Baseline Household Survey Swabi District May 2010
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

University of Engineering & Technology, Mardan
UNIVERSITY OF ENGINEERING & TECHNOLOGY, MARDAN APPLICATION Of THE ELIGIBLE CANDIDATE FOR THE POSITION OF JUNIOR CLERK (BPS-11) ON REGULAR BASIS UET MARDAN S. NO NAME FATHER NAME CONTACT NO ELIGIBLE/UN- Address REMARKS ELIGIBLE 1. Hamid Zaman Musafar 0348-9736381 Eligible Village kandar kas post office kata khat district Mardan 2. Muhammad Sheraz Nawaz Khan 0342-4204474 Eligible House No.151Nothia Pathali Nawaz Peshawar 3. Fazl-e- Allam Fazl-e-Wahid 0313-8156464 Eligible House # 49, Street # 03, Sector (P) Sheikh Malton Mardan 4. Mubassar Iqbal Said Ameer 0333-6008367 Eligible Dist & The: CChakwal Mohallah Sargajra Gharbi Wear Grid Station Talagung Road Chakwal City 5. Ashfaq Ahmad Saif Ur Rehman 0341-9112007 Eligible Mir alam khan korona sardheri District Charsada 6. Adil Iqbal Hussain 0334-9132037 Eligible 289 Abbasid Street Mardan Cantt Mardan 7. Sadiq Ur Rahman Atiq Ur Rehman 0334-2914660 Eligible Gul Shan Colony Nisatta Road Janabad 8. Ashraf Ali Niaz Ali 0345-9239491 Eligible Village & P/O Pir Abad Teh. Takht Bahi Distt. Mardan 9. Muhammad Zubair Saad Ullah 0346-9228618 Eligible Mufti Pur P/O manga Dergai Sardheri District & Teh.Charsada 10. Muhammad Ehsan Fazli Subhan 0301-8939636 Eligible Moallah Dowgoon Village Kaga Wala P.O Bada ber tehsil & District Peshawar 11. Jawad Faisal Shah Zaman Khan 0316-9416828 Eligible Model Town Mattar road House # 52 Haripur. 12. Muhammad Nawab Ali 0333-8584252 Eligible Moh. Tawan Khel Garhi Ismail Shahzad Khan Zai Gharri Kapura Mardan 13. Muhammad Younas Noor Muhmmad 0311-9992853 Eligible Koragh Road Chota Rashaki Afridi Mardan 14. Ashfaq Ahmad Karim Khan 0314-9391300 Eligible Moh. -

Genetic Analysis of the Major Tribes of Buner and Swabi Areas Through Dental Morphology and Dna Analysis
GENETIC ANALYSIS OF THE MAJOR TRIBES OF BUNER AND SWABI AREAS THROUGH DENTAL MORPHOLOGY AND DNA ANALYSIS MUHAMMAD TARIQ DEPARTMENT OF GENETICS HAZARA UNIVERSITY MANSEHRA 2017 I HAZARA UNIVERSITY MANSEHRA Department of Genetics GENETIC ANALYSIS OF THE MAJOR TRIBES OF BUNER AND SWABI AREAS THROUGH DENTAL MORPHOLOGY AND DNA ANALYSIS By Muhammad Tariq This research study has been conducted and reported as partial fulfillment of the requirements of PhD degree in Genetics awarded by Hazara University Mansehra, Pakistan Mansehra The Friday 17, February 2017 I ABSTRACT This dissertation is part of the Higher Education Commission of Pakistan (HEC) funded project, “Enthnogenetic elaboration of KP through Dental Morphology and DNA analysis”. This study focused on five major ethnic groups (Gujars, Jadoons, Syeds, Tanolis, and Yousafzais) of Buner and Swabi Districts, Khyber Pakhtunkhwa Province, Pakistan, through investigations of variations in morphological traits of the permanent tooth crown, and by molecular anthropology based on mitochondrial and Y-chromosome DNA analyses. The frequencies of seven dental traits, of the Arizona State University Dental Anthropology System (ASUDAS) were scored as 17 tooth- trait combinations for each sample, encompassing a total sample size of 688 individuals. These data were compared to data collected in an identical fashion among samples of prehistoric inhabitants of the Indus Valley, southern Central Asia, and west-central peninsular India, as well as to samples of living members of ethnic groups from Abbottabad, Chitral, Haripur, and Mansehra Districts, Khyber Pakhtunkhwa and to samples of living members of ethnic groups residing in Gilgit-Baltistan. Similarities in dental trait frequencies were assessed with C.A.B. -

