Fourth International Visual Field Symposium Bristol, April 13-16,198O
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Completing a Photography Exhibit Data Tag
Completing a Photography Exhibit Data Tag Current Data Tags are available at: https://unl.box.com/s/1ttnemphrd4szykl5t9xm1ofiezi86js Camera Make & Model: Indicate the brand and model of the camera, such as Google Pixel 2, Nikon Coolpix B500, or Canon EOS Rebel T7. Focus Type: • Fixed Focus means the photographer is not able to adjust the focal point. These cameras tend to have a large depth of field. This might include basic disposable cameras. • Auto Focus means the camera automatically adjusts the optics in the lens to bring the subject into focus. The camera typically selects what to focus on. However, the photographer may also be able to select the focal point using a touch screen for example, but the camera will automatically adjust the lens. This might include digital cameras and mobile device cameras, such as phones and tablets. • Manual Focus allows the photographer to manually adjust and control the lens’ focus by hand, usually by turning the focus ring. Camera Type: Indicate whether the camera is digital or film. (The following Questions are for Unit 2 and 3 exhibitors only.) Did you manually adjust the aperture, shutter speed, or ISO? Indicate whether you adjusted these settings to capture the photo. Note: Regardless of whether or not you adjusted these settings manually, you must still identify the images specific F Stop, Shutter Sped, ISO, and Focal Length settings. “Auto” is not an acceptable answer. Digital cameras automatically record this information for each photo captured. This information, referred to as Metadata, is attached to the image file and goes with it when the image is downloaded to a computer for example. -

Digital Camera Functions All Photography Is Based on the Same
Digital Camera Functions All photography is based on the same optical principle of viewing objects with our eyes. In both cases, light is reflected off of an object and passes through a lens, which focuses the light rays, onto the light sensitive retina, in the case of eyesight, or onto film or an image sensor the case of traditional or digital photography. The shutter is a curtain that is placed between the lens and the camera that briefly opens to let light hit the film in conventional photography or the image sensor in digital photography. The shutter speed refers to how long the curtain stays open to let light in. The higher the number, the shorter the time, and consequently, the less light gets in. So, a shutter speed of 1/60th of a second lets in half the amount of light than a speed of 1/30th of a second. For most normal pictures, shutter speeds range from 1/30th of a second to 1/100th of a second. A faster shutter speed, such as 1/500th of a second or 1/1000th of a second, would be used to take a picture of a fast moving object such as a race car; while a slow shutter speed would be used to take pictures in low-light situations, such as when taking pictures of the moon at night. Remember that the longer the shutter stays open, the more chance the image will be blurred because a person cannot usually hold a camera still for very long. A tripod or other support mechanism should almost always be used to stabilize the camera when slow shutter speeds are used. -
Take Home Primary Care Challenge “Blueprint Exam”
Take Home Primary Care Challenge “BLUEprint Exam” SECTION 2 1. A middle-aged man presents with chest pain. On examination there is a wide pulse pressure, hyperactive left ventricle, diastolic murmur along the left sternal border. ECG shows left ventricular hypertrophy. The most likely diagnosis is: a. Aortic stenosis b. Aortic regurgitation c. Mitral stenosis d. Mitral regurgitation e. Tricuspid stenosis 2. A 40-year-old patient states that for the last 10 years she has experienced recurrent throbbing headaches that are associated with visual disturbances. She experiences associated photophobia, nausea and vomiting with these headaches. Which of the following is the most likely explanation for these symptoms? a. Arteriovenous malformation b. Cluster headaches c. Migraine headaches d. Tension headaches e. Slow growing glioma 3. A 32 year-old female presents with complaints of gradual color change in a mole that has been present since birth. The patient also notes the recent onset of tenderness when her clothes rub up against it and itchiness for the past three weeks. An asymmetrical flat plaque with irregular and sharply defined margins with color variegation is noted on examination. Which of the following is the most appropriate diagnostic evaluation? a. Diascopy b. Patch testing. c. Acetowhitening d. Excisional biopsy 4. A patient presents with acute pain in his knee. The pain occurred abruptly and there was no preceding trauma. The knee is red and hot. Aspiration of the joint revealed negatively birefringent needle-shaped crystals with an increase in white cells but no bacteria on Gram stain. Which of the following is the most likely diagnosis? a. -

