1 Chemical Burns . 256 dermatitis is much wider than that of allergic contact 15.2.2 Irritant Reactions . 259 dermatitis and ranges from slight scaling of the stra- 15.2.3 Acute Irritant Contact Dermatitis . 262 tum corneum, through redness, whealing, and deep 15.2.4 Chronic Irritant Contact Dermatitis . 268 15.2.5 Special Forms of Irritation . 273 caustic burns, to an eczematous condition indistin- 15.2.5.1 Climatic Factors . 273 guishable from allergic contact dermatitis. Acute 15.2.5.2 Aggravation of Endogenous Dermatoses forms of irritant contact dermatitis may be painful by Friction and Occlusion . 273 and may be associated with sensations such as burn- ing, stinging or itching. Individual susceptibility to 15.3 Epidemiology . 274 irritants is extremely variable. 15.4 Pathogenesis . 277 15.4.1 Exogenous Factors . 277 15.4.2 Endogenous Factors . 278 Core Message 15.4.3 Sensitive (Hyperirritable) Skin . 278 15.5 Diagnostic Tests í Irritant contact dermatitis is caused and Experimental Irritant Contact Dermatitis 280 by chemicals which damage skin structures 15.6 Action of Irritants in a direct nonallergic way. The clinical and Inflammatory Mediators . 281 picture is extremely variable and ranges 15.7 Quantification of the Irritant Response from chemical burns to chronic irritant (Bioengineering Techniques) . -

University of Groningen Hand Eczema Christoffers, Wianda
University of Groningen Hand eczema Christoffers, Wianda IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2014 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Christoffers, W. (2014). Hand eczema: interventions & contact allergies. [S.n.]. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license. More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne- amendment. Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 28-09-2021 Chapter 1 8 chapter 1 Introduction Hand eczema: interventions & contact allergies Wietske Andrea Christoffers Department of Dermatology, University of Groningen, University Medical Center Groningen, Groningen, Netherlands 9 chapter A few million years ago, our ancestors decided to start walking on two legs, which made it easier for them to collect food from high branches and to use tools. -
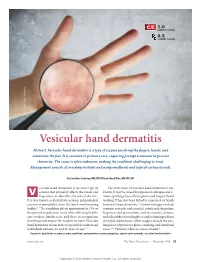
Vesicular Hand Dermatitis Abstract: Vesicular Hand Dermatitis Is a Type of Eczema Involving the fi Ngers, Hands, and Sometimes the Feet
1.0 CONTACT HOUR 0.5 CONTACT HOUR © Can Stock Photo / Peshkova Vesicular hand dermatitis Abstract: Vesicular hand dermatitis is a type of eczema involving the fi ngers, hands, and sometimes the feet. It is common in primary care, requiring prompt treatment to prevent chronicity. The cause is often unknown, making the condition challenging to treat. Management consists of avoiding irritants and using emollients and topical corticosteroids. By Geraldine Sobering, MN, NP, RN and Cheryl Dika, MN, NP, RN esicular hand dermatitis is an acute type of The exact cause of vesicular hand dermatitis is un- eczema that primarily affects the hands and known. It may be caused by exposure to allergens and ir- V fi ngers but can also affect the soles of the feet.1 ritants, prolonged use of latex gloves, and frequent hand It is also known as dyshidrotic eczema, palmoplantar washing. It has also been linked to a personal or family eczema, or pompholyx, from the Greek word meaning history of atopic dermatitis.1,2 Common triggers include bubble.2,3 The condition affects approximately 15% of exposure to metals such as nickel, cobalt, and chromium; the general population, most often affecting health- fragrances and preservatives used in cosmetics, lotions, care workers, hairdressers, and those in occupations and oils; rubber found in gloves; and certain ingredients that frequently expose the workers to water. Vesicular in topical medications. Other triggers include the pro- hand dermatitis occurs more frequently in women and longed use of protective gloves, smoking, and emotional individuals between 20 and 40 years of age.2,4-7 stress.2,5,8 However, often no cause is found.9 Keywords: dyshidrotic eczema, eczema, emollients, palmoplantar eczema, pompholyx, topical corticosteroids, vesicular hand dermatitis www.tnpj.com The Nurse Practitioner • November 2018 33 Copyright © 2018 Wolters Kluwer Health, Inc. -

