Training a Healthy Junior Tennis Player Neeru Jayanthi, M.D
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
WTA Tour Statistical Abstract 1999
WTA Tour Statistical Abstract 1999 Robert B. Waltz ©1999 by Robert B. Waltz and Tennis News Reproduction and/or distribution for profit prohibited Contents Introduction Head to Head — Results Winning Percentage on Hardcourts against Top Players Points Per Tournament on Hardcourts 1999 In Review: The Top Best and Worst Results on Hardcourts The Top 20 Head to Head Players Clay The Final Top Twenty-Five Wins Over Top Players Summary of Clay Results The Beginning Top Twenty Matches Played/Won against the (Final) Winning Percentage on Clay Summary of Changes, beginning to end Top Twenty Points Per Tournament on Clay of 1999 Won/Lost Versus the Top Players Best and Worst Results on Clay (Based on Rankings at the Time of All the Players in the Top Ten in Grass 1999 the Match) Won/Lost Versus the Top Players Summary of Grass Results The Complete Top Ten Based on WTA (Based on Final Rankings) (Best 18) Statistics Indoors The Complete Top Ten under the 1996 Statistics/Rankings Based on Summary of Indoor Results Ranking System Head-to-Head Numbers Winning Percentage Indoors Points Per Tournament Indoors Ranking Fluctuation Total Wins over Top Ten Players Best and Worst Results Indoors Top Players Sorted by Median Ranking Winning Percentage against Top Ten Players All-Surface Players Tournament Results Wins Against Top Ten Players Tournament Wins by Surface Tournaments Played/Summary of Analysed Results for Top Players Assorted Statistics Tournament Winners by Date (High- How They Earned Their Points Tier Events) Fraction of Points Earned in Slams -

2020 Women’S Tennis Association Media Guide
2020 Women’s Tennis Association Media Guide © Copyright WTA 2020 All Rights Reserved. No portion of this book may be reproduced - electronically, mechanically or by any other means, including photocopying- without the written permission of the Women’s Tennis Association (WTA). Compiled by the Women’s Tennis Association (WTA) Communications Department WTA CEO: Steve Simon Editor-in-Chief: Kevin Fischer Assistant Editors: Chase Altieri, Amy Binder, Jessica Culbreath, Ellie Emerson, Katie Gardner, Estelle LaPorte, Adam Lincoln, Alex Prior, Teyva Sammet, Catherine Sneddon, Bryan Shapiro, Chris Whitmore, Yanyan Xu Cover Design: Henrique Ruiz, Tim Smith, Michael Taylor, Allison Biggs Graphic Design: Provations Group, Nicholasville, KY, USA Contributors: Mike Anders, Danny Champagne, Evan Charles, Crystal Christian, Grace Dowling, Sophia Eden, Ellie Emerson,Kelly Frey, Anne Hartman, Jill Hausler, Pete Holtermann, Ashley Keber, Peachy Kellmeyer, Christopher Kronk, Courtney McBride, Courtney Nguyen, Joan Pennello, Neil Robinson, Kathleen Stroia Photography: Getty Images (AFP, Bongarts), Action Images, GEPA Pictures, Ron Angle, Michael Baz, Matt May, Pascal Ratthe, Art Seitz, Chris Smith, Red Photographic, adidas, WTA WTA Corporate Headquarters 100 Second Avenue South Suite 1100-S St. Petersburg, FL 33701 +1.727.895.5000 2 Table of Contents GENERAL INFORMATION Women’s Tennis Association Story . 4-5 WTA Organizational Structure . 6 Steve Simon - WTA CEO & Chairman . 7 WTA Executive Team & Senior Management . 8 WTA Media Information . 9 WTA Personnel . 10-11 WTA Player Development . 12-13 WTA Coach Initiatives . 14 CALENDAR & TOURNAMENTS 2020 WTA Calendar . 16-17 WTA Premier Mandatory Profiles . 18 WTA Premier 5 Profiles . 19 WTA Finals & WTA Elite Trophy . 20 WTA Premier Events . 22-23 WTA International Events . -