Contesting Candidates NA-1 Peshawar-I
Form-V: List of Contesting Candidates NA-1 Peshawar-I Serial No Name of contestng candidate in Address of contesting candidate Symbol Urdu Alphbeticl order Allotted 1 Sahibzada PO Ashrafia Colony, Mohala Afghan Cow Colony, Peshawar Akram Khan 2 H # 3/2, Mohala Raza Shah Shaheed Road, Lantern Bilour House, Peshawar Alhaj Ghulam Ahmad Bilour 3 Shangar PO Bara, Tehsil Bara, Khyber Agency, Kite Presented at Moh. Gul Abad, Bazid Khel, PO Bashir Ahmad Afridi Badh Ber, Distt Peshawar 4 Shaheen Muslim Town, Peshawar Suitcase Pir Abdur Rehman 5 Karim Pura, H # 282-B/20, St 2, Sheikhabad 2, Chiragh Peshawar (Lamp) Jan Alam Khan Paracha 6 H # 1960, Mohala Usman Street Warsak Road, Book Peshawar Haji Shah Nawaz 7 Fazal Haq Baba Yakatoot, PO Chowk Yadgar, H Ladder !"#$%&'() # 1413, Peshawar Hazrat Muhammad alias Babo Maavia 8 Outside Lahore Gate PO Karim Pura, Peshawar BUS *!+,.-/01!234 Khalid Tanveer Rohela Advocate 9 Inside Yakatoot, PO Chowk Yadgar, H # 1371, Key 5 67'8 Peshawar Syed Muhammad Sibtain Taj Agha 10 H # 070, Mohala Afghan Colony, Peshawar Scale 9 Shabir Ahmad Khan 11 Chamkani, Gulbahar Colony 2, Peshawar Umbrella :;< Tariq Saeed 12 Rehman Housing Society, Warsak Road, Fist 8= Kababiyan, Peshawar Amir Syed Monday, April 22, 2013 6:00:18 PM Contesting candidates Page 1 of 176 13 Outside Lahori Gate, Gulbahar Road, H # 245, Tap >?@A= Mohala Sheikh Abad 1, Peshawar Aamir Shehzad Hashmi 14 2 Zaman Park Zaman, Lahore Bat B Imran Khan 15 Shadman Colony # 3, Panal House, PO Warsad Tiger CDE' Road, Peshawar Muhammad Afzal Khan Panyala 16 House # 70/B, Street 2,Gulbahar#1,PO Arrow FGH!I' Gulbahar, Peshawar Muhammad Zulfiqar Afghani 17 Inside Asiya Gate, Moh. -

Mardan (Posts-1) Scoring Key: Grade Wise Marks 1St Div: 2Nd Div: 3Rd Div: Age 25-35 Years 1
At least 2nd Division Master in Social Sciences (Social Work/ Sociology will be preferred) District: Mardan (Posts-1) Scoring Key: Grade wise marks 1st Div: 2nd Div: 3rd Div: Age 25-35 Years 1. (a) Basic qualification Marks 60 S.S.C 15 11 9 Date of Advertisement:- 22-08-2020 2. Higher Qualification Marks (One Step above-7 Marks, Two Stage Above-10 Marks) 10 F.A/FSc 15 11 9 SOCIAL CASE WORKER (BPS-16) 3. Experience Certificate 15 BA/BSc 15 11 9 4. Interviews Marks 8 MA/MSc 15 11 9 5. Professional Training Marks 7 Total;- 60 44 36 Total;- 100 LIST OF CANDIDATES FOR APPOINTMENT TO THE POST OF SOCIAL CASE WORKER BPS-16 BASIC QUALIFICATION Higher Qual: SSC FA/FSC BA/BSc M.A/ MS.c S. # on Name/Father's Name and address Total S. # Appli: Remarks Domicile Malrks= 7 Total Marks Marks Marks Marks Marks Date of Birth Qualification Division Division Division Division Marks P.HD Marks M.Phil Marks of Experience Professional/Training One Stage Above 7 Two Two Stage Above 10 Interview Marks 8 Marks Year of Experience 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 Mr. Farhan Raza S/O Abid Raza, Koz Kaly Madyan, P.O Madyan, Tehsil and District Swat, 0314- Mphil Agriculture Rual 71 3/2/1992 Swat 1st 15 1st 15 1st 15 1st 15 10 70 70 9818407 Sociology Mr. Muhammad Asif Khan S/O Muhammad Naeem Khan, Rahat Abad Colony, Bannu Road P.O PHD Business 494 16-04-1990 Lakki Marwat 1st 15 1st 15 1st 15 1st 15 10 70 70 Sheikh Yousaf District D.I.Khan. -