Shutter Speed in Digital Photography Stephen Sagers, Tooele County 4-H Agent Ron Patterson, Carbon County Ag/4-H Agent
March 2012 4H/Photography/2012-03pr Shutter Speed in Digital Photography Stephen Sagers, Tooele County 4-H Agent Ron Patterson, Carbon County Ag/4-H Agent Photography is the process of recording light. Film The Shutter cameras recorded the light on to the film while digital cameras record light on an image sensor. In The shutter is located behind the lens and mirrors order to prevent bright or dim light from creating an and opens when a photograph is taken. Most consumer cameras can shoot pictures with shutter overexposed or underexposed image the shutter th must open and close in the right amount of time. speeds from 1/2000 of a second to several seconds The amount of time it is opened depends on three (or indefinitely.) This feature is useful for freezing factors: the light intensity, the aperture setting, and motion or capturing effects like fireworks or the ISO or film speed. (Refer to separate factsheets running water. on ISO and aperture for a more detailed definition of these concepts.) In order to achieve proper exposure these three features must be balanced. The shutter speed is the easiest to adjust in order to obtain proper exposure. Exposure In digital photography exposure refers to the amount of light that reaches the image sensor. When too much light is recorded the picture will be washed out — overexposed. When too little light is recorded the image will be dark — underexposed. Figure 1. The inside of a film camera. The mirror Usually, neither situation is desirable. and shutter behind it move when it shoots a photograph. -

A Review of Selected Neurological Diseases Affecting Horses
MILNE LECTURE Neurology Is Not a Euphemism for Necropsy: A Review of Selected Neurological Diseases Affecting Horses Stephen M. Reed, DVM, Diplomate ACVIM Author’s address: Rood and Riddle Equine Hospital, PO Box 12070, Lexington, KY 40580; e-mail: [email protected]. © 2008 AAEP. 1. Introduction An increased level of understanding about the Disorders of the nervous system are serious and causes and management of equine neurological dis- often debilitating problems affecting horses. Refer- eases during the past 30 yr has resulted in consid- ence to equine neurological diseases can be found as erably less fear on the part of owners and early as 1860 when Dr. E. Mayhew described a con- veterinarians when faced with the statement that dition of partial paralysis in The Illustrated Horse “your horse is ataxic.” This increased awareness Doctor. Dr. Mayhew wrote that “with few excep- and knowledge about causes of ataxia in horses has tions a permanent neurologic gait deficit renders a made it routine for most equine veterinarians to in- horse unsuitable for use.” Although this is still at clude some level of neurological testing as part of their least partially correct today, there would be little physical examination. One need not look too hard to need to go further with today’s lecture if not for the identify articles on the role of the neurological exami- fact that much progress has been made in our un- nation as a part of the purchase, lameness, and even derstanding of how to better diagnose and treat exercise evaluation in horses. There are even articles neurological disorders affecting horses. -

PHOTO GUIDE for USAID PARTNERS
PHOTO GUIDE for USAID PARTNERS UPDATED ON 09/2020 USAID SHOOTING GUIDE FOR PARTNERS USAID SHOOTING GUIDE FOR PARTNERS GENERAL TIPS FOR CAPTURING VISUAL CONTENT PLAN AHEAD. Partners are encouraged to hire a professional photographer. Make sure to consult with USAID Development Outreach and Communications Specialists (DOCs) early about what they would like photographed or filmed. Think about what visuals will help meet USAID’s communications objectives. Plan on visiting the site in the morning and in the afternoon to see how the sunlight enhances the photo. Arrive at a site a few minutes early to walk through where you might stand to take your photos and find unique vantage points (can you take a photo from a window on the second floor?). BRING CONSENT FORMS. Consent forms are usually provided by the mission or embassy and should be in the local language. This consent form can be used as a starting point but it needs to be translated and approved by the relevant mission/embassy. CRAFT STATEMENT OF WORK. It is important to capture photo credit details in the Statement of Work (SOW) with the hired photographer. The SOW should note if any photos are owned by USG (and therefore open for public use if on USG publications) and if not, the photographer would need to give permission for photos used outside of the project. GET CLOSER. Don’t be afraid to move nearer to your subjects when appropriate. GENERAL TIPS FOR CAPTURING VISUAL CONTENT 2 | 18 USAID SHOOTING GUIDE FOR PARTNERS GENERAL TIPS FOR CAPTURING VISUAL CONTENT BE PATIENT. -