Summer Is Near and Skin Issues Are Here
3/16/2021 DISCLOSURES • I have no disclosures • Off-label use of medications will be clearly labeled SUMMER IS NEAR AND SKIN ISSUES ARE HERE TANDY S. REPASS, MD 1 2 CLINICAL IMAGES CLINICAL IMAGES • DermNet New Zealand • www.dermnetnz.org • Unmodified images • https://creativecommons.org/licenses/by-nc-nd/3.0/nz/legalcode • Bolognia 3rd Edition • Edwards L. Genital Dermatology Atlas. Philadelphia: Lippincott Williams & Wilkins; 2004. 3 4 OBJECTIVES OBJECTIVES • Explore evidence-based practices related to • Explore evidence-based practices related to management of contact dermatitis, insect and management of contact dermatitis, insect and animal bites, and insect stings. animal bites, and insect stings. • Formulate effective strategies for managing • Formulate effective strategies for managing sunburns, burns, abrasions, abscesses, and fungal sunburns, burns, abrasions, abscesses, and fungal infections. infections. • Analyze management strategies for lacerations • Analyze management strategies for lacerations (suturing, Dermabond, medications, and follow-up). (suturing, Dermabond, medications, and follow-up). 5 6 1 3/16/2021 MANAGEMENT MANAGEMENT • Contact dermatitis • Contact dermatitis • Insect and animal bites • Insect and animal bites • Insect stings • Insect stings 7 8 CONTACT DERMATITIS CONTACT DERMATITIS • Irritant vs. allergic contact dermatitis • Irritant vs. allergic contact dermatitis • Allergic contact dermatitis • Allergic contact dermatitis • Poison ivy (urushiol) • Poison ivy (urushiol) • Nickel (chronic vs. acute) • Nickel (chronic vs. acute) • Balsam of Peru • Balsam of Peru • Neomycin • Neomycin • Formaldehyde • Formaldehyde • Special types of allergic contact dermatitis • Special types of allergic contact dermatitis • Photoallergic contact dermatitis • Photoallergic contact dermatitis • Airborne allergic contact dermatitis • Airborne allergic contact dermatitis • Stasis dermatitis • Stasis dermatitis • Hand dermatitis • Hand dermatitis • Management • Management 9 10 IRRITANT VS. -

Cutaneous Lupus Erythematosus; Epidemiology, Association with Sle and Comorbidity
From the Department of Clinical Sciences, Danderyd Hospital, Division of Dermatology, Karolinska Institutet, Stockholm, Sweden CUTANEOUS LUPUS ERYTHEMATOSUS; EPIDEMIOLOGY, ASSOCIATION WITH SLE AND COMORBIDITY Carina Grönhagen Stockholm 2012 Cover: A butterfly in Skåne, photograph taken by Gustaf Grönhagen. A “butterfly rash” is a typical manifestation of acute CLE and a butterfly is also the symbol of the European Society of cutaneous lupus erythematosus (EUSCLE). Previously published articles are reproduced with permission from the publishers. Published by Karolinska Institutet. Printed by US-AB Printcenter © Carina Grönhagen, 2012 ISBN 978-91-7457-605-4 Science is the literature of truth Josh Billings (Henry Wheeler Shaw) (1818-85) To Mum and Dad and Gustaf Abstract Lupus erythematosus (LE) is a disease that includes a broad spectrum of symptoms, from localized cutaneous LE (CLE) to severe systemic LE (SLE). Based on histopathological changes, the skin manifestations of LE can be divided into LE-specific (=CLE) and LE-non-specific manifestations. CLE is a chronic, inflammatory skin disease with a wide range of manifestations that can be seen in patients with or without SLE. As defined by clinical symptoms, average duration of symptoms, histological and serological findings, CLE can be further divided into three main subsets (acute CLE [ACLE], subacute CLE [SCLE] and chronic CLE [CCLE]). All four studies in this thesis focused on CLE and different comorbidities: the classification of cutaneous manifestations in SLE patients, the risk for progression to SLE, risk for cancer among CLE patients and the association between drug exposure and the development of subacute CLE. In study I we investigated the frequency of cutaneous manifestations in a cohort of 260 SLE patients. -