Religious Transformation and Development Among the Pakhtuns: a Historical and Analytical Study
Religious Transformation and Development among the Pakhtuns: A Historical and Analytical Study Himayatullah ∗ Like their inaccessible hilly terrain hidden away in huge mountains the origin of the Pakhtuns is also shrouded in mystery. There are various theories put forward by different scholars and historians regarding their origin. The first theory, which was propounded by Niamatullah in Makhzan-i-Afghani, was that, the Pakhtuns are the descendants of Hazrat Yaqub (A.S), which means they are of Bani Israelite origin. It goes on to say that the Pakhtuns collectively embraced Islam on the invitation of Hazrat Khalid bin Walid during the lifetime of Hazrat Muhammad (SAW). 1 The proponents of the Bani Israelite theory considered Khalid bin Walid a descendant of that Jewish community who migrated from Babul to Medina. Another theory regarding the origin of the Pakhtuns is that they belong to those Aryans who laid the foundation of an advanced culture at about 1500 B.C. It has been stated that the Aryans, on account of natural calamities, left their original homeland Central Asia and settled in the area of Bakhtar in Afghanistan in the shape of different tribes. In the fields of Bakhtar they spent their days and nights. After some time with increase in their population, the area remained not helpful and productive for them. Therefore, they started migrating from Bakhtar in groups in different phases. After the migration of two main branches from Bakhtar, the remaining Aryans left behind, decided of permanent settlement in Bakhtar. They are known as the ‘Aryans of Bakhtar’ or the ‘Central Aryans’. -

List of Unclaimed Dividends and Shares
Ferozsons Laboratories Limited List of Unclaimed Dividend & Bonus Amount of No. of Unclaimed S.No Folio Name Address CNIC Unclaimed Dividend Shares (Rupees) 1 0005 Mr. Abdul Hamid Khan C/O Ferozsons Limited 60 The Mall, Lahore. 00000-0000000-0 499 117,337 2 0011 Mr. Mohammad Javid Khan, Pak International Printers 118 - G. T. Road Lahore. 00000-0000000-0 8 3,806 3 0012 Begum Abdul Majid Khan C/O Pakistan International Printers,118-G.T.Road, Lahore. 00000-0000000-0 718 308,023 4 0017 Miss Kaukab Sadiq 64 / E - 1, Gulberg - III Lahore. 00000-0000000-0 1724 301,856 5 0019 Imtiaz Begum Sahiba 64 / E - 1, Gulberg - III Lahore. 00000-0000000-0 143 24,882 6 0028 Mr. Abdul Razzaq H.No.815,St.64, G-9/4 Islamabad 00000-0000000-0 902 156,010 7 0035 Mr. Shams-ul-Hassan Khawaja Pharmaceutical Section Ministry of Health Al-Riyadh 00000-0000000-0 236 40,960 8 0043 Mrs. Shujaat Parveen Vill: & P. O.Toru Mardan. 00000-0000000-0 1056 1,292,201 9 0050 Mrs. Khawar Kazi L - 102, D. H. A. Lahore Cantt. 35201-8757810-4 0 2,029 10 0059 Mr. Tahir Ali Khan H.No.280,St.38, G-9/1, Islamabad 00000-0000000-0 4423 759,766 11 0060 Mr. Abdul Qadir Khan Retd.Veterinary Doctor Kacha Gojra Faisalabad. 00000-0000000-0 1874 323,753 12 0063 Mr. Said Ahmed Shah House # 64 Biket Ganj Street Mardan. 00000-0000000-0 210 318,085 13 0065 Dr. Mrs. Farrakh Iqbal A-572 Block 5, Gulshan-e-Iqbal, Karachi 75300 42201-5619562-0 0 11,332 14 0066 Mr. -