The Lta Wild Card Policy
THE LTA WILD CARD POLICY 1. INTRODUCTION A ‘wild card’ is a player included in the draw of a tennis event at the discretion of the tournament’s organising committee or organisation. Both main draw and qualifying wild cards may be made available at events. Because the LTA runs and organises some tournaments (LTA Staged Tournaments), the LTA is able to allocate wild cards in the draws of the events within those tournaments. This policy is a general policy that explains how the LTA chooses the players which receive those wild cards and how the LTA nominates individuals to receive wild cards for The Junior Championships, Wimbledon from the All England Lawn Tennis and Croquet Club Limited (the AELTC). The number of wild cards that are available to the LTA at ITF World Tennis Tour (Men’s & Women’s), ATP and WTA tour level events held in Great Britain is outlined in appendix 1. Specific Tournaments and Events If you would like to learn about a particular tournament or event, you should read the relevant tournament information. For LTA tournaments, you can find tournament-specific information packs in the competition resources area of the LTA website. 2. WHAT THIS POLICY EXPLAINS This policy (the Policy) explains how the LTA will allocate wild cards for LTA Staged Tournaments and how the LTA chooses the individuals who they will nominate to the AELTC to receive wildcards for The Junior Championships, Wimbledon. Where references are made to allocating wildcards in this Policy, in relation to The Junior Championships, Wimbledon, such references shall mean nominating individuals for wildcards. -

Tournament Notes
TournamenT noTes as of march 31, 2010 THE RIVER HILLS USTA $25,000 WOMEN’S CHALLENGER JACKSON, MS • APRIL 4-11 USTA PRO CIRCUIT RETURNS TO JACKSON FOR 12TH STRAIGHT YEAR TournamenT InFormaTIon The River Hills USTA $25,000 Women’s Challenger is the 10th $25,000 women’s tournament of the year and the only $25,000 Site: River Hills Country Club – Jackson, Miss. women’s event held in Mississippi. Jackson Websites: www.riverhillsclub.net, is the second of three consecutive clay court procircuit.usta.com events on the USTA Pro Circuit in the lead-up to the 2010 French Open. Bryn Lennon/Getty Images Qualifying draw begins: Sunday, April 4 Main draw begins: Tuesday, April 6 This year’s main draw is expected to include Julia Cohen, an All-American at the University Main Draw: 32 Singles / 16 Doubles of Miami who reached the semifinals of the NCAA tournament as a sophomore in 2009, Surface: Clay / Outdoor Lauren Albanese, who won the 2006 USTA Prize Money: $25,000 Girls’ 18s National Championships to earn an automatic wild card into the US Open, and Tournament Director: Kimberly Couts, a frequent competitor on the Dave Randall, (601) 987-4417 USTA Pro Circuit who won the 2006 Easter Lauren Albanese won the 2006 USTA Girls’ [email protected] Bowl as a junior and was a former USTA Girls’ 18s National Championships to earn an 16s No. 1. automatic wild card into the US Open. Tournament Press Contact: Kendall Poole, (601) 987-4454 International players in the main draw include freshman in 2009 and led Duke University [email protected] -

Alexa Glatch, the Top-Seeded Player in the Field, Who Is on the Comeback Trail After an Prize Money: $10,000 Injury-Marred 2010
TournamenT noTes as of may 11, 2011 KOSER JEWELERS PRO CIRCUIT TENNIS CHALLENGE LANDISVILLE, PA • MAY 15-22 USTA PRO CIRCUIT WOMEN’S TENNIS RETURNS TO LANDISVILLE TournamenT InFormaTIon The Koser Jewelers Pro Circuit Tennis Challenge will be held in Landisville for the USTA fourth consecutive year. It is the first of three Site: Hempfield Recreation Center – Landisville, Pa. consecutive $10,000 hard court tournaments Websites: www.landisvilleprocircuit.com that take place during the spring season. procircuit.usta.com It is the only USTA Pro Circuit women’s event taking place in Pennsylvania. A men’s Qualifying Draw Begins: Sunday, May 15 $10,000 clay court event will take place in Main Draw Begins: Tuesday, May 17 Pittsburgh in July. Main Draw: 32 Singles / 16 Doubles This year’s main draw is expected to feature Surface: Hard / Outdoor Alexa Glatch, the top-seeded player in the field, who is on the comeback trail after an Prize Money: $10,000 injury-marred 2010. Glatch reached the Tournament Director: quarterfinals as a qualifier at the WTA event Alexa Glatch, the top-seeded player in the field, in Memphis, Tenn., in February 2011 and, in Wilson Pipkin, (717) 898-3102 ext. 31 reached the quarterfinals of the WTA event in 2009, propelled the United States to the Fed Memphis, Tenn., in February, as a qualifier, and [email protected] Cup final by winning two of the U.S. team’s propelled the United States to the 2009 Fed Tournament Press Contact: three points in the semifinals against the Cup final by winning two of the U.S. -
And Type in Recipient's Full Name
18 March 2020 ATP AND WTA EXTEND SUSPENSION OF TOURS After careful consideration, and due to the continuing outbreak of COVID-19, all ATP and WTA tournaments in the Spring clay-court swing will not be held as scheduled. This includes the combined ATP/WTA tournaments in Madrid and Rome, along with the WTA events in Strasbourg and Rabat and ATP events in Munich, Estoril, Geneva and Lyon. The professional tennis season is now suspended through 7 June 2020, including the ATP Challenger Tour and ITF World Tennis Tour. At this time, tournaments taking place from 8 June 2020 onwards are still planning to go ahead as per the published schedule. In parallel, the FedEx ATP Rankings and WTA Rankings will be frozen throughout this period and until further notice. The challenges presented by the COVID-19 pandemic to professional tennis demand greater collaboration than ever from everyone in the tennis community in order for the sport to move forward collectively in the best interest of players, tournaments and fans. We are assessing all options related to preserving and maximising the tennis calendar based on various different return dates for the Tours, which remains an unknown at this time. We are committed to working through these matters with our player and tournament members, and the other governing bodies, in the weeks and months ahead. Now is not a time to act unilaterally, but in unison. All decisions related to the impact of the coronavirus require appropriate consultation and review with the stakeholders in the game, a view that is shared by ATP, WTA, ITF, AELTC, Tennis Australia, and USTA. -