Dermatitis (Eczema) Including Occupational Dermatitis
Ministry of Defence Synopsis of Causation Dermatitis (Eczema) including Occupational Dermatitis Author: Dr Tony Woolfson, Medical Author, Medical Text, Edinburgh Validator: Professor Ian White, St John’s Dermatology Centre, St Thomas’ Hospital, London September 2008 Disclaimer This synopsis has been completed by medical practitioners. It is based on a literature search at the standard of a textbook of medicine and generalist review articles. It is not intended to be a meta-analysis of the literature on the condition specified. Every effort has been taken to ensure that the information contained in the synopsis is accurate and consistent with current knowledge and practice and to do this the synopsis has been subject to an external validation process by consultants in a relevant specialty nominated by the Royal Society of Medicine. The Ministry of Defence accepts full responsibility for the contents of this synopsis, and for any claims for loss, damage or injury arising from the use of this synopsis by the Ministry of Defence. 2 1. Definition 1.1. "Dermatitis" simply means inflammation of the skin and the term is used interchangeably with "eczema", defined as an inflammatory process of the skin characterised variably by erythema, oedema, vesiculation, scaling, fissuring and lichenification, depending on severity and chronicity2 . 1.2. Eczema is not a single disease entity, but describes a pattern of inflammatory responses originating in the dermis. The inflammation may be acute, subacute or chronic, each representing one stage in the evolution of the inflammatory process. 1.3. Dermatitis may usefully be divided into endogenous and exogenous types, depending on whether the main precipitating factor of the inflammatory response is within the body or is caused by some external agent. -

The Classification and Treatment of Hand Eczema
Peter Saitta, DO Associate Clinical Professor The Classification and Treatment of Hand Eczema 2 . Period prevalence . Risk factors . Classification systems . Differential diagnosis . First-line therapy options Objectives 3 . Prevalence . Number of new cases per time period . Period prevalence . Number of patients with outbreaks during a time period . Varies 2-10%1-3 Period Prevalence 4 STUDY NO AD / NO AD / NO AD / IRRITANT IRRITANT WATER IRRITANT WATER WATER EXPOSURE EXPOSURE EXPOSURE Meding et al. 1990 5-9% 14-23% 34-48% Nilsson et al. 1986 16% 38% 62-72% Rystedt et al. 1985 5% 37-50% 60-81% Hand Eczema Risks 5 . Atopic dermatitis .Lammintausta et al. 1991 .Coenraads et al. 1998 .Meding et al. 2000 .Meding et al. 2004 .Toledo et al. 2008 Hand Eczema Risks: Atopic Dermatitis 6 . Allergic rhinitis/asthma increases risk of hand eczema . But not more than atopic dermatitis4 Hand Eczema Risks: Allergic Rhinitis 7 and Asthma . Female gender increased risk . Coenraads et al. 1983 . Kavli et al. 1984 . Lantinga et al. 1984 . Bryld et al. 2000 . Yngveson et al. 2000 . Meding et al. 2001 . Mortz et al. 2001 . Dickel et al. 2002 Hand Eczema Risks: Female Gender 8 . Meding et al.5 . Wet work in 19-29 year-olds . 37.5% of women occupationally exposed . 18.2% of men . Learbek et al.6 . Private exposures Why Female Gender ? 9 STUDY TYPE OF STUDY INCIDENCE STUDY POPULATION (PER 100) Lantinga et al. Retrospective General 7.9 1984 Population Uter et al. 1994 Prospective Hairdressers 152 Smit et al. 1994 Prospective Hairdressers 328 Nurses 145 Brisman et al. -
Guide-Occupational-Dermatitis.Pdf
Recommendations for the Prevention, Detection and Management of Occupational Contact Dermatitis in Health Care Settings October 2019 Public Health Ontario Public Health Ontario is a Crown corporation dedicated to protecting and promoting the health of all Ontarians and reducing inequities in health. Public Health Ontario links public health practitioners, frontline health workers and researchers to the best scientific intelligence and knowledge from around the world. Public Health Ontario provides expert scientific and technical support to government, local public health units and health care providers relating to the following: • communicable and infectious diseases • infection prevention and control • environmental and occupational health • emergency preparedness • health promotion, chronic disease and injury prevention • public health laboratory services Public Health Ontario's work also includes surveillance, epidemiology, research, professional development and knowledge services. For more information, visit publichealthontario.ca. How to cite this document: Ontario Agency for Health Protection and Promotion (Public Health Ontario). Recommendations for the prevention, detection and management of occupational dermatitis in health care settings. Toronto, ON: Queen’s Printer for Ontario; 2019. ISBN 978-1-4868-3689-5 [PDF] Public Health Ontario acknowledges the financial support of the Ontario Government. ©Queen’s Printer for Ontario, 2019 Cover photo DermNet NZ. Irritant dermatitis [Internet]. Hamilton, NZ: DermNet New Zealand; 2003 [cited 2019 Oct 3]. Original picture provided by professor Raimo Suhonen. Available from: https://www.dermnetnz.org/topics/irritant-contact-dermatitis/. Used with permission. Recommendations for the Prevention, Detection and Management of Occupational Contact Dermatitis 2019 i Acknowledgements Public Health Ontario would like to thank Dr. Maureen Cividino, chair of the occupational dermatitis in health care committee (ODHCC), as well as Dr.