Swabi Blockwise
POPULATION AND HOUSEHOLD DETAIL FROM BLOCK TO DISTRICT LEVEL KHYBER PAKHTUNKHWA (SWABI DISTRICT) ADMIN UNIT POPULATION NO OF HH SWABI DISTRICT 1,624,616 214,209 LAHOR TEHSIL 306,168 39,528 LAHOR I QH 264,748 34113 ANBAR PC 17,437 2227 ANBAR 10,625 1331 033010201 1,928 255 033010202 1,764 223 033010203 634 80 033010204 884 122 033010209 2,537 306 033010210 1,382 144 033010211 1,496 201 JANGI DHER 2,756 341 033010207 775 87 033010208 1,981 254 SHEIKH DHERI 4,056 555 033010205 1,926 252 033010206 1,722 217 033010212 408 86 BEKA PC 16,758 1978 BEKA 11,209 1345 033010301 1,713 222 033010302 1,685 213 033010303 1,589 207 033010304 1,102 140 033010305 2,262 235 033010310 1,283 164 033010311 1,575 164 NABI 5,549 633 033010306 1,902 228 033010307 1,316 144 033010308 1,357 131 033010309 974 130 HARYAN PC 8,400 1141 DHERI ZAKRIA 1,259 189 033010403 1,259 189 HARYAN 3,251 430 033010401 1,384 157 033010404 434 71 033010405 1,433 202 SALLAH 3,890 522 033010402 1,130 157 033010406 911 107 033010407 1,849 258 HUND PC 11,435 1505 HUND 11,435 1505 Page 1 of 32 POPULATION AND HOUSEHOLD DETAIL FROM BLOCK TO DISTRICT LEVEL KHYBER PAKHTUNKHWA (SWABI DISTRICT) ADMIN UNIT POPULATION NO OF HH 033010101 812 69 033010102 299 49 033010103 460 74 033010104 713 106 033010105 239 44 033010106 452 76 033010107 423 69 033010108 1,007 121 033010109 454 67 033010110 679 81 033010111 608 78 033010112 437 70 033010113 1,385 149 033010114 248 40 033010115 562 69 033010116 648 94 033010117 266 38 033010118 730 101 033010119 748 70 033010120 265 40 JAHANGIRA PC 42,081 4952 -
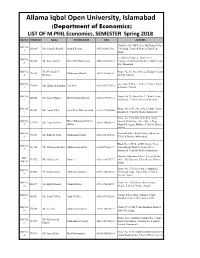
Allama Iqbal Open University, Islamabad (Department of Economics) LIST of M.PHIL Economics, SEMESTER Spring 2018 Roll No FORM NO Name FATHER NAME CNIC ADDRESS
Allama Iqbal Open University, Islamabad (Department of Economics) LIST OF M.PHIL Economics, SEMESTER Spring 2018 Roll No FORM NO Name FATHER NAME CNIC ADDRESS Chak No 286, GB II, Near By Rajana Toba Roll No 215685 Ms. Shamila Khalid Khalid Pervaz 33303-63601202 Tek Singh, Tehsil & District Toba Tek 1 Singh C/o Shahzad Ahmed, Block No. 4, Roll No 382384 Mr. Israr Ahmad Rana Din Muhammad 36603-8306381-3 Computer Lab, Room No 210, AIOU, Sector 2 H-8, Islamabad Roll No Mr. Mehboob Ur House No. 61, Street No. 2, Zaildaar Colony 378423 Muhammad Jamil 36502-6305513-5 3 Rehman 82/6-R, Sahiwal Roll No Government Degree College Chitral, Tehsil 378615 Mr. Ghani Ur Rahman Zar Wali 15201-0572307-1 4 & District Chitral Roll No House No. 79, Street No. 21, Rawal Town, 384055 Ms. Laraib Hassan Hafiz Ghulam Hassan 32103-0903961-2 5 Islamabad, Tehsil & District Islamabad Roll No. House No. 1276, Street No 3, Model Town 104223 Ms. Anam Tahir Syed Tahir Hussain Shah 61101-7909382-6 6 Islamabad, Tehsil & District Islamabad House No. 1220/6M, Mohala Neelgran Roll No Haji Muhammad Saleem Outside Dehli Gate, Street No. 1, Near 379936 Ms. Anum Saleem 36302-1466511-2 7 Akhtar Masjid Neelgran, Multan , Tehsil & District Multan Roll No Mohallah Khan, Khail Village Dhamtour, 378258 Ms. Raheela Sadiq Muhammad Sadiq 13101-6272715-4 8 Tehsil & District Abbottabad Block No. 3, B/16, AGPR Colony, Near Roll No 111182 Mr. Muhammad Nasir Muhammad Ashraf 41204-0946621-9 Imam Bargah Market, Sector G-9/2, 9 Islamabad, Tehsil & District Islamabad Mohalla Muhammad Khel, Village & Post Roll 378172 Mr. -