Opthalmology
OPTHALMOLOGY PRECOURSE WORKBOOK EYE ANATOMY Please watch this video before listening to the audio session. Anatomy of the Eye : https://www.osmosis.org/learn/Anatomy_and_physiology_of_the_eye HISTORY TAKING AND PHYSICAL EXAMINATION https://geekymedics.com/eye-examination-osce-guide/ REASON FOR VISIT/PRESENTING COMPLAINT Ask the main reason why the patient has come to seek an eye examination. Record the main presenting symptoms in the patient's own words and in a chronological order. The four main groups of symptoms are: 1. Red, sore, painful eye or eyes (including injury to the eye) 2. Decreased distance vision in one or both eyes, whether suddenly or gradually 3. A reduced ability to read small print or see near objects after the age of 40 years 4. Any other specific eye symptom, such as double vision, swelling of an eyelid, watering or squint. HISTORY OF PRESENTING COMPLAINT This is an elaboration of the presenting complaint and provides more detail. The patient should be encouraged to explain their complaint in detail and the person taking history should be a patient listener. While taking a history of the presenting complaint, it is important to have potential diagnoses in mind. For each complaint, ask about: • Onset (sudden or gradual) • Course (how it has progressed) • Duration (how long) • Severity • Location (involving one or both eyes) • Any relevant associated symptoms • Any similar problems in the past • Previous medical advice and any current medication. Compiled by Belmatt Healthcare from CKS NICE GUIDELINES PAST EYE HISTORY Ask for detail about any previous eye problems • History of similar eye complaints in the past. -
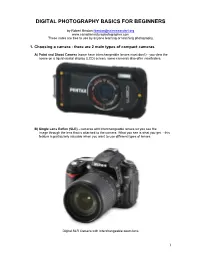
Digital Photography Basics for Beginners
DIGITAL PHOTOGRAPHY BASICS FOR BEGINNERS by Robert Berdan [email protected] www.canadiannaturephotographer.com These notes are free to use by anyone learning or teaching photography. 1. Choosing a camera - there are 2 main types of compact cameras A) Point and Shoot Camera (some have interchangeable lenses most don't) - you view the scene on a liquid crystal display (LCD) screen, some cameras also offer viewfinders. B) Single Lens Reflex (SLR) - cameras with interchangeable lenses let you see the image through the lens that is attached to the camera. What you see is what you get - this feature is particularly valuable when you want to use different types of lenses. Digital SLR Camera with Interchangeable zoom lens 1 Point and shoot cameras are small, light weight and can be carried in a pocket. These cameras tend to be cheaper then SLR cameras. Many of these cameras offer a built in macro mode allowing extreme close-up pictures. Generally the quality of the images on compact cameras is not as good as that from SLR cameras, but they are capable of taking professional quality images. SLR cameras are bigger and usually more expensive. SLRs can be used with a wide variety of interchangeable lenses such as telephoto lenses and macro lenses. SLR cameras offer excellent image quality, lots of features and accessories (some might argue too many features). SLR cameras also shoot a higher frame rates then compact cameras making them better for action photography. Their disadvantages include: higher cost, larger size and weight. They are called Single Lens Reflex, because you see through the lens attached to the camera, the light is reflected by a mirror through a prism and then the viewfinder. -