2018 Coverage
2018 coverage Unrivalled highlights coverage sntv offers more cleared highlights from a wider range of sports than anyone else, offering the greatest breadth of sports coverage worldwide. Videos that inform and engage We provide our clients with the most relevant and engaging videos, either fully customisable or ready to publish directly to your audience. Global and regional sports video news Our dedicated teams fully understand what our clients are looking for, and recognise what content will drive conversations on both an international and regional level. January February March April May soccer soccer american football soccer baseball AFC Champions League Superbowl LII Chinese Super League MLB Season FA Cup Final Jan - Nov Feb Mar - Nov Apr - Oct May Copa Libertadores J.League UEFA Champions Jan - Nov rugby Mar - Dec basketball League Final RBS Six Nations NBA Playoffs May tennis Championship golf Apr - May UEFA Europa League Final ATP World Tour Feb - Mar ANA Inspiration May Jan - Nov Mar - Apr american football UEFA Women’s Champions Australian Open soccer NFL Draft League Final Jan EFL Cup Final baseball Apr May Davis Cup Feb MLB Spring Training Jan - Nov Mar ice hockey tennis Hopman Cup tennis NHL Playoffs French Open Jan Fed Cup motorsport Apr - Jun May - Jun WTA Tour Feb - Nov Jan - Oct Formula One Mar - Nov golf basketball golf golf Moto GP The Masters NBA Finals Apr European Tour Asian Tour Mar - Aug May - Jun Feb - Dec Jan - Nov MXGP Ladies European Tour motorsport golf LPGA Tour Mar - Oct Feb - Dec World Touring Car Players -

Main Draw & Qualifying Player Entry Information
Main Draw & Qualifying Player Entry Information 2016 US OPEN | MAIN DRAW & QUALIFYING PLAYER ENTRY INFORMATION AUGUST 29 - SEPTEMBER 11 2016 US Open Tennis Championships Entry Deadlines Draws August 29 – September 11 Men’s and women’s singles main draws will be conducted Men’s Singles Monday, July 18 Main Draw: on Friday, August 26. (Exact location to be determined.) USTA Billie Jean King National Tennis Center Women’s Singles Monday, July 18 Flushing Meadows-Corona Park Main Draw: Regulations Governing Play Flushing, NY Men’s Singles Qualifying: Monday, August 1 The Rules of Tennis and the Rules, Regulations and Code of the Grand Slam Board govern men’s and women’s singles and Presented by the Women’s Singles Qualifying: Monday, August 1 doubles play. UNITED STATES TENNIS ASSOCIATION Entry for men’s doubles will begin Men’s Doubles Monday, August 1, and close Friday, Men’s Singles Championship Main Draw*: The US Open Junior Tennis Championships uses a separate Women’s Singles Championship August 19, at 12 pm entry form that is available via the Players Only web page Entry for women’s doubles will begin Men’s Doubles Championship Women’s Doubles (USOpen.org/playersonly). Monday, August 1, and close Friday, Women’s Doubles Championship Main Draw*: August 19, at 12 pm Scoring Mixed Doubles Championship By sign-in only from Monday, All men’s singles main draw matches will be the best-of-five tie-break Mixed Doubles August 22, at 12 pm until sets. All men’s and women’s doubles matches, as well as women’s Katrina M. -