Zootheraputic Practices in Swabi District of Khyber Pakhtunkhawa Pakistan
Pure Appl. Biol., 8(1): 222-231, March, 2019 http://dx.doi.org/10.19045/bspab.2018.700180 Research Article Zootheraputic practices in Swabi district of Khyber Pakhtunkhawa Pakistan Waqas Ahmad Shams1*, Gauhar Rehman1, Zahid Ullah2, Sumbal Ara1, Sadaf Niaz1, Abid Ali1, Khurshid Khan1, Huma Alam1, Nida Gul1, Tahira Naz1, Saif ul Islam3 and Abdul Jamil khan1 1. Department of Zoology, Abdul Wali Khan University Mardan Khyber Paktunkhwa-Pakistan 2. Department of Zoology, University of Buner Khyber Paktunkhwa-Pakistan 3. Department of Zoology, Government Degree College Lahor Swabi, Khyber Paktunkhwa-Pakistan *Corresponding author’s email: [email protected] Citation Waqas Ahmad Shams, Gauhar Rehman, Zahid Ullah, Sumbal Ara, Sadaf Niaz, Abid Ali, Khurshid Khan, Huma Alam. Nida Gul, Tahira Naz, Saif ul Islam and Abdul Jamil Khan. Zootheraputic practices in Swabi district of Khyber Pakhtunkhawa Pakistan. Pure and Applied Biology. Vol. 8, Issue 1, pp222-231. http://dx.doi.org/10.19045/bspab.2018.700180 Received: 22/07/2018 Revised: 11/10/2018 Accepted: 21/10/2018 Online First: 02/11/2018 Abstract The use of animals for therapeutic purpose is an important filed from ancient time. They utilize animals for different purposes like art, religion, music, and literature. In Zoo therapy different parts of the animal body, their products, or non-animal materials such as nests and cocoon are used. It has an important contribution to understanding traditional subsistence and medical knowledge and practices. The present study is intended to look into different zoo therapeutic medicinal uses in the traditional health care system among the native inhabitants of district Swabi, Khyber PakhtunKhawa Pakistan. -

District Wise Details of De-Registered Npos / Ngos Registered Under the Societies Registration Act, 1860
DISTRICT WISE DETAILS OF DE-REGISTERED NPOS / NGOS REGISTERED UNDER THE SOCIETIES REGISTRATION ACT, 1860 District Chitral Upper S.No. Name of NPOs Address 1. Shoungush Youth Welfare Organization Ohoshush Owir Chitral (Upper) 2. Shami Welfare Society Village Chinar, Tehsil Mastuj, District Chitral (Upper) District Chitral Lower S.No. Name of NPOs Address 1. Nidaul Harmain Shar e faine Foundation Gool Door Near Old Zari Bank District Chitral (Lower) 2. Alian Foundation Village Alyian Near Chitral Scouts Cantt Teh & Dist Chitral (Lower) 3. Association for Sustainable Development (ASD) Chinar Inn Market Office No 26 Shahi Chitral (lower) 4. ANWAAZ Polo ground Main bazar Garam Chashma Chitral (Lower) KP District Dir Upper S.No. Name of NPOs Address 1. Socio Economic Advancement Society (SEAS) Main Bazar Wari Dir upper District Dir Lower S.No. Name of NPOs Address 1. Social Workers Awareness& Rural Development Naway Kalay Nasafa Talaah Tehsil Temergarah district Dir Lower (SWARD) 2. Social Awareness and Rural Development Temergarah district Dir Lower 3. Human Relief Trust Chakdara opposite to ID card office university road chakdara Dir lower 4. Organization for Human Development Program (CHDP) 3rd Floor Sanna Market China Plaza Chakdara The Adenzai district Dir Lower 5. Agency for Change & Transparency Timergara, district Dir Lower, Khyber Pakhtunkhwa, Pakistan. 6. Zoonoses Control Committee (ZCC) PCA Form Services Bypass Road Timergarah Dir Lower 7. Helping People Foundation (HPF) Gulabad Tehsil Adenzai District Lower Dir KP 8. Health Education Disaster Vulnerable Area Identification Dir Lower Tehsil Adenzai PO Chakdara Mandi program (MEDVAIP) NGO 9. Qalam Foundation Temergarah District Dir Lower. District Dera Ismail Khan S.No. -