Abdominal Distension
2003 OSCE Handbook The world according to Kelly, Marshall, Shaw and Tripp Our OSCE group, like many, laboured away through 5th year preparing for the OSCE exam. The main thing we learnt was that our time was better spent practising our history taking and examination on each other, rather than with our noses in books. We therefore hope that by sharing the notes we compiled you will have more time for practice, as well as sparing you the trauma of feeling like you‟ve got to know everything about everything on the list. You don‟t! You can‟t swot for an OSCE in a library! This version is the same as the 2002 OSCE Handbook, except for the addition of the 2002 OSCE stations. We have used the following books where we needed reference material: th Oxford Handbook of Clinical Medicine, 4 Edition, R A Hope, J M Longmore, S K McManus and C A Wood-Allum, Oxford University Press, 1998 Oxford Handbook of Clinical Specialties, 5th Edition, J A B Collier, J M Longmore, T Duncan Brown, Oxford University Press, 1999 N J Talley and S O‟Connor, Clinical Examination – a Systematic Guide to Physical Diagnosis, Third Edition, MacLennan & Petty Pty Ltd, 1998 J. Murtagh, General Practice, McGraw-Hill, 1994 These are good books – buy them! Warning: This document is intended to help you cram for your OSEC. It is not intended as a clinical reference, and should not be used for making real life decisions. We‟ve done our best to be accurate, but don‟t accept any responsibility for exam failure as a result of bloopers…. -
View / Download Pdf Version of This Article
GIANT CELL ARTERITIS: Always keep it in your head 16 Giant cell arteritis, also referred to as temporal arteritis, is a form of vasculitis which predominantly affects older people. It must be treated urgently, as it is associated with a significant risk of permanent visual loss, stroke, aneurysm and possible death. A low threshold for suspicion and prompt corticosteroid treatment are essential to prevent these complications. However, arriving at a diagnosis of this enigmatic condition can be difficult, as patients can present with non-specific symptoms. Referring the patient for a temporal artery biopsy is a key aspect of confirming the diagnosis, but this must not delay the initiation of corticosteroid treatment if giant cell arteritis is suspected. If undetected, giant cell arteritis can result in catastrophic A headache not to miss sequelae, such as irreversible visual loss, stroke and aortic Giant cell arteritis is an immune-mediated, ischaemic aneurysm. Visual loss, due to ischaemic optic neuropathy, is condition caused by inflammation in the wall of medium to an early manifestation and can be a presenting symptom. This large arteries. While it can affect all medium to large arteries occurs in 20 – 50% of people with giant cell arteritis if they are in the head, neck and upper torso, the involvement of the untreated.5, 6 Large-vessel stenosis, and with it an increased risk temporal artery is usually the only artery in which physical of stroke, occurs in 10 – 15% of people.7, 8 Prompt treatment changes are clinically apparent (giving rise to the alternative with corticosteroids can markedly reduce these risks. -
Camera Settings Guide
Camera Settings Guide • " " and " " are trademarks or registered trademarks of Sony Corporation. • All other company and product names mentioned herein are used for identification purposes only and may be the trademarks or registered trademarks of their respective owners. TM and ® symbols are not included in this booklet. • Screen displays and effects used to illustrate some functions are simulated. Conventional autofocus has until now dealt with space alone. Sony goes one step further — a big step, with an innovative image sensor that picks up both space and time to capture moving subjects with new clarity. Sony spells the beginning of a new autofocus era. 4D FOCUS allows you to take crisper photos than ever. Plain old autofocus is a thing of the past. The future of photography is in motion. What is 4D FOCUS? Space: 3D Time: 4D 4D FOCUS Area Depth Time Wide Fast Steadfast The wide AF area, covering nearly the Fast Hybrid AF, combining phase- An advanced AF algorithm accurately entire frame, allows focusing on a detection AF and contrast-detection AF, predicts subject’s next move. Precise AF subject positioned even off the center instantly detects distance to the subject tracking allows focus to be maintained of the frame. to focus accurately. even on fast-moving subjects. Meeting your focusing demands Basic AF performance of Wide Fast Steadfast Focusing over wide area Instant focusing! Once it's focused, it never lets go The 6000 employs a focal plane phase- Advanced Fast Hybrid AF combines phase- With Focus Mode set to AF-C, the camera detection AF sensor with 179 AF points spread detection AF and contrast-detection AF to achieve displays one or more small green frames to cover nearly the entire frame. -

SONY Alpha 3000 Manual FILMP/MEDP 150/160 • M. Lucas
SONY Alpha 3000 Manual FILMP/MEDP 150/160 • M. Lucas The Sony Alpha 3000 looks like a DSLR, but it actually is closer to a video camera in an SLR body, AKA a “mirrorless” camera. It records a 20MB still image (5456 x 3632 pixels!) and can be set for JPEG or RAW + JPEG. The camera comes with a battery, a charger, a lens cap, a lens hood and a shoulder strap. The lens has a UV filter, which can be cleaned without damaging the lens. There are two kinds of chargers, one where you plug in the camera, and the other where you just put the battery in the charger, a better idea. The batteries should last through more than one day of shooting. But they should be charged at least once a week. The camera stores images on an SD card, which is in a slot as shown. Be careful with the door covering the card. The card removes by pushing it in, and springing it out. Side door for SD card and charger. Using the Camera The viewfinder is electronic, giving you the same image you see on the back viewscreen. There is a button on the top right to switch between the two ways of viewing next to the Mode Wheel. (see below) The viewfinder is good for situations that are too bright for the rear screen, but not great for critical viewing. The lens is interchangeable. It is an E‐mount lens, which is a new Sony mount. So adaptors are needed for other lenses like Canon or Nikon.