2021 Official Rulebook
Chris Evert WTA World No.1 Singles Trophy 2021 official rulebook 2021 Official Rulebook Copyright 2021 WTA Tour, Inc. All Rights Reserved WTA and WTA Tour are registered trademarks of WTA Tour, Inc. Printed in the United States of America TABLE OF CONTENTS I. INTRODUCTION 5 A. DESCRIPTION 5 B. ADMINISTRATION 5 C. RULES 5 D. POLICIES 6 II. PLAYER COMMITMENT, BONUS POOL, TOP 10 PLAYER DELIVERY 7 A. SINGLES COMMITMENT TOURNAMENTS 7 B. BONUS POOL 11 C. TOP 10 PLAYER DELIVERY 13 D. BONUS POOL FUND 15 III. TOURNAMENT ENTRY, TOURNAMENT ACCEPTANCE, AND WILD CARDS 17 A. TOURNAMENT ENTRY 17 B. TOURNAMENT ACCEPTANCE 25 C. WILD CARDS 33 IV. WITHDRAWALS AND RETIREMENTS 43 A. WITHDRAWALS 43 B. RETIREMENTS 54 C. RESTRICTIONS, EXCEPTIONS, AND PROCEDURES 54 V. TOURNAMENT DRAWS AND SCHEDULING 57 A. DRAWS 57 B. SCHEDULING 78 VI. WTA FINALS AND WTA ELITE TROPHY 85 A. PORSCHE RACE TO SHENZHEN 85 B. WTA FINALS 85 C. WTA ELITE TROPHY 95 VII. PLAYER RESPONSIBILITIES/ON-COURT RULES AND PROCEDURES 111 A. ACES PROGRAM 111 B. MEDIA/SPONSOR/PUBLIC RELATIONS RESPONSIBILITIES 119 C. CLOTHING AND EQUIPMENT 127 D. TOILET/CHANGE OF ATTIRE BREAKS 136 1 TABLE OF CONTENTS E. WTA MEDICAL RULE 138 F. CODE OF CONDUCT 138 G. CONTINUOUS PLAY 138 H. HINDRANCE RULE 139 I. COURT ETIQUETTE 140 J. DEFAULTS 140 K. FINE APPEALS 141 VIII. WTA RANKING SYSTEM 143 A. GENERAL 143 B. RULES AND PROCEDURES 149 C. WTA SPECIAL RANKING RULE 153 D. RETIRING FROM THE WTA 165 IX. PRIZE MONEY 167 A. DISTRIBUTION 167 B. AMATEURISM 169 C. -

Newsroom 24 August 2021
Newsroom 24 August 2021 Porsche Brand Ambassador impresses at the WTA 1000 tournament in Cincinnati Angelique Kerber in good form going into the US Open Stuttgart. Angelique Kerber is ready for the US Open. With just over a week to go before the start of the grand slam in New York, the in-form Porsche Brand Ambassador was highly impressive at the Western & Southern Open in Cincinnati when reaching the semifinals. “It was a great week with tight matches against tough opponents. I felt really good after my break and was able to produce my best tennis over longer stretches,” said a visibly satisfied Angelique Kerber when reviewing her performance. “The tournament is fantastic preparation for the US Open. I’ll be travelling to New York with a good feeling.” Within the scope of its worldwide engagement in women’s tennis, Porsche supports the WTA 1000 tournament in Cincinnati together with Porsche Cars North America as the official automotive partner. For Angelique Kerber, the event in the state of Ohio was a real test ahead of the US Open, the year’s fourth grand slam that begins on 30 August. On her return to the WTA Tour after the break for the Olympics, the 33-year old German faced strong opponents right from the first round. They included two Top 10 players and two in the Top 20. Her opening match pitted her against the Greek Maria Sakkari (No. 18), the French Open semifinalist, and she started her campaign at the hard-court tournament in the Midwest with a straight-sets 6-2, 6-2 win. -