Pakistan Agricultural Storage and Services Corporation
Table of Contents Table of Contents ................................................................................................................... 1 List of acronyms...................................................................................................................... 3 Assessment Team Members ................................................................................................... 4 Executive Summary ................................................................................................................ 6 I. Crisis Storyline ................................................................................................................... 10 2.1 Rationale and Objectives.........................................................................................................................12 2.2 Methodology............................................................................................................................................13 2.3 Limitations................................................................................................................................................16 III. Population and Markets in the Crisis Areas...................................................................... 17 3.1 High Food Inflation Rates: continuing to burden the population...............................................................18 IV. Trade across Crisis Areas: more difficult and more expensive .......................................... 20 4.1 Current Hot Spots (FATA): market -

1 Annexure - D Names of Village / Neighbourhood Councils Alongwith Seats Detail of Khyber Pakhtunkhwa
1 Annexure - D Names of Village / Neighbourhood Councils alongwith seats detail of Khyber Pakhtunkhwa No. of General Seats in No. of Seats in VC/NC (Categories) Names of S. Names of Tehsil Councils No falling in each Neighbourhood Village N/Hood Total Col Peasants/Work S. No. Village Councils (VC) S. No. Women Youth Minority . district Council Councils (NC) Councils Councils 7+8 ers 1 2 3 4 5 6 7 8 9 10 11 12 13 Abbottabad District Council 1 1 Dalola-I 1 Malik Pura Urban-I 7 7 14 4 2 2 2 2 Dalola-II 2 Malik Pura Urban-II 7 7 14 4 2 2 2 3 Dabban-I 3 Malik Pura Urban-III 5 8 13 4 2 2 2 4 Dabban-II 4 Central Urban-I 7 7 14 4 2 2 2 5 Boi-I 5 Central Urban-II 7 7 14 4 2 2 2 6 Boi-II 6 Central Urban-III 7 7 14 4 2 2 2 7 Sambli Dheri 7 Khola Kehal 7 7 14 4 2 2 2 8 Bandi Pahar 8 Upper Kehal 5 7 12 4 2 2 2 9 Upper Kukmang 9 Kehal 5 8 13 4 2 2 2 10 Central Kukmang 10 Nawa Sher Urban 5 10 15 4 2 2 2 11 Kukmang 11 Nawansher Dhodial 6 10 16 4 2 2 2 12 Pattan Khurd 5 5 2 1 1 1 13 Nambal-I 5 5 2 1 1 1 14 Nambal-II 6 6 2 1 1 1 Abbottabad 15 Majuhan-I 7 7 2 1 1 1 16 Majuhan-II 6 6 2 1 1 1 17 Pattan Kalan-I 5 5 2 1 1 1 18 Pattan Kalan-II 6 6 2 1 1 1 19 Pattan Kalan-III 6 6 2 1 1 1 20 Sialkot 6 6 2 1 1 1 21 Bandi Chamiali 6 6 2 1 1 1 22 Bakot-I 7 7 2 1 1 1 23 Bakot-II 6 6 2 1 1 1 24 Bakot-III 6 6 2 1 1 1 25 Moolia-I 6 6 2 1 1 1 26 Moolia-II 6 6 2 1 1 1 1 Abbottabad No.