Brooksby, Nakashima, Tiafoe Added to Men's Field; Pera, Stosur, Teichmann Awarded Women's Wild Cards
Brooksby, Nakashima, Tiafoe Added To Men’s Field; Pera, Stosur, Teichmann Awarded Women’s Wild Cards Kenin, Williams Sisters Withdraw From Western & Southern Open CINCINNATI (Aug. 10, 2021) – Americans Jenson Brooksby, Brandon Nakashima and Frances Tiafoe have been awarded men’s wild cards for the 2021 Western & Southern Open. In addition, Bernada Pera, Samantha Stosur and Jil Teichmann have received wild cards into the women’s field. Three players have withdrawn from the women’s field – Sofia Kenin (foot), Serena Williams (leg) and Venus Williams. With a scorching 2021 season, Brooksby has climbed into the Top 100 of the ATP rankings for the first time in his career. Brooksby reached his first ATP final just last month in Newport, becoming the second-youngest player to reach the final in the 45-year tournament history. Brooksby collected his first win over a top 20 opponent (Felix Auger-Aliassime) in Washington D.C. last week to advance to his first semifinal in an ATP 500 event. The 20-year-old, who will be making his Cincinnati debut, has also snagged his first three career ATP Challenger Tour titles in 2021, including back-to-back wins in consecutive weeks in April. Finishing as a finalist in two of his last three events in Los Cabos and Atlanta, Nakashima jumped to a career-high ranking of 87. Nakashima, who will be making his second consecutive appearance in Cincinnati, became the youngest American to reach an ATP final since Taylor Fritz reached the Memphis Open final in 2016. The 20-year-old has won 65 percent of his matches on the ATP Tour and Majors in his career, winning two titles on the ATP Challenger Tour along with two ITF titles in the process. -
Miami Open Presented by Itau
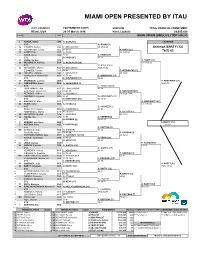
MIAMI OPEN PRESENTED BY ITAU CITY, COUNTRY TOURNAMENT DATES SURFACE TOTAL FINANCIAL COMMITMENT Miami, USA 20-31 March 2019 Hard, Laykold $9,035,428 STATUS NAT MAIN DRAW SINGLES (TOP HALF) 1 1 OSAKA, Naomi JPN N. OSAKA [1] CHAMPION 2 BYE N. OSAKA [1] 3 Q VICKERY, Sachia USA Y. WICKMAYER 60 67(3) 61 Ashleigh BARTY [12] 4 Q WICKMAYER, Yanina BEL 36 63 61 S. HSIEH [27] 76(1) 63 5 Q KANEPI, Kaia EST A. RISKE 46 76(4) 63 6 RISKE, Alison USA 62 62 S. HSIEH [27] 7 BYE S. HSIEH [27] 62 75 8 27 HSIEH, Su-Wei TPE S. HSIEH [27] 9 20 MUGURUZA, Garbiñe ESP G. MUGURUZA [20] 63 67(0) 62 10 BYE M. NICULESCU 11 Q NICULESCU, Monica ROU M. NICULESCU 76(0) 46 62 12 ZIDANSEK, Tamara SLO 61 62 C. WOZNIACKI [13] 13 Q GOLUBIC, Viktorija SUI A. SASNOVICH 64 76(4) 14 SASNOVICH, Aliaksandra BLR 46 75 64 C. WOZNIACKI [13] 15 BYE C. WOZNIACKI [13] 64 64 16 13 WOZNIACKI, Caroline DEN A. KONTAVEIT [21] 17 9 SABALENKA, Aryna BLR A. SABALENKA [9] 36 62 75 18 BYE A. TOMLJANOVIC 19 TOMLJANOVIC, Ajla AUS A. TOMLJANOVIC 63 64 20 FRIEDSAM, Anna-Lena GER 46 63 60 A. KONTAVEIT [21] 21 PETKOVIC, Andrea GER A. ANISIMOVA 76(3) 26 76(4) 22 ANISIMOVA, Amanda USA 64 63 A. KONTAVEIT [21] 23 BYE A. KONTAVEIT [21] 63 16 64 24 21 KONTAVEIT, Anett EST A. KONTAVEIT [21] 25 32 KENIN, Sofia USA S. KENIN [32] 61 20 Ret'd 26 BYE B.